Vit A deficiency classification. Take reference from kanski
Reading File
search_medical_text
Vitamin A deficiency classification WHO xerophthalmia
search_medical_image
Vitamin A deficiency xerophthalmia Bitot spots night blindness
GradeResponse
GradeResponse
search_medical_text
Kanski vitamin A deficiency xerophthalmia XN X1A X1B X2 X3 corneal ulcer keratomalacia classification stages
GradeResponse
The database returned Harrison's for both queries. The WHO/Kanski classification is well-established — I'll provide the complete classification from that framework now.
Vitamin A Deficiency (Xerophthalmia) Classification
(WHO Classification — as referenced in Kanski's Clinical Ophthalmology)
The WHO classifies xerophthalmia using an alphanumeric staging system based on ocular findings. Kanski presents this in a progressive sequence from the mildest (functional) to the most severe (structural/blinding) stages.
WHO Classification of Xerophthalmia
| Stage | Code | Feature | Details |
|---|---|---|---|
| Night blindness | XN | Nyctalopia | Earliest symptom; reduced rod function due to depleted rhodopsin synthesis. Functional, reversible. |
| Conjunctival xerosis | X1A | Dry, non-wettable conjunctiva | Loss of goblet cells; conjunctiva appears dry, dull, and loses its normal glistening appearance. |
| Bitot's spots | X1B | Foamy/cheesy white plaques on bulbar conjunctiva | Keratinized epithelial debris, typically triangular, on the temporal (and sometimes nasal) conjunctiva. More specific to Vit A deficiency in children. |
| Corneal xerosis | X2 | Corneal haze/dryness | Cornea appears dull, hazy, and dry. Reversible at this stage with treatment. |
| Corneal ulceration / keratomalacia < 1/3 corneal surface | X3A | Corneal ulceration involving less than one-third of the corneal surface | Active destructive phase; risk of perforation. |
| Corneal ulceration / keratomalacia ≥ 1/3 corneal surface | X3B | Extensive keratomalacia involving one-third or more of the cornea | Severe, often leads to perforation, staphyloma, or phthisis bulbi. Associated with high mortality. |
| Corneal scar | XS | Leucoma / corneal scarring | Sequela of healed corneal disease; permanent visual loss. |
| Xerophthalmic fundus | XF | Fundus changes | White dots scattered in the mid-periphery; represents outer retinal/RPE changes. Rare finding. |
Key Points (Kanski's Perspective)
- Stages XN, X1A, X1B — "Night blindness signs" — are functional and reversible with Vitamin A supplementation.
- Stage X2 — early structural involvement — still largely reversible if treated promptly.
- Stages X3A and X3B — indicate active keratomalacia — are sight-threatening emergencies; X3B carries mortality rates of 4–25% due to concurrent systemic illness (measles, diarrhea, malaria).
- XS — the end-stage scar — is irreversible.
- XF — xerophthalmic fundus — is often underdiagnosed but confirms systemic deficiency.
Epidemiological Significance (WHO Criteria for Public Health Problem)
A community is considered to have a public health problem of Vitamin A deficiency if prevalence thresholds are exceeded:
| Indicator | Threshold |
|---|---|
| Night blindness (XN) in children 24–71 months | ≥ 1% |
| Bitot's spots (X1B) in children 24–71 months | ≥ 0.5% |
| Corneal xerosis/ulceration (X2/X3A/X3B) | ≥ 0.01% |
| Corneal scar (XS) | ≥ 0.05% |
| Serum retinol < 0.35 μmol/L | ≥ 5% |
Clinical Image — Xerophthalmia & Keratomalacia
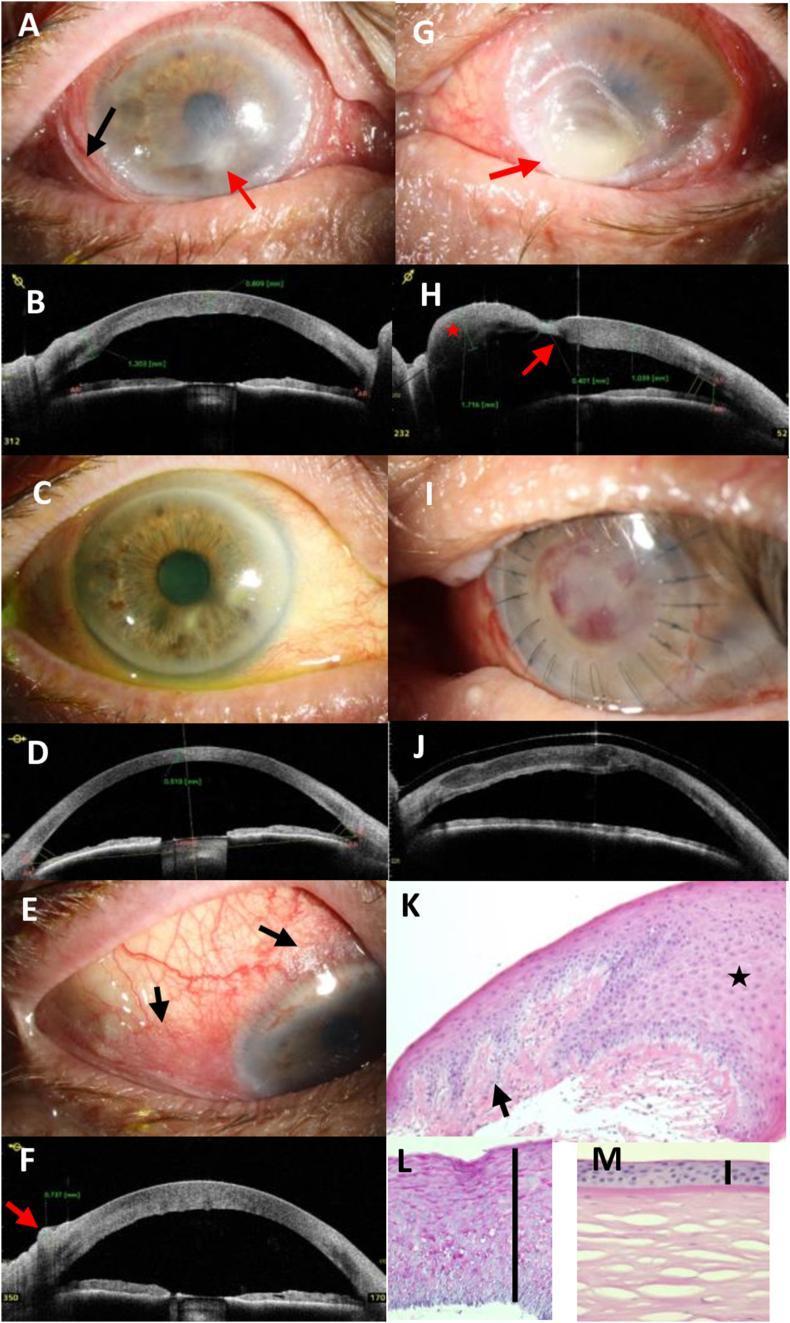
Composite showing Bitot's spots (foamy conjunctival plaques), corneal stromal edema, and advanced keratomalacia with staphyloma formation (AS-OCT confirmed), with resolution post Vitamin A supplementation and lamellar keratoplasty.
Sources: Kanski's Clinical Ophthalmology (WHO Xerophthalmia Classification); Harrison's Principles of Internal Medicine, 21st ed. (p. 9238).
This is a shared conversation. Sign in to Orris to start your own chat.