
Screenshot_20260530_091859_Samsung Notes.jpg
Tell me what to do with this patient
Reading File
Searching PubMed
metastatic prostate cancer PSMA PET treatment guidelines 2024
Searching the Web
metastatic castration sensitive prostate cancer oligometastatic bony mets treatment 2025 EAU AUA guidelines
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12091045
Searching PubMed
metastatic hormone sensitive prostate cancer low volume ADT ARPI triplet therapy
Reading File
Reading Article
PMID: 41193370
I now have all the information needed for a comprehensive management plan. Here is a detailed clinical response:
Management Plan: Revabhai Patel, 76M - mHSPC with Bone Metastases
Clinical Summary from the PSMA PET-CT
| Finding | Detail |
|---|---|
| Primary | Prostatomegaly (37x45x46mm), PSMA-avid lesion (SUVmax 35.7), central + left half, abutting bladder neck, no SV/rectal invasion |
| Nodal | No loco-regional or distant nodal disease |
| Bone Mets | 2 sites: D12 vertebra (SUVmax 18.8) + sternal body (SUVmax 3.7) = sclerotic, low-volume metastatic disease |
| Visceral | None |
| Other | Incidental cystitis with small bladder diverticulum; spondylotic changes; marginally bulky left adrenal (non-PSMA expressive) |
Disease classification: de novo metastatic hormone-sensitive prostate cancer (mHSPC), LOW-VOLUME (fewer than 4 bone mets, no lesion outside axial skeleton, no visceral mets, by CHAARTED criteria)
Step-by-Step Management
1. Confirm Disease Status / Baseline Work-up
- Confirm castration status - obtain serum testosterone. If not already on ADT, this is de novo mHSPC.
- PSA: 24.5 ng/mL (14-05-26) - document as baseline
- Gleason/ISUP grade from biopsy - essential for risk stratification (LATITUDE criteria: Gleason ≥8, ≥2 bone lesions, visceral mets = high risk; this patient has only 2 bone lesions, so LATITUDE low risk)
- Labs: CBC, LFTs, RFTs, serum calcium, alkaline phosphatase, LDH, HbA1c (before starting steroids if abiraterone used)
- Bone densitometry (DEXA scan) - ADT causes bone loss; baseline needed
- Germline testing (BRCA1/2, ATM, etc.) + somatic tumor profiling - 2025 CUA guidelines give this a strong recommendation for all metastatic PCa; BRCA2 mutations may qualify for PARP inhibitor later
2. Primary Systemic Treatment - ADT + ARPI Doublet (Standard of Care for Low-Volume mHSPC)
Per 2026 AUA/SUO, 2025 CUA, and EAU 2026 guidelines, and confirmed by the 2026 European Urology living network meta-analysis (PMID 41193370):
In synchronous low-volume mHSPC, ARPI + ADT provides statistically significant OS benefit over ADT alone (HR 0.65; 95% CI 0.52-0.80). Adding docetaxel to ARPI+ADT does not improve OS in low-volume disease (HR 1.08; 0.65-1.79 - non-significant).
Recommended regimen:
ADT + one ARPI (doublet) - choose one of:
- Enzalutamide 160 mg/day orally (ARCHES/ENZAMET trial)
- Apalutamide 240 mg/day orally (TITAN trial)
- Darolutamide 600 mg twice daily orally (ARASENS/ARANOTE trials - new 2025 data)
- Abiraterone acetate 1000 mg/day + prednisone 5 mg twice daily (LATITUDE/STAMPEDE)
For a 76-year-old, darolutamide or apalutamide may be preferred due to a more favorable CNS/falls/seizure risk profile compared to enzalutamide - important in elderly patients.
ADT options:
- LHRH agonist (leuprolide/goserelin) - add bicalutamide 50mg x 2 weeks at initiation to prevent testosterone flare
- LHRH antagonist (degarelix/relugolix) - preferred in patients with cardiovascular risk or spine mets (no flare risk); relugolix (oral) offers convenience
Given D12 vertebral metastasis with high SUVmax (18.8), avoid testosterone flare - prefer LHRH antagonist or cover with bicalutamide.
Do NOT add docetaxel in this low-volume patient - no survival benefit, only toxicity in a 76-year-old.
3. Bone Health Management (Mandatory)
- Zoledronic acid 4 mg IV every 4 weeks (or denosumab 120 mg SC every 4 weeks) to prevent skeletal-related events (SREs)
- Calcium 1200 mg/day + Vitamin D 800-1000 IU/day supplementation (mandatory with bone-targeting agents)
- Dental review before starting bisphosphonate/denosumab (risk of osteonecrosis of the jaw)
- Monitor renal function before each zoledronate dose (contraindicated if GFR <30)
4. Prostate-Directed Radiotherapy - Consider in Low-Volume Disease
Per STAMPEDE and PEACE-1 data incorporated in 2026 AUA guidelines:
- In patients with low-volume mHSPC, addition of prostate radiotherapy (hypofractionated EBRT) to systemic therapy improved rPFS (HR=0.65 in PEACE-1 abiraterone arm)
- OS benefit was not proven, but radiotherapy is recommended as an option for low-volume mHSPC to delay progression
- This patient has no SV/rectal invasion and bladder neck abutment without infiltration - prostate RT is feasible
Discuss with radiation oncology for:
- Hypofractionated prostate EBRT (e.g., 36.25 Gy in 5 fractions, or 60 Gy in 20 fractions)
5. Stereotactic Body Radiotherapy (SBRT) to Bone Metastases
- Metastasis-directed therapy (MDT) with SBRT to D12 vertebra (high SUVmax 18.8 - high local risk) and sternum can be considered for local control and pain prevention
- D12 vertebral involvement - monitor for cord compression symptoms (back pain, neurological signs); urgent MRI spine if these develop
6. Monitoring Plan
- PSA every 3 months initially, then every 6 months on stable treatment
- Testosterone level to confirm castrate levels (<50 ng/dL or <1.7 nmol/L)
- Imaging: repeat PSMA PET-CT or bone scan at 6-12 months, or sooner if PSA rises or symptoms develop
- Metabolic monitoring: lipid profile, fasting glucose (on ARPI), blood pressure, LFTs (on abiraterone), ECG (enzalutamide carries seizure/fall risk)
- Watch for CRPC: PSA rising despite castrate testosterone on 2 consecutive measurements 1 week apart = CRPC - triggers next-line therapy planning
7. Incidental Findings to Address
- Cystitis with bladder diverticulum: urine culture, treat if infected; urological follow-up
- Mosaic perfusion pattern in bilateral lungs: low priority but consider respiratory review if symptomatic (likely chronic change)
- Left adrenal: non-PSMA expressive, marginally bulky - low suspicion; note and follow
- Spondylotic changes: physiotherapy, pain management as needed
8. MDT and Supportive Care
- Refer to Uro-oncology MDT: Urologist + Medical Oncologist + Radiation Oncologist + Nuclear Medicine
- Geriatric assessment given age 76: assess frailty, comorbidities, polypharmacy before ARPI initiation
- Counsel on ADT side effects: hot flashes, fatigue, loss of libido, gynecomastia, metabolic syndrome, osteoporosis, cardiac risk
- Psychosocial support and patient/family counseling about disease prognosis and goals of care
Summary Algorithm
mHSPC, LOW VOLUME, 76M
|
├─ Start ADT (LHRH antagonist preferred) + ARPI doublet
| (Darolutamide or Apalutamide preferred in elderly)
|
├─ Bone protection: Zoledronate + Ca/Vit D
|
├─ Discuss prostate EBRT (low-volume mHSPC benefit)
|
├─ Consider SBRT to D12 vertebra (high SUVmax lesion)
|
├─ Germline + somatic genomic testing
|
└─ 3-monthly PSA + castrate testosterone monitoring
Key references:
- 2026 AUA/SUO Advanced Prostate Cancer Guideline
- 2025 CUA-CUOG Guideline (PMID: PMC12091045)
- Riaz IB et al., Eur Urol 2026 - Living NMA by disease volume (PMID 41193370) - confirms doublet (not triplet) is optimal for low-volume synchronous mHSPC
- Smith and Tanagho's General Urology, 19th Ed., p. 426
Disclaimer: This is clinical decision support for a qualified treating physician. Final management must be individualized after full clinical assessment, patient preferences, comorbidities, and local drug availability.
So this will cure by only medicine no surgery required
This is an important question that needs a very honest answer.
No - This Cannot Be Cured
I have to be direct with you: metastatic prostate cancer (stage IV with bone metastases) is not curable with any current treatment - medicine, surgery, or otherwise.
Why Surgery Is Not the Answer Here
Once prostate cancer has spread to bones (D12 vertebra + sternum), removing the prostate surgically (radical prostatectomy) does not improve survival. The cancer is already "out of the box." Surgery would:
- Put a 76-year-old through major operative risk for zero survival benefit
- Not address the bone metastases at all
- Still leave him needing all the same systemic treatments afterward
Surgery is only potentially curative in localized prostate cancer (confined to the prostate). This patient is beyond that stage.
What Treatment Actually Does Here
The goal of treatment shifts from cure to control:
| Goal | What It Means |
|---|---|
| Control disease | Slow or stop cancer growth |
| Extend life | Patients on ADT + ARPI doublet can live several years - median OS in low-volume mHSPC trials exceeds 5-7 years |
| Maintain quality of life | Keep PSA low, prevent bone fractures, manage symptoms |
| Delay progression | Delay the cancer becoming resistant (castration-resistant) |
The Honest Prognosis
- Low-volume mHSPC (like this patient - only 2 bone lesions, no visceral spread) actually carries a relatively favorable prognosis among metastatic patients
- With ADT + ARPI doublet therapy, median overall survival in clinical trials has been 6-8+ years
- This patient may respond very well - PSA can drop dramatically (sometimes to undetectable) within months
- However, most patients eventually develop castration-resistant prostate cancer (CRPC) where the cancer grows despite low testosterone - this typically happens after a median of 2-3 years, at which point next-line therapies are available
The Right Mindset for This Patient
"We cannot cure this cancer, but we can control it for years, keep you feeling well, and continue to have active treatment options as the disease evolves."
This is a chronic disease management situation - similar to how diabetes or heart failure is managed long-term - not a one-time fix.
The priority now is to start ADT + ARPI as soon as possible, protect the bones, and monitor closely. Every month of delay allows further spread.
What is adt and arpi
Finding Sources
Finding Sources
Here is a clear, plain-language explanation:
The Core Concept: Prostate Cancer Feeds on Testosterone
Prostate cancer cells need testosterone (the male hormone) to grow and multiply. The entire strategy of ADT + ARPI is to cut off this fuel supply at two different points.
ADT - Androgen Deprivation Therapy
Simply put: Switch off testosterone production from the testicles
The testicles produce ~95% of the body's testosterone. ADT "switches them off" medically.
How it works:
Brain (Hypothalamus)
↓ releases GnRH/LHRH
Pituitary Gland
↓ releases LH
Testicles
↓ produce Testosterone
Cancer cells GROW
ADT blocks this chain at the pituitary level, so testosterone drops to near-zero ("castrate levels").
ADT drugs available in India:
| Drug | Type | How Given | Frequency |
|---|---|---|---|
| Leuprolide (Lupride, Eligard) | LHRH agonist | Injection | Monthly or 3-monthly |
| Goserelin (Zoladex) | LHRH agonist | Injection | Monthly or 3-monthly |
| Degarelix (Firmagon) | LHRH antagonist | Injection | Monthly |
| Relugolix (Orgovyx) | LHRH antagonist | Oral tablet | Daily |
For this patient (D12 vertebral met), prefer LHRH antagonist (degarelix/relugolix) - it drops testosterone immediately without a dangerous initial "flare" that can worsen spinal cord compression.
ADT side effects to warn patient about:
- Hot flashes
- Loss of sex drive
- Fatigue
- Weight gain
- Bone thinning (osteoporosis) - why we add zoledronate
- Mild memory/mood changes
ARPI - Androgen Receptor Pathway Inhibitor
Simply put: Block the lock that testosterone uses to enter cancer cells
Even after ADT drops testosterone very low, some residual androgen activity remains (from adrenal glands, or from within the tumor itself). Cancer cells also become "hypersensitive" to even tiny amounts of testosterone.
ARPI drugs block the androgen receptor - the "lock" on the cancer cell surface - so even the remaining testosterone cannot activate it.
Testosterone (very low after ADT)
↓
Androgen Receptor (the LOCK on cancer cell)
← ARPI BLOCKS THIS LOCK
Cancer cell cannot grow
ARPI drugs (choose ONE):
| Drug | Brand Name | Dose | Notes |
|---|---|---|---|
| Enzalutamide | Xtandi | 160 mg/day oral | Avoid in seizure history, fall risk in elderly |
| Apalutamide | Erleada | 240 mg/day oral | Good safety profile |
| Darolutamide | Nubeqa | 600 mg twice daily oral | Best CNS safety - preferred in elderly like this patient |
| Abiraterone | Zytiga/Abiratas | 1000 mg/day oral | Blocks adrenal androgen production; needs prednisone with it |
For a 76-year-old like this patient, darolutamide is preferred - it does not cross the blood-brain barrier well, so lower risk of falls, dizziness, and seizures compared to enzalutamide.
The Combination - Why Both Together?
Think of it this way:
| ADT alone | Turns off the main testosterone factory (testicles) |
| ADT + ARPI | Turns off the factory AND blocks the door of every cancer cell |
Clinical trials show that doublet therapy (ADT + ARPI) extends life by 2-3+ years compared to ADT alone in low-volume metastatic prostate cancer.
Practical Starting Plan for This Patient
Day 1:
→ Degarelix 240mg SC (loading dose) - immediate testosterone suppression
→ Start Darolutamide 600mg twice daily orally
→ Start Zoledronate 4mg IV (bone protection)
→ Calcium + Vitamin D daily
Month 1 onwards:
→ Degarelix 80mg SC monthly
→ Continue Darolutamide daily
→ Check PSA + Testosterone at 3 months
- PSA should fall significantly (often >90% drop)
- Testosterone should be <50 ng/dL (castrate level)
Bottom line: ADT kills the testosterone supply. ARPI blocks the receptor the cancer uses. Together, they are the most effective non-surgical treatment available for this stage of prostate cancer - and for a low-volume patient like this, the response is often very good for several years.
Without medicine how long will patient survive only on some basic medicine
Finding Sources
Searching PubMed
untreated metastatic prostate cancer survival natural history no treatment
Here is the honest, direct answer:
Survival Without Proper Treatment
The Short Answer:
Without ADT-based treatment, a patient with metastatic prostate cancer and bone metastases typically survives 1 to 2 years. With only basic/supportive medicines (painkillers, antibiotics, etc.) but no hormone therapy - the cancer will progress steadily and cause death primarily from bone complications and disease spread.
What Happens Without Treatment - The Timeline
Months 0-6:
PSA continues rising rapidly
Bone lesions enlarge and multiply
Bone pain begins (especially back pain from D12 vertebra)
Months 6-12:
Severe bone pain requiring strong opioids
D12 vertebral lesion enlarges → risk of SPINAL CORD COMPRESSION
(sudden paralysis of legs - a medical emergency)
Pathological fractures (bone breaks spontaneously without injury)
Fatigue, weight loss, anemia
Months 12-24:
Cancer spreads to more bones, possibly liver/lungs
Hypercalcemia (high calcium from bone destruction - causes confusion)
Urinary obstruction from prostate enlarging further
Kidney failure (from ureteric obstruction or hypercalcemia)
Death - typically from:
→ Complications of bone metastases
→ Infection/sepsis
→ Organ failure
Comparison - With vs Without Treatment
| No Treatment | ADT only | ADT + ARPI (recommended) | |
|---|---|---|---|
| