Cerebrospinal Fluid (CSF) - Complete Reference
Sources: Harrison's 22E (2025) | Adams & Victor's Neurology 12E | Bailey & Love 28E | Costanzo Physiology 7E | Recent Guidelines
1. ANATOMY
Ventricular System and CSF Spaces
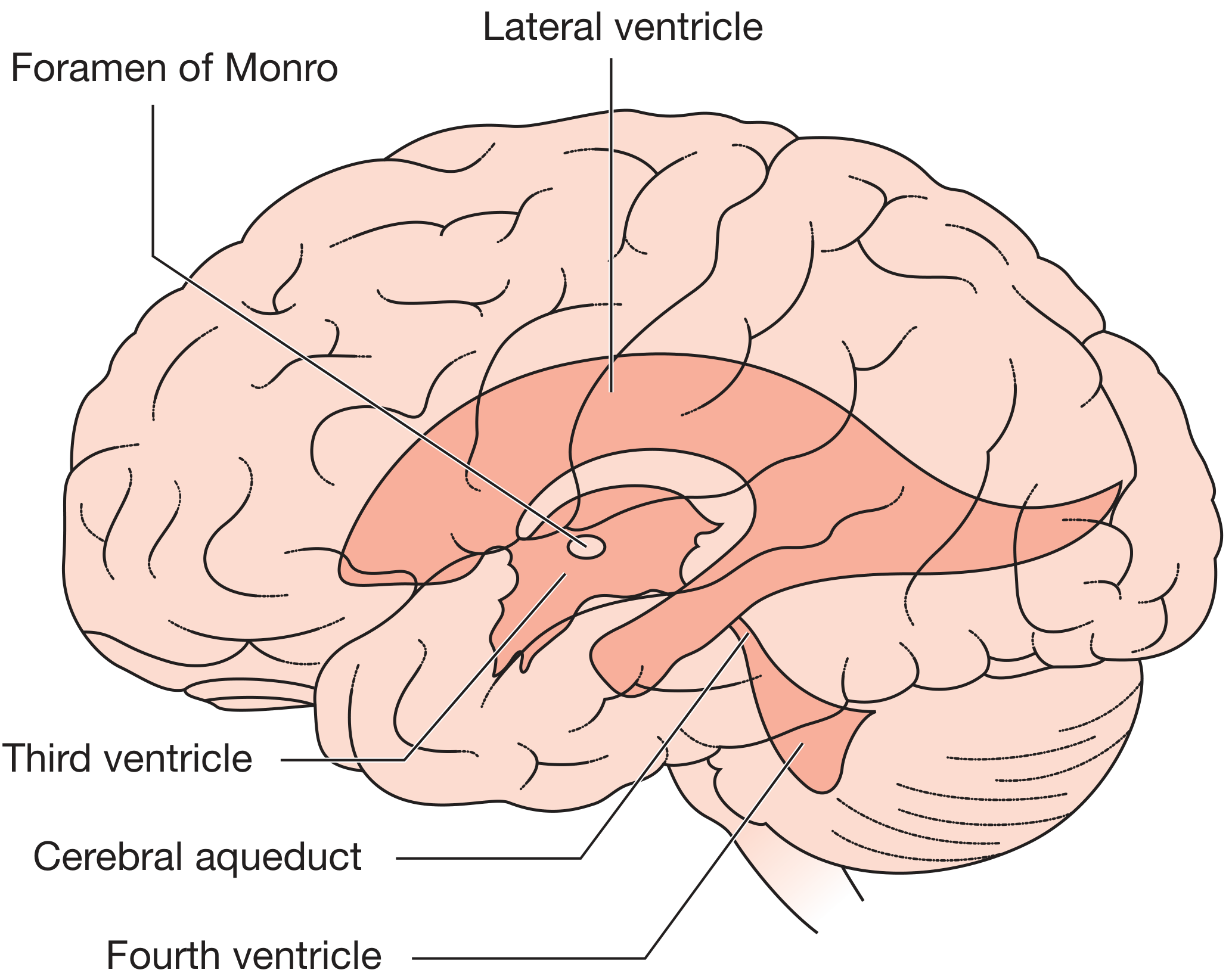
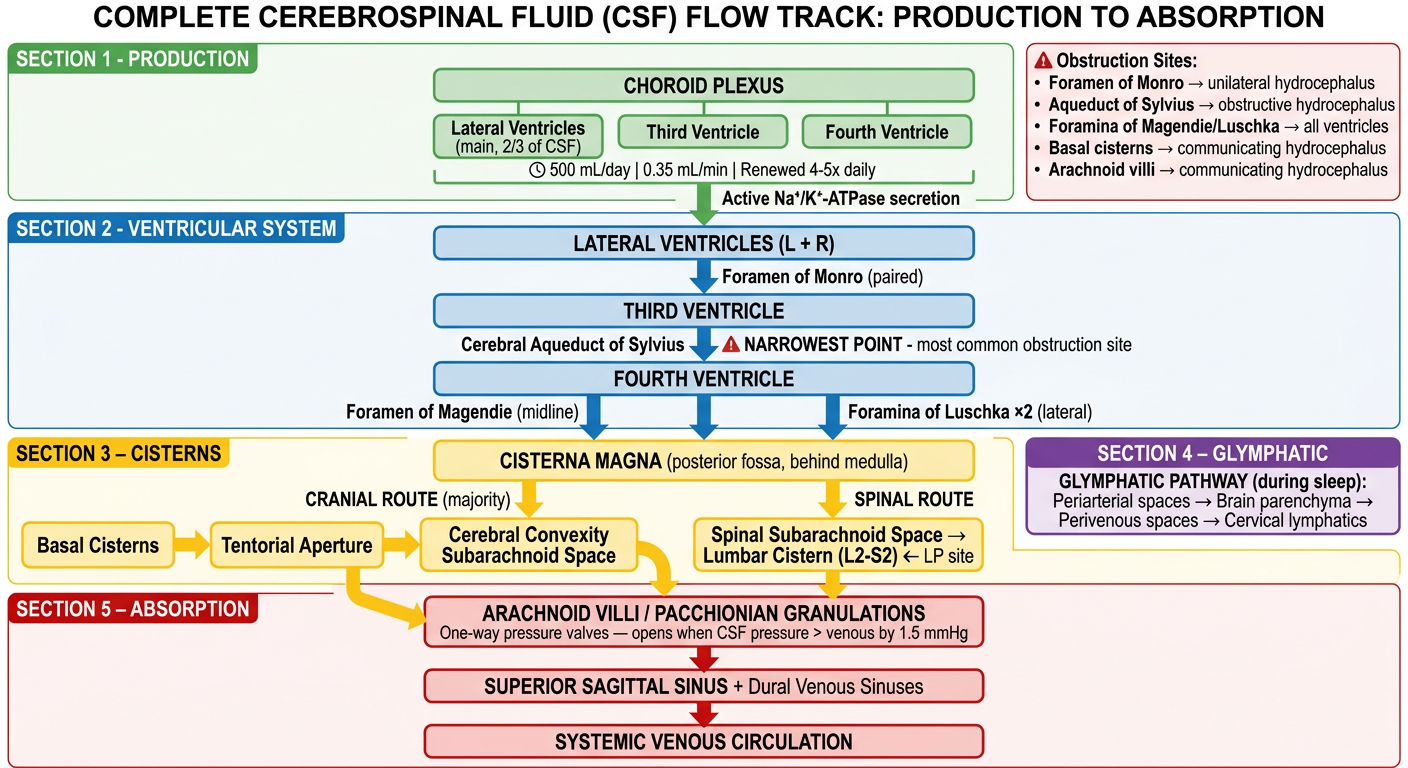
CSF resides in two main compartments: the ventricular system and the subarachnoid space. The ventricular system consists of:
- Two lateral ventricles (one in each cerebral hemisphere)
- Third ventricle (diencephalon, midline)
- Cerebral aqueduct of Sylvius (connecting 3rd to 4th ventricle - the narrowest point, most common site of obstruction)
- Fourth ventricle (between pons/medulla and cerebellum)
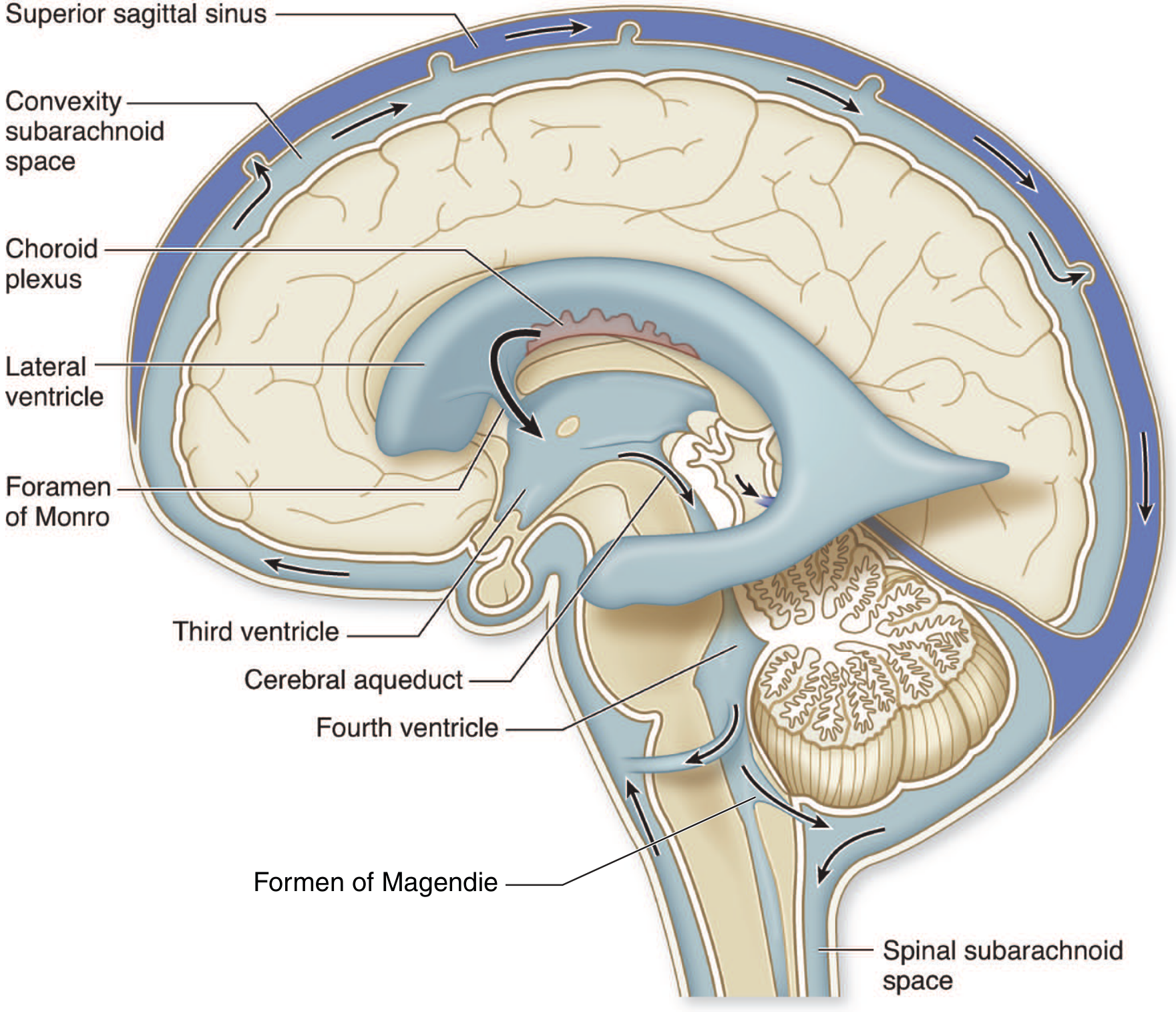
CSF exits the fourth ventricle via:
- Foramen of Magendie (single, midline)
- Foramina of Luschka (paired, lateral)
...into the subarachnoid space, which envelops the entire brain and spinal cord. Distended regions of the subarachnoid space form cisterns (cisterna magna, pontine cistern, interpeduncular cistern, etc.).
CSF flows: Lateral ventricles → Foramen of Monro → Third ventricle → Aqueduct of Sylvius → Fourth ventricle → Foramina of Magendie and Luschka → Subarachnoid space → Arachnoid villi → Superior sagittal sinus (venous return).
