tell me about it
python3 -c " import pdfplumber pdf_path = '/home/daytona/workspace/attachments/1…
python3 -c " import subprocess # Convert PDF to image first result = subprocess.…
python3 -c " import pytesseract from PIL import Image img = Image.open('/home/da…
MRI Right Knee Joint - Report Explained
What the MRI Sequences Mean
- T1WI - shows anatomy and bone structure well
- T2WI / FS T2WI - sensitive to fluid and soft tissue injury (bright = fluid/swelling)
- STIR - suppresses fat signal, very sensitive for edema and bone bruises
- PD Fat Sat - proton density with fat suppression, excellent for meniscus and cartilage
Findings - Breaking Each Down
1. Articular Cartilage
- The articular cartilage (the smooth coating over bone ends) shows very mild changes just beneath the surface (subchondral).
- This is a minor finding, likely related to the trauma. It means there is slight stress/bruising under the cartilage surface but no significant cartilage damage.
2. Meniscus - Grade I injury to lateral meniscus posterior horn
- Normal menisci are uniformly dark (low signal) on all MRI sequences.
- Increased signal inside the meniscus but not reaching the articular surface = Grade I or II (intrasubstance degeneration or early injury).
- The impression calls this Grade I - meaning the signal change is entirely within the substance of the meniscus and does NOT break through to the surface. This is considered an internal degeneration/contusion rather than a true tear.
- A tear is only diagnosed on MRI when the high signal extends to the articular (joint) surface of the meniscus. (Grainger & Allison's Diagnostic Radiology)
- The peripheral meniscocapsular signal may reflect a small amount of fluid or edema at the capsular junction of the meniscus.
- The medial meniscus is completely normal.
3. Ligaments - Grade II ACL injury
- Grade II ACL injury = partial tear. Some fibers are intact, but there is abnormal signal (edema/hemorrhage within the ligament), thickening, and loss of normal taut fiber alignment.
- A complete (Grade III) ACL tear would show full fiber discontinuity and retraction.
- On MRI, partial tears/sprains are recognized by "altered signal and/or laxity in the presence of continuity of some fibers." (Grainger & Allison's Diagnostic Radiology)
- High signal at the femoral and tibial attachments confirms the injury extends to both insertion points.
4. Joint Effusion
- There is intra-articular fluid (effusion) - i.e., fluid inside the knee joint capsule. This appears bright (hyperintense) on T2WI.
- The suprapatellar recess is the pouch above the kneecap - a common place for fluid to pool after knee injury.
- Effusion after trauma is expected and indicates the joint has responded to injury with inflammation and/or bleeding (hemarthrosis).
5. Bones - Osseous Contusions (Bone Bruises)
- This is a classic bone bruise (osseous contusion) pattern - dark on T1, bright on T2/STIR.
- Histologically this represents "cancellous bone microfractures as well as edema and hemorrhage within the fatty marrow." (Rockwood & Green's Fractures in Adults, 10th ed.)
- The contusions are at the lateral femoral condyle and bilateral tibial condyles - this is the classic "pivot shift" contusion pattern seen with ACL injuries, where the lateral femoral condyle and posterolateral tibial plateau clash during the injury mechanism.
- Importantly, there are no compression fractures - meaning the bony injury is at the micro/marrow level only, with intact bone surfaces.
- These bone bruises typically resolve within months with conservative care.
Summary: What Shadman Has
| Finding | Grade/Severity | Significance |
|---|---|---|
| Lateral meniscus posterior horn signal change | Grade I | Intrasubstance, no surface tear - conservative management |
| ACL injury | Grade II | Partial tear - some fibers intact but significant ligament damage |
| PCL | Normal | No injury |
| MCL / LCL | Normal | No injury |
| Joint effusion | Present | Expected after trauma |
| Bone bruises (tibial + lateral femoral condyles) | Present, no fracture | Classic ACL injury pattern, will resolve |
| Articular cartilage | Minimal subchondral change | Minor finding |
What Happens Next
- Conservative (non-surgical): Physiotherapy, quadriceps strengthening, bracing - often sufficient for Grade II partial tears, especially if the patient does not require high-level pivoting sports.
