7th lession notes
Asking for Preferences
Community health nursing 1 5th sem
Reading File
Finding Sources
Searching the Web
Community Health Nursing 1 5th semester BSc nursing 7th lesson syllabus topics
Finding Sources
Reading Web Page
https://www.slideshare.net/slideshow/assisting-individuals-a…
Reading Web Page
https://www.dmiher.edu.in/frontEnd/pages/page/images/pdf/poc…
Finding Sources
Finding Sources
I have sufficient content from the syllabus and the web extraction. Let me now compile comprehensive notes for Unit 7.
Unit 7 - Assisting Individuals and Families to Promote and Maintain Their Health
Community Health Nursing I | 5th Semester B.Sc. Nursing (INC Syllabus)
Overview
This unit (10 hours theory) focuses on how community health nurses deliver essential health services to individuals, families, and groups through home visits, community outreach, and at Health & Wellness Centres (HWCs), using approved protocols from MoH&FW and INC regulations.
A. Assessment of Individuals and Families
(Review from Child Health Nursing, Medical Surgical Nursing, OBG Nursing)
The community health nurse assesses the health status of:
- Children
- Women
- Adolescents
- Elderly
Purpose of Assessment:
- Identify health needs and problems
- Plan need-based, appropriate care
- Prioritize referrals
- Monitor progress over time
B. Assessment of Children
1. Monitoring Growth and Development
- Growth = physical changes (increase in height, weight)
- Development = skill/milestone progression (speaking, walking, social skills)
Tools used:
- Growth charts (WHO/National standards)
- Height boards, infantometers
- Weighing scales
Nurse's Role:
- Measure growth parameters during home/clinic visits
- Educate parents about nutrition and developmental stimulation
- Identify delays or abnormalities early
2. Anthropometric Measurements
- Height / Length
- Weight
- BMI (Body Mass Index)
- Head circumference (in infants)
- Mid-Upper Arm Circumference (MUAC) - for malnutrition screening
3. Developmental Milestones
- Assess gross motor, fine motor, language, and social milestones
- Use standard milestone charts
- Refer if delay is noted
4. Social Development
- Observation of interaction with family, peers
- Assess school attendance and behavior
C. Assessment of Women
1. Nutritional and Reproductive Health Screening
Why it matters:
- High prevalence of iron deficiency anemia, underweight, and obesity in Indian women
Parameters assessed:
- Hemoglobin levels (to detect anemia)
- Height / Weight / BMI
- Dietary patterns and food habits
- Obstetric history (number of pregnancies, abortions, living children)
- Use of contraception and menstrual regulation methods
2. Menstrual Cycle Assessment
- Regularity, duration, flow
- Identify dysmenorrhea, menorrhagia, or absence of menses
- Counsel on menstrual hygiene and self-care
- Identify and refer cases of anemia or hormonal disorders
3. Breast Self-Examination (BSE)
- Teach women how to perform BSE monthly
- Identify any lumps, discharge, or skin changes
- Refer suspicious findings for further evaluation
D. Providing Primary Care at Home / Health Centres
Routine Check-ups
- Covers all age groups: children, pregnant women, elderly, those with chronic conditions
Nurse's Responsibilities:
- Measure vital signs (BP, temperature, pulse, respiration)
- Conduct visual inspections (skin, eyes, wounds)
- Monitor weight, height, BMI
- Record findings and plan further care or referrals
Immunization
- Goal: prevent vaccine-preventable diseases
- Nurse's role:
- Check immunization status of children and pregnant women
- Administer vaccines as per the Universal Immunization Programme (UIP)
- Educate about the immunization schedule
- Maintain cold chain and records
Health Counseling
- Dietary counseling (balanced diet, breastfeeding)
- Hygiene and sanitation
- Family planning counseling
- Counseling for chronic disease management (diabetes, hypertension)
- Antenatal and postnatal counseling
E. Therapeutic Procedures at Home and in the Community
Community health nurses are trained to perform basic therapeutic procedures during home visits or at sub-centers/HWCs.
Definition: Therapeutic procedures are interventions carried out to treat a condition, relieve symptoms, or assist recovery. In community settings these are limited to simple, safe, approved techniques.
| Procedure | Purpose |
|---|---|
| Wound dressing | Prevent infection and promote healing |
| Temperature monitoring | Fever detection and illness follow-up |
| Blood pressure check | Screen and manage hypertension |
| Glucometer testing | Monitor blood sugar in diabetic patients |
| Administering injections | Vaccines, iron injections (as per protocol) |
| Oral Rehydration Therapy (ORT) | Manage diarrhea in children |
| Nebulization | For respiratory conditions (at sub-center) |
Nurse must follow: Standing orders and approved protocols from MoH&FW/INC
F. Records and Reports
The community health nurse must maintain proper records for accountability and continuity of care.