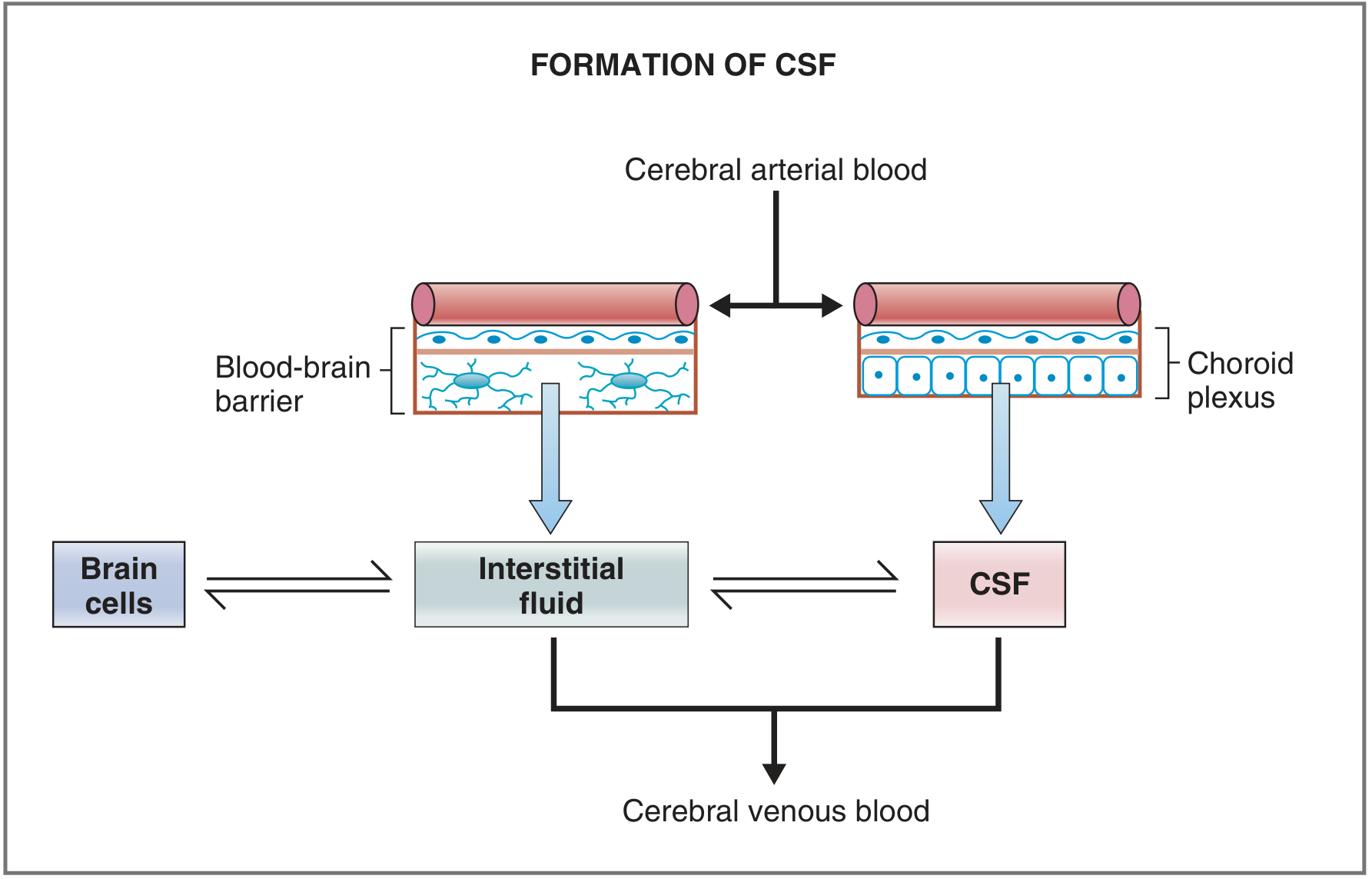
Blood-Brain Barrier and Choroid Plexus
The choroid plexus is the primary site of CSF formation, located in the floor of the lateral ventricles, the roof of the third ventricle, and the roof of the fourth ventricle. The barrier between cerebral capillary blood and CSF is the choroid plexus itself, consisting of three layers:
- Capillary endothelial cells and basement membrane
- Neuroglial membrane
- Epithelial cells of the choroid plexus (functionally analogous to renal distal tubule cells)
The blood-brain barrier (BBB) separates capillary blood from brain interstitial fluid. It differs from other tissue barriers in two critical ways:
-
Tight junctions between endothelial cells prevent paracellular passage
-
Only lipid-soluble substances (O2, CO2, most drugs with log P > 0) cross freely; water-soluble substances are excluded
-
Costanzo Physiology 7E, p. 119
2. PHYSIOLOGY
Formation
CSF is formed by active secretion and filtration at the choroid plexus. The epithelial cells:
- Secrete INTO CSF: Na+, Cl-, HCO3-, and water
- Absorb FROM CSF into blood: K+