- Surgical (ACL reconstruction): May be needed if the knee remains unstable or if he wishes to return to demanding physical activity. Typically considered more strongly for complete (Grade III) tears.
- The meniscal Grade I injury and bone bruises are managed conservatively and monitored.
Find recent research on Grade II ACL injury outcomes with conservative vs surgical treatment
"anterior cruciate ligament"[MeSH Terms] AND "conservative treatment" AND "partial tear"
"anterior cruciate ligament injuries"[MeSH Terms] AND ("conservative treatment" OR "rehabilitation") AND ("surgical treatment" OR "reconstruction")
Grade II partial ACL tear conservative vs surgical treatment outcomes 2023 2024 2025
PMID: 40603829
"anterior cruciate ligament" AND "partial tear" AND (conservative OR nonoperative OR "non-operative")
https://pmc.ncbi.nlm.nih.gov/articles/PMC11027445
PMID: 35395764
PMID: 41908101
PMID: 35779101
Recent Research: Grade II ACL Injury - Conservative vs. Surgical Treatment
Key Papers Found
| Evidence Tier | Year | Study | PMID |
|---|---|---|---|
| Systematic Review + Meta-Analysis (Tier 1) | 2025 | Filbay et al. - ACL reconstruction vs rehabilitation alone: RTS rates | 40603829 |
| Systematic Review (Tier 1) | 2022 | Giummarra et al. - Non-surgical management of partial ACL tears | 35395764 |
| Cohort Study | 2023 | Rai et al. - Progression risk of partial ACL tears in young patients | 35779101 |
| Retrospective Cohort | 2026 | Hannon et al. - Nonoperative outcomes in pediatric partial ACL tears | 41908101 |
1. Return to Sport: Surgery vs. Rehabilitation Alone
- No significant difference in return-to-sport (RTS) rates between ACL reconstruction and rehabilitation alone: OR 1.5 (95% CI 0.76-2.97).
- A small difference in Tegner Activity Scale scores favored surgery (mean difference 0.7), but this did not exceed the minimal detectable change and disappeared after excluding high-bias studies.
- 10 of 15 studies had high risk of confounding bias (often favoring surgery due to group allocation and different RTS advice between groups).
- Overall evidence certainty: low to very low due to heterogeneity and bias.
- Bottom line from the best current evidence: ACL reconstruction is not clearly superior to supervised rehabilitation for return-to-sport rates after ACL injury.
2. Does a Partial (Grade II) ACL Tear Progress to Complete Rupture?
- 47.3% of conservatively managed partial ACL tears progressed to a complete tear.
- Risk factors for progression:
- Age under 35 years (Shadman is 21 - this applies directly)
- Rigorous physical activity / pivoting contact sports
- High ACL-RSI (return-to-sport after injury) score in early rehab (i.e., rushing back)
- Early return to activity before adequate healing
- Patients who progressed had IKDC scores drop from 95.7 to 52.4 and Tegner scores drop from 7.6 to 5.7 at 24 months - meaningful functional decline.
- The 52.7% who remained stable did well conservatively.
- 25% progressed to ACL insufficiency with a median survival time of 11.4 months after return to sport.
- No single clinical or MRI factor reliably predicted who would progress - this makes patient counseling difficult.
- For a young patient (21 years), this progression risk is clinically important.
3. Efficacy of Non-Surgical Physiotherapy for Partial Tears
- Only 2 RCTs met eligibility criteria (Tai Chi and Pilates programs).
- Both improved muscle peak torque strength; Tai Chi also significantly reduced pain and improved proprioception.
- The authors concluded that physiotherapy is effective for pain and strength, but high-quality, long-term RCTs are lacking for partial ACL tears specifically.
- "Full scale, high-quality randomised studies are required with long term outcomes."