Types of Records:
- Family folder / Family health record
- Antenatal and postnatal registers
- Immunization records
- Growth monitoring records
- Daily / Weekly activity reports
- Field practice reports
Importance:
- Continuity of care
- Monitoring trends
- Planning interventions
- Legal documentation
G. Care for Specific Groups
Adolescents
- Physical growth assessment (height, weight, BMI)
- Menstrual health (girls)
- Nutritional assessment (anemia screening)
- Mental health screening
- Counseling on sexual and reproductive health
- Prevention of substance abuse
Elderly
- Assessment of activities of daily living (ADL)
- Screening for hypertension, diabetes, COPD
- Fall risk assessment
- Mental status evaluation (dementia, depression)
- Social support assessment
H. Nurse's Role - Summary
| Function | Activities |
|---|---|
| Assessor | History taking, physical examination, anthropometry |
| Educator | Health education, counseling individuals and families |
| Care Provider | Therapeutic procedures, first aid, wound care |
| Coordinator | Referral and follow-up with higher health facilities |
| Record Keeper | Maintaining family folders, registers, reports |
| Advocate | Identifying vulnerable individuals and advocating for their care |
Key Learning Outcomes (as per INC)
By the end of this unit, students should be able to:
- Assess and interpret health status of individuals and the community correctly
- Organize and provide need-based health services
- Perform primary care at home/health centres using approved standing orders and protocols
- Develop skill in maintenance of records and reports
- Appreciate the importance of teamwork and inter-sectoral coordination
Quick Revision Points
- Unit 7 = 10 theory hours (one of the longest units in CHN-I)
- Focuses on all age groups: children, women, adolescents, elderly
- Key tools: growth charts, anthropometric measurements, vital signs
- Key activities: monitoring growth & development, immunization, health counseling, therapeutic procedures
- Always follow MoH&FW / INC approved protocols and standing orders
- Nurse's role: assessor, educator, care provider, coordinator, record keeper, advocate
These notes cover the complete INC syllabus content for Unit 7 of Community Health Nursing I. Let me know if you want any subtopic expanded further - such as detailed immunization schedules, BSE technique, bag technique for home visits, or growth chart interpretation.
Menstrual cycle, breast self examination, Maintenance of record and reports,
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching the Web
community health nursing maintenance of records and reports types family folder PHC registers
Reading File
Reading Web Page
https://www.slideshare.net/slideshow/records-and-reportsin-p…
Loading Image
I now have all the content needed for comprehensive notes on all three topics. Here are your detailed notes:
Unit 7 - Detailed Notes
Community Health Nursing I | 5th Semester B.Sc. Nursing
TOPIC 1: MENSTRUAL CYCLE
Definition
The menstrual cycle is a regular, recurring series of physiological changes in a woman's reproductive system that prepares the body for pregnancy. Its most visible feature is periodic vaginal bleeding (menstruation) due to shedding of the uterine lining.
- Average cycle length: 28 days (counted from Day 1 of one period to Day 1 of the next)
- Normal range: 21-35 days
- Cycle days are numbered starting from the first day of menstruation
Ganong's Review of Medical Physiology, 26th Ed.