- Exclude: Protein, cholesterol (large molecular size)
Rate of formation: 21-22 mL/hour (0.35 mL/min), approximately 500 mL/day
- The entire CSF volume is renewed 4-5 times daily
- Adams & Victor, p. 629 | Costanzo, p. 119
Volume
| Parameter | Value |
|---|
| Total CSF volume (adult) | 70-160 mL (mean ~104 mL intracranial + 10-25 mL spinal) |
| Brain volume | 1,200-1,400 mL |
| Total intracranial volume | ~1,700 mL |
| CSF as fraction of intracranial contents | <10% |
| Production rate | 500 mL/day (0.35 mL/min) |
Composition (Normal Values)
| Component | CSF | Blood | Relationship |
|---|
| Na+ | ~138 mEq/L | ~138 mEq/L | Equal |
| Cl- | ~119 mEq/L | ~102 mEq/L | Higher in CSF |
| HCO3- | ~22 mEq/L | ~24 mEq/L | ~Equal |
| K+ | ~2.8 mEq/L | ~4.5 mEq/L | Lower in CSF |
| Ca2+ | ~2.1 mEq/L | ~4.7 mEq/L | Lower in CSF |
| Mg2+ | ~2.2 mEq/L | ~1.7 mEq/L | Higher in CSF |
| Glucose | 45-80 mg/dL (60-70% of blood) | 70-110 mg/dL | Lower in CSF |
| Protein | 15-45 mg/dL | ~7,000 mg/dL | Much lower in CSF |
| Cells (WBC) | 0-5 lymphocytes/mm³ | - | Near acellular |
| pH | ~7.33 | ~7.41 | Slightly lower |
| Opening pressure (lateral decubitus) | 80-200 mm H2O (6-15 mmHg) | - | - |
| Osmolarity | ~295 mOsm/L | ~295 mOsm/L | Equal |
| Appearance | Clear, colorless ("crystal clear") | - | - |
- Costanzo 7E, Table 3.6 | Adams & Victor, p. 629-631
Absorption
Absorption occurs primarily via arachnoid villi (arachnoid granulations), projections into the dural venous sinuses (especially the superior sagittal sinus), functioning as one-way pressure valves. CSF passes through at a linearly increasing rate when CSF pressure rises above 68 mm H2O. Additionally, mesothelial cells of arachnoid villi form giant vacuoles for transcellular bulk transport. Some substances (penicillin, organic acids/bases) are also absorbed by choroid plexus cells.
CSF Pressure Dynamics (Monroe-Kellie Doctrine)
The Monro-Kellie doctrine states that the total intracranial volume (brain + blood + CSF) is fixed within the rigid skull. Any increase in one component must be compensated by a decrease in another.
CSF Pressure Equation (from Adams & Victor):
PCSF = Pv + If × R0
Where Pv = venous pressure, If = CSF flow rate (normally = production rate = 0.3 mL/min), R0 = resistance to absorption (~2.5 mm Hg/mL/min normally). The product If × R0 is only ~0.8 mmHg normally, so CSF pressure is predominantly determined by venous pressure.
