Write short note on Nevus cutaneous lipomatosus superficialis for ms general surgery graduate and give cross questions and answers for the same in poster presentation
Nevus cutaneous lipomatosus superficialis clinical features diagnosis treatment
lipomatous hamartoma skin histopathology differential diagnosis surgical excision
nevus lipomatosus superficialis skin lesion histopathology
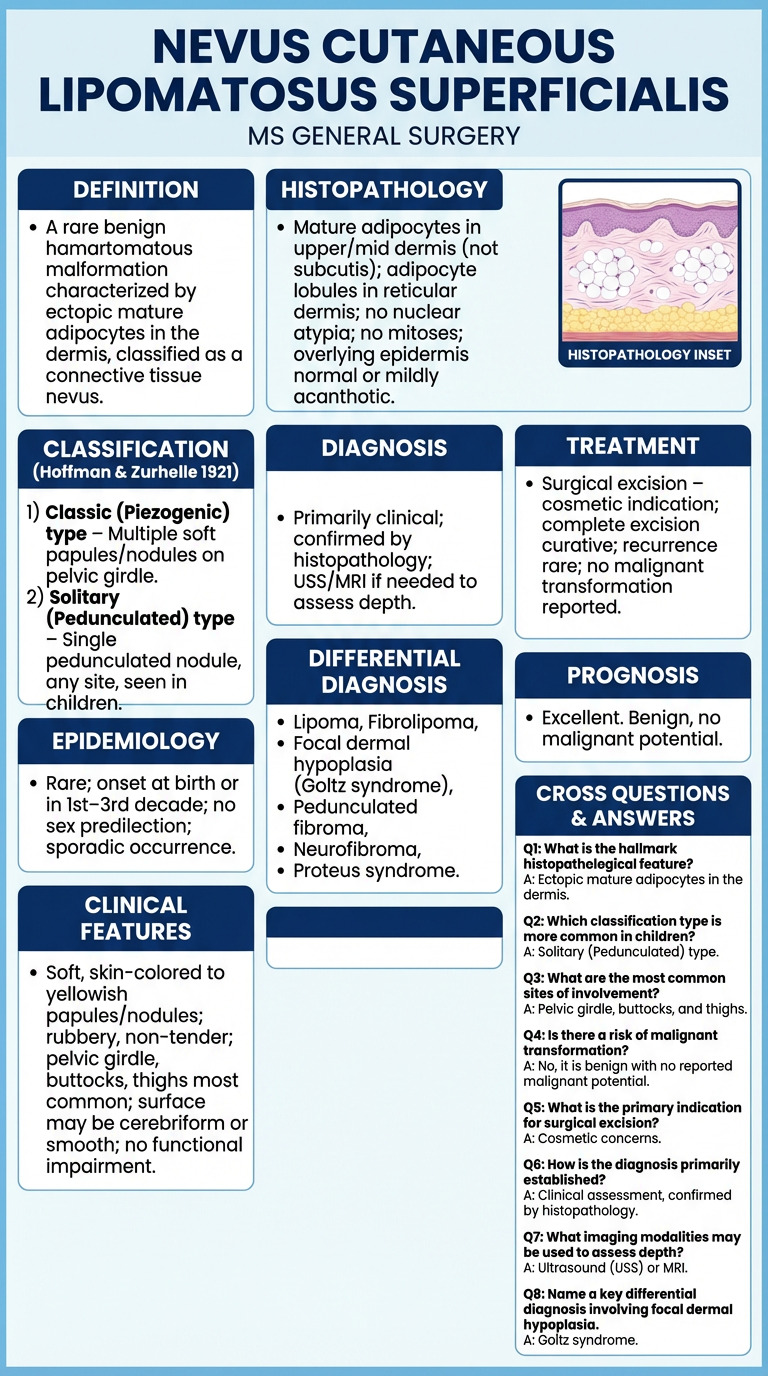
A clean, professional medical academic poster titled "Nevus Cutaneous Lipomatosus Superficialis" for MS General Surgery. Include the following organized sections with clear bold headings and bullet points: DEFINITION: A rare benign hamartomatous malformation characterized by ectopic mature adipocytes in the dermis, classified as a connective tissue nevus. CLASSIFICATION (Hoffman & Zurhelle 1921): 1) Classic (Piezogenic) type – Multiple soft papules/nodules on pelvic girdle. 2) Solitary (Pedunculated) type – Single pedunculated nodule, any site, seen in children. EPIDEMIOLOGY: Rare; onset at birth or in 1st–3rd decade; no sex predilection; sporadic occurrence. CLINICAL FEATURES: Soft, skin-colored to yellowish papules/nodules; rubbery, non-tender; pelvic girdle, buttocks, thighs most common; surface may be cerebriform or smooth; no functional impairment. HISTOPATHOLOGY: Mature adipocytes in upper/mid dermis (not subcutis); adipocyte lobules in reticular dermis; no nuclear atypia; no mitoses; overlying epidermis normal or mildly acanthotic. DIAGNOSIS: Primarily clinical; confirmed by histopathology; USS/MRI if needed to assess depth. DIFFERENTIAL DIAGNOSIS: Lipoma, Fibrolipoma, Focal dermal hypoplasia (Goltz syndrome), Pedunculated fibroma, Neurofibroma, Proteus syndrome. TREATMENT: Surgical excision – cosmetic indication; complete excision curative; recurrence rare; no malignant transformation reported. PROGNOSIS: Excellent. Benign, no malignant potential. CROSS QUESTIONS & ANSWERS section with 8 bold questions and concise answers listed. Use a light blue and white color scheme with navy blue headers, organized in a clear grid layout suitable for a medical poster presentation. Add a small histopathology inset diagram showing adipocytes in dermis.