Phases of the Menstrual Cycle
Phase 1 - Menstrual Phase (Day 1-5)
- Shedding of the endometrial lining
- Estrogen and progesterone levels fall
- Normal blood loss: 30-80 mL
- Duration: 3-7 days
Phase 2 - Follicular / Proliferative Phase (Day 1-14)
- Dominated by Estrogen (17β-Estradiol)
- FSH stimulates several primordial follicles to grow; one becomes the dominant (Graafian) follicle
- Endometrium thickens (proliferates) - glands and stroma grow, spiral arteries elongate
- Cervical mucus becomes copious, watery, elastic - shows "ferning" pattern on a glass slide
- Channels form in the mucus creating openings for sperm
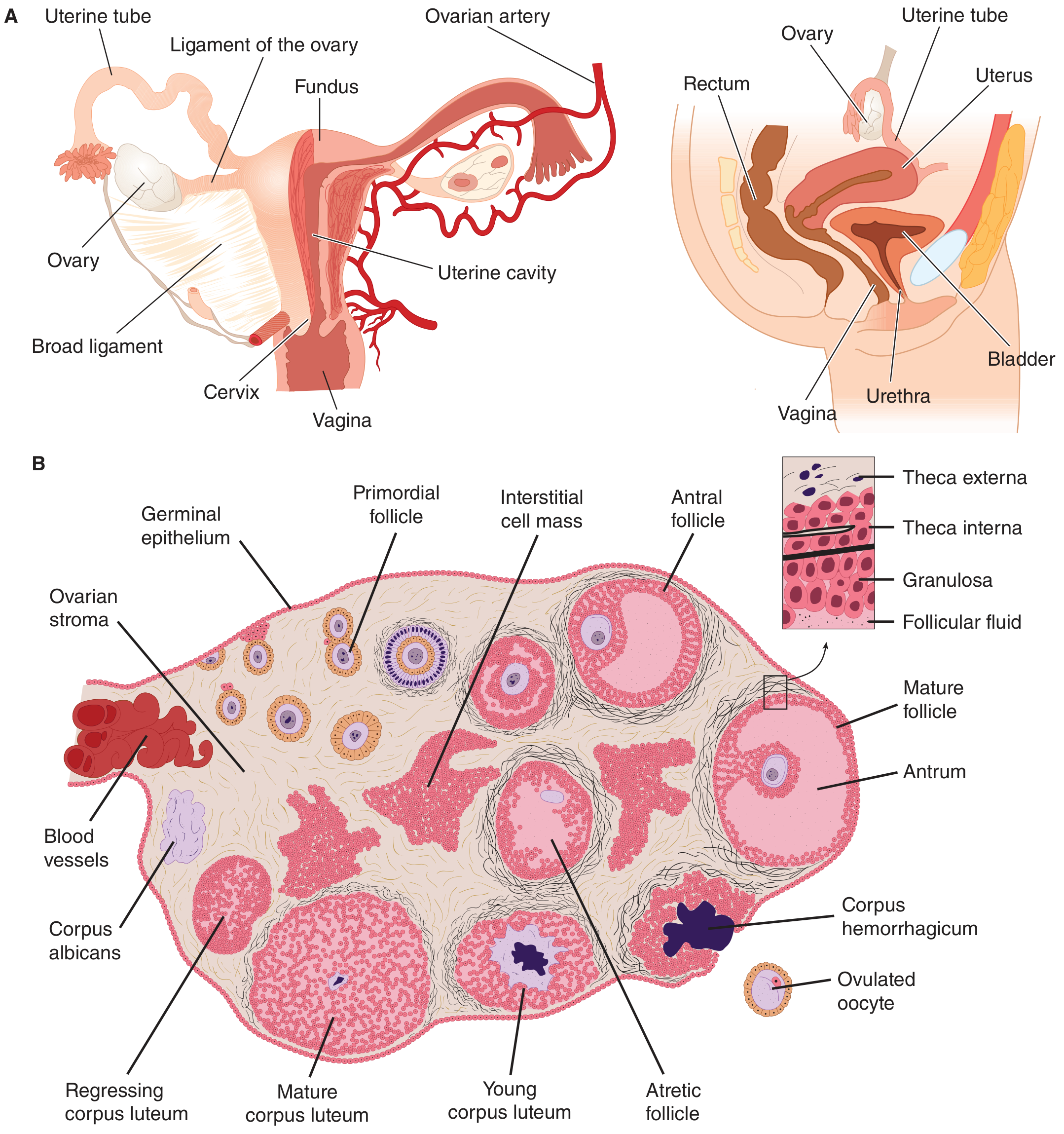
Phase 3 - Ovulation (Day 14)
- LH surge triggers rupture of the dominant follicle
- Ovum is released into the abdominal cavity and picked up by the fimbriated ends of the uterine tubes
- Minor bleeding from follicle may cause brief lower abdominal pain = Mittelschmerz
- The ruptured follicle fills with blood = Corpus hemorrhagicum
Phase 4 - Luteal / Secretory Phase (Day 14-28)
- Dominated by Progesterone
- Granulosa and theca cells proliferate to form the Corpus luteum (yellowish, lipid-rich)
- Endometrial changes:
- Proliferation slows
- Uterine glands become tortuous, accumulate glycogen
- Stroma becomes edematous
- Spiral arteries become more coiled
- Cervical mucus becomes thick, non-elastic, does not fern (blocks sperm entry)
- Progesterone has a mild thermogenic action - raises basal body temperature (basis of rhythm method of contraception)
- If no fertilization: corpus luteum regresses → estrogen and progesterone fall → menstruation begins
Hormonal Control Summary
| Hormone | Phase | Effect |
|---|---|---|
| FSH | Follicular | Stimulates follicle growth |
| Estrogen | Follicular | Endometrial proliferation, cervical mucus changes |
| LH surge | Ovulation (Day 14) | Triggers ovulation |
| Progesterone | Luteal | Endometrial secretory changes, raises body temp |
Normal Menstrual Parameters (for Assessment)
| Parameter | Normal Value |
|---|---|
| Cycle length | 21-35 days |
| Duration of flow | 3-7 days |
| Amount of blood loss | 30-80 mL |
| Onset | Menarche: 10-15 years |
Common Menstrual Disorders to Identify & Refer
| Disorder | Description |
|---|---|
| Dysmenorrhea | Painful menstruation (cramps) |
| Menorrhagia | Excessive/prolonged bleeding |
| Oligomenorrhea | Infrequent cycles (>35 days) |
| Amenorrhea | Absence of periods |
| Metrorrhagia | Irregular bleeding between periods |
| PMS | Pre-menstrual syndrome (bloating, mood changes) |
Nurse's Role in Menstrual Health (Community Setting)
- Assessment - Ask about cycle regularity, duration, flow, pain, last menstrual period (LMP)
- Counseling on menstrual hygiene:
- Use clean absorbent material (sanitary pads/cloth)
- Change pads every 4-6 hours
- Wash genitalia with clean water
- Avoid using unclean materials (risk of infection/toxic shock)
- Identify abnormalities - Refer cases of heavy bleeding, severe pain, absent periods
- Screen for anemia - Check conjunctiva, pallor; refer for hemoglobin testing if suspected
- Educate about normalcy - Reduce myths and taboos around menstruation
- Document - Record LMP, cycle details in family health record
TOPIC 2: BREAST SELF-EXAMINATION (BSE)
Definition