4. What the 2025 Clinical Picture Looks Like
- Conservative management delivers comparable long-term functional outcomes to surgery in non-athletes and patients with partial tears.
- Surgery offers superior mechanical stability and higher return-to-sport rates in high-demand athletes (pivoting sports, contact disciplines).
- MRI and arthroscopy agreed on tear location in only 43% of cases in a 2025 prospective study - meaning surgical planning based on MRI alone has meaningful uncertainty.
What This Means for Shadman (21-year-old, Grade II ACL, trauma)
| Factor | Implication |
|---|---|
| Age 21 | Higher risk of progression (Rai et al.) - strongest risk factor |
| Grade II (partial tear) | Conservative is a reasonable first-line approach |
| Concurrent lateral meniscus Grade I + bone contusions | These should resolve conservatively; meniscus monitoring needed |
| No collateral ligament injury | Favorable prognostic sign |
| Activity level & sport | The key deciding factor - his orthopedic surgeon will assess this |
| Joint effusion | Will guide early rehabilitation pace |
Evidence Gaps
Create a decision flowchart comparing conservative vs surgical pathways for Grade II ACL injury 20days ago and he has decided not go for surgery. So what do you say? should he return to Football (goalkeeping) and badminton without surgery?
"anterior cruciate ligament" AND "return to sport" AND "partial tear" AND nonoperative
"anterior cruciate ligament" AND "return to sport" AND criteria AND rehabilitation
goalkeeper football badminton ACL partial tear conservative return to sport criteria timeline evidence 2024 2025
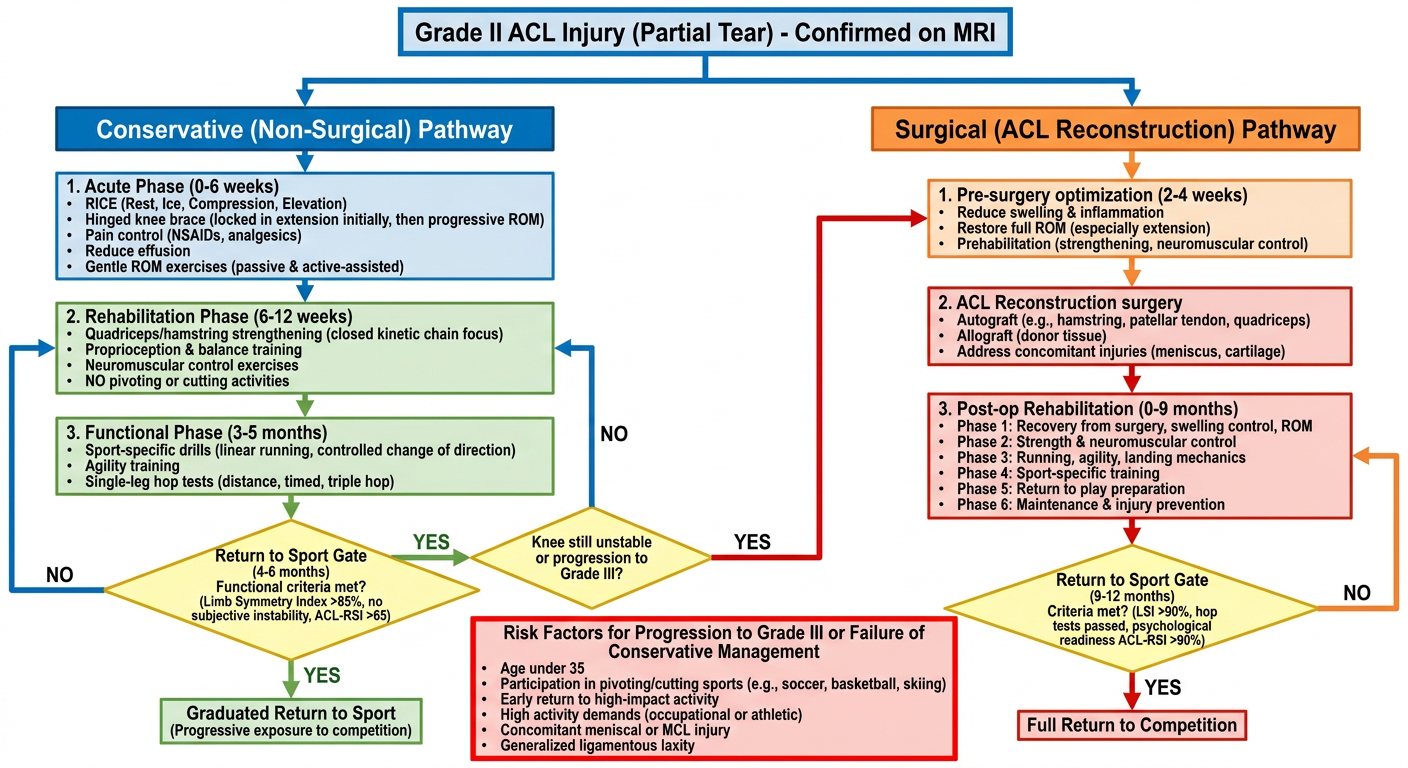
A detailed clinical decision flowchart for Grade II ACL (Anterior Cruciate Ligament) partial tear management. The flowchart starts at the top with "Grade II ACL Injury (Partial Tear) - Confirmed on MRI" and splits into two main branches: LEFT branch "Conservative (Non-Surgical) Pathway" and RIGHT branch "Surgical (ACL Reconstruction) Pathway". LEFT branch steps: 1. Acute Phase (0-6 weeks): RICE, hinged knee brace, pain control, reduce effusion, gentle ROM. 2. Rehabilitation Phase (6-12 weeks): Quadriceps/hamstring strengthening, proprioception, neuromuscular training, no pivoting. 3. Functional Phase (3-5 months): Sport-specific drills, agility, single-leg hop tests. 