Nevus Cutaneous Lipomatosus Superficialis (NLS)
Definition
Historical Background
Classification
| Type | Features |
|---|---|
| Classic (Multiple/Piezogenic) | Multiple soft papules/nodules; pelvic girdle, buttocks, upper thighs; onset in 1st–3rd decade |
| Solitary (Pedunculated) | Single pedunculated or sessile nodule; any site including ear, scalp, face; often in children/neonates; more common type overall |
Epidemiology
- Rare condition; exact prevalence unknown
- Classic type: onset 1st–3rd decade of life
- Solitary type: congenital or early childhood
- No sex predilection; sporadic, no known genetic transmission established
Clinical Features
- Soft, skin-colored to yellowish papules or nodules
- Rubbery, non-tender, freely mobile
- Surface may be smooth, cerebriform, or wrinkled
- Classic type: clustered lesions on pelvic girdle, buttocks, lumbar region, thighs
- Solitary type: pedunculated nodule — ear tragus, scalp, face, trunk
- No associated systemic abnormalities in most cases
- Asymptomatic; occasionally cosmetically distressing
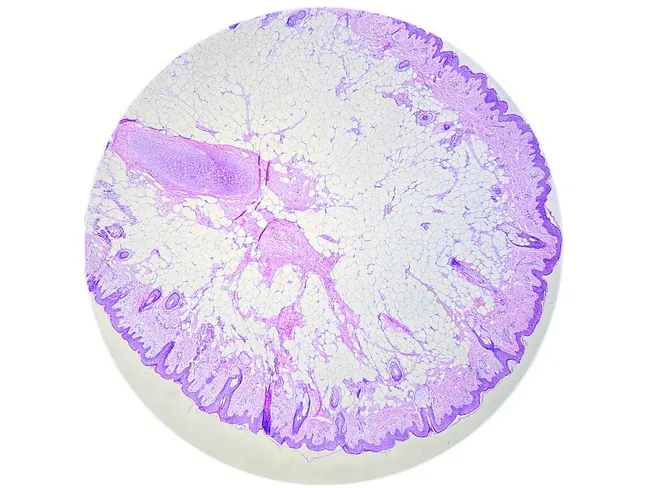
Histopathology (Key for Exam)
- Lobules of mature adipocytes with clear cytoplasm and compressed nuclei
- Situated in the mid to upper dermis, intermingled with collagen bundles
- No cellular atypia, no mitotic figures
- Overlying epidermis: normal or mildly acanthotic/papillomatous
- Fibrous stroma surrounds adipocyte lobules
- No lipoblasts, no inflammation, no vascular proliferation
Diagnosis
- Clinical diagnosis in classic form (grouped soft papules over pelvic girdle)
- Confirmed by excisional biopsy + histopathology
- Ultrasound / MRI — useful to assess depth, rule out deeper extension, and plan surgery
- Dermoscopy: may show yellowish structureless areas
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Lipoma | Subcutaneous, not dermal; no papular grouping |
| Fibrolipoma | Contains fibrous tissue admixed with fat; deeper |
| Focal dermal hypoplasia (Goltz syndrome) | X-linked dominant; multisystem involvement; skin herniation of fat |
| Pedunculated fibroma (skin tag) | Fibrous stroma dominant; no fat |
| Neurofibroma | Neural tissue; café-au-lait spots; NF1 association |
| Proteus syndrome | Mosaic overgrowth syndrome; lipomatous involvement + other anomalies |
| Angiolipoma | Vascular channels + fat; painful; subcutaneous |
Treatment
- Surgical excision — treatment of choice; cosmetic indication is the primary reason
- Complete excision is curative
- Recurrence is rare after complete excision
- No malignant transformation has been reported
- In solitary pedunculated type (e.g., ear, scalp): simple excision under local anesthesia
- No medical treatment needed
Prognosis
- Excellent — purely benign lesion
- No systemic association, no malignant potential
- Cosmetic outcome post-excision is very good
Cross Questions & Answers for Poster Presentation
Tip for viva/poster defense: If asked "is it a hamartoma or a choristoma?" — NLS is a hamartoma (normal tissue in abnormal quantity at a normal site), not a choristoma (normal tissue at an abnormal body site). The fat is in the skin (normal site for fat lobules in subcutis), but displaced superficially into the dermis.