BSE is a self-screening method in which a woman examines her own breasts regularly to detect any changes, lumps, or abnormalities that may indicate a problem.
Purpose
- Early detection of breast lumps or changes
- Increases awareness of normal breast feel and appearance
- Helps identify signs that need medical attention
When to Perform BSE
- Premenopausal women: Monthly, 7-10 days after the onset of menstruation (when breasts are least tender and least swollen)
- Postmenopausal women: Monthly on a specific calendar date (easier to remember)
- Frequency: Once a month
The 7 Ps of Breast Examination (Essential Components)
| P | Meaning |
|---|---|
| Positions | Different body positions during examination |
| Palpation | Feeling the breast tissue |
| Pads of fingers | Use pads of three middle fingers for palpation |
| Pressure | Three levels - light, medium, deep |
| Perimeter | Cover entire breast area |
| Pattern of search | Systematic method - vertical stripe preferred |
| Patient education | Teaching the woman about BSE |
Step-by-Step BSE Technique
Step 1 - Inspection (Looking)
Stand or sit before a mirror in good light.
Look for:
- Asymmetry in size or shape
- Skin dimpling or puckering
- Nipple retraction or discharge
- Redness, swelling, or rash
Do these 3 positions:
- Arms at sides (normal relaxed position)
- Arms raised over head
- Hands pressed on hips (contracts pectoralis muscles - highlights dimpling)
- Bend forward and lean - check for any hanging irregularity
Step 2 - Palpation (Feeling) - Standing/Sitting
- Use fingers of the opposite hand
- Palpate each breast and axilla (armpit)
Step 3 - Palpation - Lying Down
- Lie flat on back
- Place a small pillow under the shoulder of the side being examined
- Use the pads of the three middle fingers of the opposite hand
- Apply three pressures:
- Light - skin surface
- Medium - mid breast tissue
- Deep - near the chest wall (ribs)
Step 4 - Pattern of Search
Cover the entire breast from:
- Top to bottom: Clavicle to inframammary fold
- Side to side: Sternum to latissimus dorsi (armpit)
Preferred pattern: Vertical Stripe (Up-and-Down method)
- Move fingers in vertical overlapping columns from top to bottom
- Better than concentric circular or radial methods (those miss the edges)
Step 5 - Nipple Examination
- Gently squeeze the nipple
- Note any discharge (clear, milky, bloody)
Tip: BSE can be performed while showering - soap and water increase sensitivity of palpation; the privacy of a shower may reduce anxiety.
What to Look/Feel For (Abnormal Signs - REFER Immediately)
- A new lump or thickening (especially if hard, painless, irregular border)
- Skin dimpling or puckering
- Nipple retraction (turning inward) that is new
- Bloody or unusual nipple discharge
- Redness, swelling, or warmth that doesn't resolve
- Change in breast size or shape
Nurse's Role in BSE Education
- Teach the technique during home visits, ANM clinics, health camps
- Demonstrate using a breast model or diagram
- Educate about the importance of monthly BSE
- Counsel women not to panic - most lumps are benign
- Ensure follow-up referral for any suspicious finding
- Document BSE education and findings in the family health record
TOPIC 3: MAINTENANCE OF RECORDS AND REPORTS
Definitions
Record: A written, permanent account of information about a patient, family, or community that has been assessed and managed. It is a legal document.
Report: A verbal or written account that communicates information about current events, status, or findings from one person/unit to another.
Purposes / Importance of Records and Reports
For Patient Care:
- Communication - ensures continuity of care between health workers
- Coordination - links different levels of care (sub-centre → PHC → CHC)
- Planning - helps nurses plan future visits and care
- Evaluation - track progress of individual and family health
For Administration:
- Statistical information - helps management make decisions on resource use
- Supervision - helps supervisors evaluate services rendered
- Legal protection - proof of care given
For Education:
- Teaching/learning - case studies and outcomes educate nursing staff
- Research - data from records used for community health research
Types of Records in Community Health Nursing
1. Cumulative / Continuing Records
- Systematic account of an individual's total history over time
- Time-saving and economical
- Allows review of long-term progress
2. Family Records - The Family Folder
- All health records of a family kept together in one folder
- Gives a complete picture of the family's health status
- Contains:
- Family demographic details (name, address, age, occupation)
- Socio-economic information
- Health status of each member
- Services received (immunizations, antenatal visits, treatments)
3. Registers (at Sub-Centre / PHC level)
| Register | Purpose |
|---|---|
| Eligible Couple Register | Track couples for family planning services |
| Sterilization and IUD Register | Record family planning procedures |
| MCH (Mother & Child Health) Card/Register | Track antenatal, postnatal, child health |
| Child Health Card/Register | Track immunization and growth |
| Birth and Death Register | Record vital events |
| Sub-Centre / PHC / Clinic Register | Daily OPD visits and services |
| Stock and Issue Register | Track medicines and supplies |
| Malaria/Filaria Blood Test Register | Track disease surveillance |
| Malaria Parasite Positive Case Register | Track malaria positive cases |
4. Diaries
- Diary of Health Worker Male (HWM) and Health Worker Female (HWF)
- Diary of Health Assistant (HA) Male and Female
- Record of daily field activities and visits
Types of Reports
A. Based on Format:
| Type | When Used |
|---|---|
| Oral Report | Immediate use, not permanent (e.g., handover between nurses) |
| Written Report | Permanent record, used by several personnel (e.g., daily reports, census) |
B. Reports Used in Community Setting (Returns):
- Monthly Report of HW (Male and Female)
- Complication Report of HW
- PHC Monthly Report
C. Reports Used in Hospital Setting:
- Change-of-Shift Report - nurse handover at shift change
- Transfer Report - when patient moves between wards/hospitals
- Incident Report - any unusual event (fall, medication error)
- Legal Report - for medico-legal cases
- 24-hour Report - overall ward summary
- Census Report - daily patient count
- Birth and Death Report - vital statistics
- Anecdotal Report - narrative account of specific observation
Principles of Good Record Keeping
A good record must be:
- Accurate - factual, no guesses
- Complete - all relevant details included
- Clear - legible, no ambiguous abbreviations
- Concise - brief but containing all important information
- Timely (Prompt) - written as soon as possible after the event
- Confidential - not shared with unauthorized persons
- Dated and signed - with name and designation of the nurse
Principles of a Good Report
A good report must be:
- Prompt - given at the right time
- Clear - easy to understand
- Concise - to the point
- Complete - includes all pertinent details
- Objective - based on facts, not opinions
Record Maintenance at Sub-Centre / PHC Level - Summary
| Level | Records Maintained |
|---|---|
| Sub-Centre | Family folder, MCH register, immunization register, eligible couple register, birth/death register, stock register, HW diary |
| PHC | All sub-centre records + OPD register, lab reports, monthly reports, PHC report |
| Community (Home) | Family folder, antenatal card, child health card, immunization card |
Quick Revision - Key Points
- Menstrual cycle: Average 28 days; 4 phases - menstrual, follicular (estrogen), ovulation (LH surge), luteal (progesterone)
- BSE: Monthly, 7-10 days after period starts; use 7 Ps; vertical stripe pattern preferred
- Records vs Reports: Record = permanent written document; Report = communication of current findings
- Family folder = most important record in community health nursing
- Good records: Accurate, complete, clear, concise, prompt, confidential, signed
Sources: Ganong's Review of Medical Physiology 26e; Costanzo Physiology 7e; Berek & Novak's Gynecology; INC CHN-I Syllabus
This is a shared conversation. Sign in to Orris to start your own chat.