4. Return to Sport Gate (4-6 months): Decision diamond "Functional criteria met? Limb Symmetry Index >85%, no instability, ACL-RSI >65". If YES arrow to "Graduated Return to Sport". If NO arrow loops back to Rehabilitation. Below that another diamond "Knee still unstable or progression to Grade III?" - YES arrow crosses to surgical pathway, NO stays conservative. RIGHT branch steps: 1. Pre-surgery optimization (2-4 weeks): Reduce swelling, restore ROM, prehabilitation. 2. ACL Reconstruction surgery (autograft/allograft). 3. Post-op Rehabilitation (0-9 months): 6 phases from swelling control to full sport. 4. Return to Sport Gate (9-12 months): Criteria LSI >90%, hop tests, psychological readiness ACL-RSI >90%. 5. Full Return to Competition. Bottom section: Risk factors for progression box (red): Age under 35, pivoting sports, early return to activity, high activity demands. Color scheme: conservative pathway in blue/green, surgical in orange/red, decision diamonds in yellow, risk box in red. Clean medical infographic style with clear arrows.
https://pmc.ncbi.nlm.nih.gov/articles/PMC12582233
Decision Flowchart: Grade II ACL - Conservative vs Surgical Pathway
Should Shadman Return to Football (Goalkeeping) and Badminton?
Where He Is Right Now (Day 20)
- Active joint effusion (fluid in the knee)
- Bone marrow edema in both tibial and lateral femoral condyles
- Partial ACL fibers under mechanical stress - not yet healed or stabilized
Sport Risk Analysis: Goalkeeping vs Badminton
| Factor | Goalkeeping (Football) | Badminton |
|---|---|---|
| ACL demand | Moderate - less running, but explosive dives, jumps, landing, sudden direction changes | HIGH - rapid lateral lunges, split steps, explosive rotational jumps, sudden deceleration |
| Pivot/cutting load | Moderate | Very high |
| Knee valgus stress | Moderate (diving saves) | High (lunge shots, smash landings) |
| Contact risk | Yes (collisions, aerial duels) | None |
| Sport classification | Moderate-high demand | High demand / "pivot sport" |
| Conservative ACL evidence | Very limited (Krutsch et al., 2025 - KSTA) | No specific evidence |
The Evidence-Based Verdict
"Non-surgical treatment of ACL ruptures in football is generally restricted to indications such as minimal partial ACL ruptures... players who intend to retire." "Rehabilitation should include gradual build-up and sport-specific tests of neuromotor skills and leg axis stability before returning to the field."