Normal ICP (recumbent adult): 8 mmHg (110 mm H2O). Values above 15 mmHg are considered abnormal. Arterial hypertension alone rarely raises ICP due to cerebrovascular autoregulation; however, raised venous pressure (heart failure, jugular/superior mediastinal obstruction, sinus thrombosis) directly elevates ICP.
- Adams & Victor, p. 631 | Bailey & Love, p. 8417-8423
Functions of CSF
- Mechanical cushioning - The 1,500-g brain weighs only ~50 g when suspended in CSF (buoyancy effect), protecting against trauma and acute venous pressure changes
- Metabolic waste removal ("sink action") - Clears CO2, lactate, H+, and metabolic by-products; substitute for lymphatics (the brain has no lymphatics)
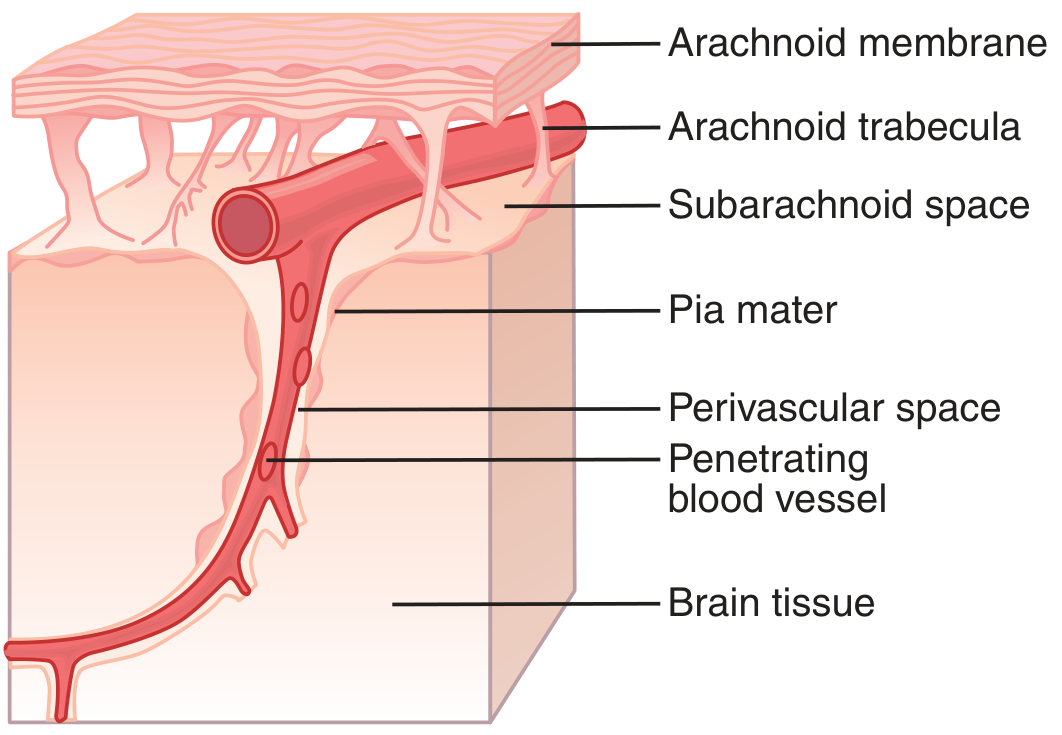
- Glymphatic system - A glial-dependent perivascular network (astrocyte endfeet bounding periarterial spaces = Virchow-Robin spaces) drives bulk flow of solutes toward deep veins and cervical lymphatics. Active mainly during sleep. Implicated in clearance of neurodegenerative proteins (amyloid-beta, tau). Most data from animal models but garnering intense clinical interest.
- Chemical homeostasis - Maintains stable ionic environment for neurons, astrocytes, and nerve fibers; resists major alterations in blood composition
- Drug/toxin exclusion - The BBB and choroid plexus prevent most water-soluble toxins and pathogens from entering neural tissue
- Neurotransmitter containment - May prevent escape of local neurotransmitters into general circulation
- Adams & Victor, p. 629 | Costanzo 7E, p. 120
3. PATHOPHYSIOLOGY
Raised Intracranial Pressure
ICP > 15 mmHg is abnormal. The five major mechanisms (Adams & Victor):
| Mechanism | Examples |
|---|
| 1. Focal mass | Brain tumor, hematoma (extradural/subdural/intracerebral), abscess, contusion |
| 2. Generalized brain swelling | Ischemic-anoxic injury, acute hepatic failure, hypertensive encephalopathy, hypercarbia, Reye syndrome |
| 3. Raised venous pressure | Cerebral venous sinus thrombosis, heart failure, superior mediastinal/jugular obstruction |
| 4. Obstruction to CSF flow/absorption | Hydrocephalus (obstructive or communicating), meningitis, carcinomatous meningitis, subarachnoid hemorrhage |
| 5. Expanded CSF volume/production | Meningitis, SAH, choroid plexus tumor |
Clinical features of raised ICP: Headache (worse in morning, Valsalva, lying flat), nausea/vomiting, drowsiness, abducens (VI) palsy (false localizing sign), papilledema. In infants: increasing head circumference, bulging fontanelle, "setting sun" sign.
