A 26 year old female suddenly experienced blood in urine but not continously coming
Reading File
search_medical_text
hematuria young female causes differential diagnosis
search_medical_text
intermittent hematuria evaluation workup management
search_medical_image
hematuria diagnostic algorithm causes
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive clinical overview of intermittent gross hematuria in a 26-year-old female.
Hematuria in a Young Female — Clinical Overview
Hematuria is defined as the presence of blood in the urine. It can be gross (visible) or microscopic (≥3 RBCs/HPF on urinalysis). In this case, the intermittent nature is an important clue.
Differential Diagnosis
🔴 Most Common Causes in a Young Female
| Category | Condition | Key Features |
|---|---|---|
| Urinary Tract Infection | Cystitis, urethritis | Dysuria, frequency, urgency; most common cause in young women |
| Urolithiasis (Kidney Stones) | Ureteral or renal stones | Sudden flank pain (renal colic), colicky, unilateral; may cause painless gross hematuria (Harrison's, p. 8698) |
| Glomerulonephritis | IgA nephropathy, thin basement membrane disease | Often episodic hematuria, may follow upper respiratory tract infection; dysmorphic RBCs/RBC casts on UA |
| Urethral causes | Urethritis, trauma | Post-coital or external trauma-related |
| Menstrual contamination | Pseudohematuria | Confirm with midstream clean catch |
🟡 Less Common but Important
| Condition | Features |
|---|---|
| IgA Nephropathy | Most common glomerulonephritis in young adults; synpharyngitic hematuria (hematuria coinciding with sore throat/URI) |
| Thin Basement Membrane Nephropathy | Familial; benign; persistent microscopic > gross hematuria |
| Endometriosis of urinary tract | Cyclic hematuria corresponding to menstrual cycle |
| Arteriovenous malformation (AVM) | Rare; intermittent; diagnosed on imaging |
| Loin pain-hematuria syndrome | Episodic gross hematuria + loin pain in young women; diagnosis of exclusion |
| Coagulation disorders | Bleeding diathesis; check PT/aPTT |
| Bladder pathology | Hemangioma, polyp (malignancy rare at age 26) |
Diagnostic Algorithm
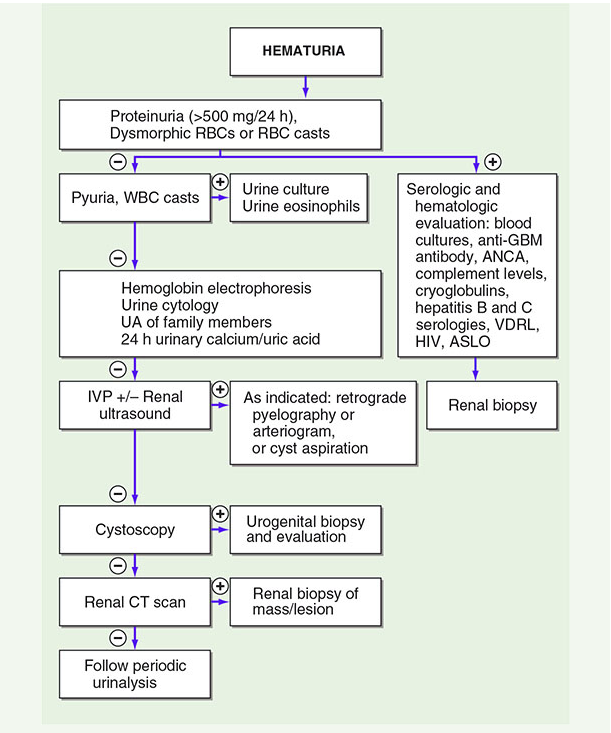
Initial Workup
Step 1 — Confirm True Hematuria
- Urinalysis (microscopy) on a fresh, midstream clean-catch specimen
- Confirm ≥3 RBCs/HPF (threshold consistent across AUA and international guidelines)
- Rule out menstrual contamination, myoglobinuria, hemoglobinuria (dipstick positive but no RBCs on microscopy)
Step 2 — Characterize the Hematuria
| Finding | Suggests |
|---|---|
| Dysmorphic RBCs / RBC casts | Glomerular origin → nephrology referral |
| WBC casts, pyuria | Infection or interstitial nephritis |
| Proteinuria >500 mg/24h | Glomerular disease |
| Normal morphology RBCs | Lower urinary tract or non-glomerular upper tract |
Step 3 — Additional Tests
- Urine culture — rule out UTI
- Urine cytology — if recurrent or risk factors (low yield at age 26, but useful if no other cause found)
- CBC, coagulation profile — bleeding disorders
- Serum creatinine, eGFR — renal function
- Serologies (if glomerulonephritis suspected): ANA, ANCA, anti-GBM, complement (C3/C4), ASO titer, hepatitis B/C, HIV
- Hemoglobin electrophoresis — sickle cell trait (can cause hematuria)
- 24-hour urine calcium/uric acid — hypercalciuria, hyperuricosuria
Step 4 — Imaging
- Renal ultrasound — first-line; detects stones, cysts, masses
- CT urogram (non-contrast + contrast) — gold standard for urolithiasis and upper tract evaluation
- Retrograde pyelography — if CT inconclusive
Step 5 — Cystoscopy
- Generally recommended for gross hematuria in adults; in a 26-year-old without risk factors, may be deferred unless workup is unrevealing or hematuria persists
Key Considerations in This Patient
- Age 26, female — UTI and urolithiasis are the leading causes to exclude first; simple and treatable.
- Intermittent nature — points toward IgA nephropathy (episodic, often triggered by illness), stones (passes and recurs), or loin pain-hematuria syndrome.
- Synpharyngitic pattern? — if hematuria occurs within 1–2 days of a sore throat/URI, IgA nephropathy is highly likely.
- Cyclic timing with menstruation? — consider urinary endometriosis.
- Malignancy is very unlikely at this age but cannot be dismissed if workup is negative and hematuria persists (AUA guideline notes the intermittent nature of cancer-related hematuria as reason not to ignore a single positive microscopy result — Hematuria as a Marker of Occult Urinary Tract Cancer, p. 2).
Summary Management Approach
1. Urinalysis with microscopy (clean catch, midstream)
2. Urine culture
3. Renal ultrasound
4. If glomerular features → nephrology workup + serologies
5. If no infection/stone → CT urogram
6. If unrevealing → consider cystoscopy, urology/nephrology referral
7. Track timing relative to menstrual cycle and infections
⚠️ Clinical Pearl: Never attribute hematuria to menstrual contamination without confirmed clean-catch microscopy. Intermittent hematuria from cancer can be falsely reassuring — a single positive microscopy result warrants evaluation (AUA guideline).
This is a shared conversation. Sign in to Orris to start your own chat.