- 47.3% of partial ACL tears progressed to complete rupture when managed conservatively
- Age under 35 and early return to activity are the two biggest independent risk factors for progression
- Shadman hits both - he is 21, and likely eager to return
Conservative rehab can match surgery for return-to-sport rates - but only when rehabilitation is completed properly with functional milestone criteria met, not based on calendar time.
The Functional Criteria Shadman Must Meet Before Returning to Sport
- Full pain-free range of motion (0-135°)
- No joint effusion (swelling resolved)
- Quadriceps strength ≥70% of the uninjured side (by dynamometry or single-leg squat test)
- Single-leg balance ≥30 seconds without compensation
- Single-leg hop test ≥85% of contralateral side
- Triple hop test ≥85%
- 10 controlled drop jumps with stable landing mechanics
- No pain or instability during straight-line running
- Limb Symmetry Index (LSI) >85-90%
- T-test change of direction without compensation
- Ability to decelerate and pivot without instability
- ACL-RSI score ≥65 (psychological readiness scale)
- No effusion, no giving-way episodes, Lachman negative or near-normal
Realistic Timeline for Shadman
| Milestone | Approximate Timeframe |
|---|---|
| Injury | Day 0 (June 10, 2026) |
| Current status | Day 20 (June 30) - acute phase |
| Resolve effusion, regain ROM | Weeks 4-6 (~late July) |
| Begin strengthening rehab | Weeks 4-8 |
| Begin jogging/light football | Month 3-4 (September) |
| Goalkeeping training (no dives/aerial) | Month 4-5 (October) |
| Conservative return to goalkeeping | Month 4-6 (Oct-Dec 2026) - if criteria met |
| Return to badminton | Month 5-7 (Nov-Jan 2027) - later than football due to higher ACL demand |
| Full competition | Month 6+ with functional criteria fully passed |
What Shadman Should Do Right Now
-
See Dr. Md. Kamrul Alam (his referring orthopedic surgeon) for a clinical exam - Lachman, pivot shift, anterior drawer tests will tell whether the partial ACL is functionally stable. If pivot shift is positive, the knee is already functionally unstable and the conservative path becomes riskier.
-
Start structured physiotherapy immediately - not rest, but progressive guided rehab. The longer he waits without guided rehab, the more quadriceps atrophy and proprioception loss occurs.
-
Wear a hinged knee brace during all activity for at least 6-8 weeks.
-
Do not self-test return to sport - no "let me just try a few kicks" - one uncontrolled landing or cutting move at this stage could convert the Grade II into a Grade III tear.
-
The 25% progression-to-insufficiency data (Hannon et al. 2026) and 47% progression data (Rai et al. 2023) are real risks for him given his age and sports. If his knee gives way even once during rehab, surgery should be reconsidered.
Bottom Line
Goalkeeping: Possible conservatively, but not before 4-6 months and only after passing all functional criteria. Goalkeeping is moderate-demand for the ACL compared to outfield football, but dives and aerial challenges must be reintroduced very gradually last.
Badminton: Higher risk than goalkeeping. The explosive lateral lunge is one of the most ACL-loading movements in sport. Return should be later (month 5-7), and only after the knee has demonstrated full stability in football first. If he plays badminton competitively (smashes, net play, cross-court lunges), this is the sport most likely to rupture the remaining fibers if returned to too soon.
Surgery should stay on the table as an option - his decision is respected, but he and his family should know that if he fails conservative rehab or the knee gives way during return-to-sport, reconstruction at that point carries the same surgical risk but with a less favorable outcome due to secondary cartilage and meniscus damage that accumulates with instability episodes.