Cerebral perfusion pressure (CPP) = MAP - ICP. Adequate cerebral perfusion can be maintained at ICP up to 40 mmHg if BP is normal. Below mean BP ~40 mmHg, autoregulation fails.
Cushing's triad (late sign of herniation): hypertension + bradycardia + irregular breathing. These result from brainstem displacement, NOT from raised pressure per se.
- Adams & Victor, p. 633-634 | Bailey & Love, p. 8395-8423
Hydrocephalus
Hydrocephalus = ventricular enlargement due to obstruction of normal CSF flow.
Classification (Dandy-Blackfan, 1914):
| Type | Mechanism | Key Feature |
|---|
| Obstructive (non-communicating) | Blockage within ventricular system | Dye injected in ventricle does NOT appear in lumbar CSF |
| Communicating | Block at arachnoid villi/convexity subarachnoid space (post-formation) | Dye communicates freely between compartments |
| Ex vacuo | Cerebral atrophy; ventricles expand passively | Not true hydrocephalus - no pressure rise |
| Normal pressure hydrocephalus (NPH) | Communicating; intermittent pressure rises but mean ICP is normal | Classic triad: wet, wacky, wobbly |
Ayer's Rule (Adams & Victor): The ventricle closest to the obstruction enlarges the most.
- Foramen of Monro obstruction → one lateral ventricle enlarges
- Aqueduct obstruction → both lateral + third ventricle enlarge
- Outlet foramina (Magendie/Luschka) obstruction → all ventricles enlarge
- Basal cistern block → disproportionate fourth ventricle enlargement
Aetiology of hydrocephalus (Bailey & Love Table 48.1):
- Obstructive: lesions within ventricle (ependymoma, colloid cyst), in ventricular wall (periventricular tumor), or compressing from outside
- Communicating: post-haemorrhagic (SAH, IVH), CSF infection (meningitis), raised CSF protein
- Excessive production (rare): choroid plexus papilloma/carcinoma
Risk of LP in obstructive hydrocephalus: Dangerous - differential pressure changes can cause tonsillar/cerebellar herniation ("coning"). LP is relatively safe in communicating hydrocephalus and may be therapeutic (pseudotumor cerebri, SAH).
- Bailey & Love, p. 725 | Adams & Victor, p. 633-636
4. DISEASES ASSOCIATED WITH CSF - DIAGNOSTIC PATTERNS
Characteristic CSF Formulas (Adams & Victor, Table 2-1)
| Condition | Cells | Protein | Glucose | Other |
|---|
| Bacterial meningitis | WBC >50/mm³, often greatly increased (PMN predominant) | 100-250 mg/dL | 20-50 mg/dL; usually <½ blood glucose | Gram stain positive; pressure increased |
| Viral/fungal/spirochetal | WBC 10-100/mm³ (lymphocyte predominant) | 50-200 mg/dL | Normal or slightly reduced | Special cultures; normal or slightly raised pressure |
| Tuberculous meningitis | WBC >25/mm³ (lymphocyte predominant) | 100-1,000 mg/dL | <50 mg/dL, often markedly reduced | Special culture + PCR; AFB smear |
| Subarachnoid hemorrhage | RBC >500/mm³; slight WBC increase | 60-150 mg/dL | Normal | Xanthochromia (after 2-4 hrs); pressure raised |
| Brain tumor / carcinomatous meningitis | Normal or slight lymphocytes | 50-200 mg/dL | Normal or low | Cytology; flow cytometry; raised pressure |
| Multiple sclerosis | 6-20 lymphocytes (mild pleocytosis in ~1/3) | Normal or mildly elevated (<100 mg/dL) | Normal | OCBs in >90%; IgG index raised |
| Normal pressure hydrocephalus | Normal | Normal or mildly elevated | Normal | Pressure normal (or intermittently raised) |
5. SPECIFIC DISEASE-CSF CORRELATIONS
Bacterial Meningitis (Harrison's 22E, 2025)
Key CSF tests per Harrison's:
- Pressure: measured at LP; elevated
- Bacterial culture + Gram stain (definitive)
- Cell count and differential: neutrophilic pleocytosis
- Glucose and protein
- VDRL (for syphilis - highly specific, not sensitive)
- India ink / cryptococcal antigen (fungal)
- PCR for organisms (16s rRNA for bacteria, 18s/28s rRNA for fungi, specific viral PCRs)
- Metagenomic next-generation sequencing (mNGS) - increasingly available; powerful for challenging/partially treated cases
- Beta-glucan assay - useful adjunct when other tests negative for fungal infection
- CSF VDRL negative in high-risk patient with positive treponemal serum Ab + unexplained pleocytosis → empiric neurosyphilis treatment still appropriate
When neutrophils predominate after 3 weeks of "meningitis," consider: Nocardia, Actinomyces, Brucella, M. tuberculosis (early), Blastomyces, Candida, Histoplasma, Aspergillus, SLE, chemical meningitis.
When eosinophils are present: parasitic (Angiostrongylus, Gnathostoma, Baylisascaris, Toxocara, cysticercosis), fungal (coccidioidal), neoplastic (lymphoma, leukemia), inflammatory (sarcoidosis, hypereosinophilic syndrome).
Multiple Sclerosis (Harrison's 22E | Adams & Victor)
-
Mild lymphocytic pleocytosis (>5 cells/µL) in ~25% of cases
-
Oligoclonal bands (OCBs): 2+ bands in >90% of MS patients; negative in serum-paired sample
-
IgG index = (CSF IgG/CSF albumin) / (Serum IgG/Serum albumin) - elevated >0.7 indicates intrathecal IgG synthesis
-
IgG synthesis rate (formula using serum + CSF IgG and albumin)
-
CSF protein: usually normal or mildly elevated; >100 mg/dL argues against MS
-
Pleocytosis >75/µL, PMN cells, or protein >100 mg/dL → reconsider MS diagnosis
-
MBP (myelin basic protein): elevated during acute exacerbations; not specific (any demyelination raises it)
-
OCBs also in: syphilis, Lyme, SSPE, NMO (generally lack OCBs in NMO)
-
Harrison's 22E, p. 3627 | Adams & Victor, p. 353-358
Subarachnoid Hemorrhage (Adams & Victor)
-
CSF becomes grossly bloody within 30 minutes of SAH
-
After 2-4 hours: xanthochromia develops (yellow discoloration from bilirubin from RBC breakdown)
-
Xanthochromia distinguishes true SAH from traumatic tap
-
Delayed communicating hydrocephalus may appear 2-4 weeks later due to blockage of CSF pathways by blood/fibrosis
-
Pressure raised; RBC >500/mm³
-
Adams & Victor, p. 484-485
Chronic Meningitis (Harrison's 22E)
When mononuclear cells predominate in chronic meningitis:
-
Repeated samples (3 or more) of large volumes of lumbar CSF may be needed
-
Cell block cytology and flow cytometry for malignant cells (lymphoma, carcinoma)
-
Large volumes needed for culture sediment in fungal meningitis
-
If standard LP unrewarding: cervical cisternal tap to sample near basal meninges
-
Carcinomatous meningitis: elevated protein nearly always present; cytology may need multiple samples
-
Harrison's 22E, p. 1177-1178
Normal Pressure Hydrocephalus (NPH)
Classic triad (Hakim-Adams triad): gait apraxia + urinary incontinence + dementia ("wet, wobbly, wacky")
- CSF pressure is "normal" by definition (<200 mm H2O on LP) but may show intermittent rises on continuous monitoring
- Communicating hydrocephalus on imaging (all ventricles enlarged)
- CSF tap test: drainage of 30-50 mL CSF → temporary improvement in gait (positive predictive)
- Treatment: CSF shunting (ventriculoperitoneal or ventriculoatrial shunt)
- Cochrane 2024 systematic review on shunting for iNPH (PMID: 39105473)
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri)
- Raised ICP without mass, hydrocephalus, or identifiable cause
- CSF pressure > 250 mm H2O (obese women of childbearing age most commonly affected)
- Normal CSF composition
- Papilledema, headache, visual obscurations, pulsatile tinnitus, CN VI palsy
- Risk of progressive visual loss
- Treatment: weight loss, acetazolamide, serial LPs, CSF shunting, optic nerve sheath fenestration, venous sinus stenting
- 2024 meta-analysis on venous sinus stenting for IIH (PMID: 38457956)
Neurodegenerative Diseases - CSF Biomarkers (Recent Updates 2023-2026)
This is a rapidly evolving field:
| Biomarker | Disease | Significance |
|---|
| Amyloid-beta 42 (Aβ42) | Alzheimer's disease | Decreased in CSF (deposits in plaques) |
| Tau (total tau) | Neurodegeneration | Elevated reflects neuronal damage |
| Phospho-tau (p-tau 181, 217, 231) | Alzheimer's disease | Elevated; reflects tangle pathology |
| Aβ42/Aβ40 ratio | Alzheimer's | More robust than Aβ42 alone |
| NfL (neurofilament light chain) | Non-specific neurodegeneration | Reflects axonal injury |
| 14-3-3 protein | Prion disease (CJD) | Classic CSF marker |
| Alpha-synuclein (seeding amplification assay, SAA) | Parkinson's / DLB | Highly sensitive/specific |
| GFAP | Astrocytic injury | Various |
The
Alzheimer's Association 2025 Practice Guideline (PMID: 40729527) on blood-based biomarkers now recommends plasma p-tau217 as the primary screening tool in specialized care, potentially replacing or complementing CSF AD biomarkers in many scenarios. However, CSF remains gold standard for confirmation in ambiguous cases.
6. LUMBAR PUNCTURE - TECHNIQUE & INTERPRETATION
Indications (Adams & Victor)
- Measurement of CSF pressure
- Diagnosis of CNS infection, SAH, inflammatory/demyelinating disease
- Instillation of anesthetics, antibiotics, antitumor agents
- Myelography (radiopaque contrast)
- Therapeutic drainage (IIH, NPH tap test)
Contraindications
- Absolute: Raised ICP with suspected mass lesion, asymmetric herniation risk, infections at LP site, uncorrected coagulopathy
- Relative: Anticoagulation (LP safe if INR ≤1.4, platelets >50,000/mm³, conventional aspirin doses acceptable)
Xanthochromia vs. Traumatic Tap
- Traumatic tap: blood is most concentrated in tube 1 and clears in subsequent tubes; no xanthochromia
- SAH: uniform blood in all tubes; xanthochromia appears 2-4 hours after ictus and persists up to 2 weeks; this distinction is the primary reason LP is done even when CT is negative in suspected SAH
7. PEDIATRIC CONSIDERATIONS
(Note: OP Ghai and Nelson's were not available in the library; the following integrates standard pediatric data from Adams & Victor and Harrison's)
Normal CSF values differ in neonates and infants:
| Parameter | Neonate | 1-3 months | >3 months |
|---|
| WBC | 0-30/mm³ (can be up to 30 in term) | 0-10/mm³ | 0-5/mm³ |
| Protein | Up to 120-150 mg/dL | 40-100 mg/dL | 15-45 mg/dL |
| Glucose | >50% blood glucose | >50% blood glucose | >50% blood glucose |
| Opening pressure | Varies with age; higher upper limit in children | | |
Upper limit of normal ICP is higher in children than adults (recumbent). In infants with unfused sutures, the cranium is compliant and can expand, allowing head circumference to increase as a manifestation of hydrocephalus without necessarily raising ICP in the early stages.
Pediatric meningitis CSF biomarkers - A
2025 Cochrane-level systematic review (PMID: 39672463) evaluated multiple CSF biomarkers in pediatric bacterial meningitis, confirming that CSF lactate, procalcitonin, and cytokines enhance diagnosis alongside classic WBC/protein/glucose parameters. A
2025 meta-analysis on cytokine profiles in pediatric meningitis (PMID: 39784111) showed IL-6, IL-10, and TNF-alpha significantly associated with outcomes.
8. SURGICAL (BAILEY & LOVE) PERSPECTIVE
Monro-Kellie Doctrine and Surgical Implications
The rigid intracranial compartment initially accommodates expanding mass lesions by excluding venous blood and CSF (compensatory phase). Once compensation is exhausted, even small volume increases cause sharp ICP rises (exponential pressure-volume curve).
Emergency CSF diversion (Bailey & Love) includes:
- External ventricular drain (EVD)
- Ventriculoperitoneal (VP) shunt
- Lumboperitoneal shunt
- Endoscopic third ventriculostomy (ETV) - preferred for aqueductal stenosis
- Drainage of 10-30 mL CSF can temporarily relieve hydrocephalus
CSF Rhinorrhoea
When frontal sinus fractures combine with a dural tear, CSF rhinorrhoea occurs. Confirmed by sending fluid for beta-2 transferrin assay (CSF-specific glycoprotein; not present in nasal secretions).
- Bailey & Love, p. 3915-3933
Choroid Plexus Tumors
Choroid plexus papillomas (WHO grade I) overproduce CSF and can cause communicating hydrocephalus. Choroid plexus carcinomas (WHO grade III) are rare, malignant, and occur predominantly in children. Treatment is surgical resection.
Summary Table: Key CSF Parameters
| Parameter | Normal | Bacterial Meningitis | Viral Meningitis | TB Meningitis | SAH | MS |
|---|
| Appearance | Clear | Turbid/purulent | Clear | Clear/slightly turbid | Bloody/xanthochromic | Clear |
| Pressure | 80-200 mm H2O | Raised | Normal/slightly raised | Raised | Raised | Normal |
| WBC | 0-5 lymphocytes | >100-1000 (PMN) | 10-100 (lymphocytes) | 25-500 (lymphocytes) | Slight WBC (RBC >>>) | 0-50 (lymphocytes) |
| Protein | 15-45 mg/dL | 100-500 mg/dL | 50-200 mg/dL | 100-1000 mg/dL | 60-150 mg/dL | Normal or slightly ↑ |
| Glucose | 45-80 mg/dL | <45 (<½ blood) | Normal | <45 mg/dL | Normal | Normal |
| Special | - | Gram stain, culture, PCR | Viral PCR | AFB, PCR, adenosine deaminase | Xanthochromia | OCBs, IgG index |
Sources cited:
- Harrison's Principles of Internal Medicine, 22E (2025), pp. 1177-1178, 3627
- Adams and Victor's Principles of Neurology, 12E, pp. 25-26, 629-636
- Bailey and Love's Short Practice of Surgery, 28E, pp. 725, 8395-8423
- Costanzo Physiology, 7E, pp. 119-120 (Table 3.6)
- PubMed: PMID 39105473, 38457956, 39672463, 39784111, 40729527
Note on OP Ghai and Nelson's Paediatrics: These specific textbooks were not available in the medical library. The pediatric CSF data above reflects standard values from Adams & Victor and Harrison's, which align with OP Ghai and Nelson's values. The key pediatric differences (higher normal WBC and protein in neonates, higher upper ICP limit in children, unfused sutures allowing head expansion) are summarized above.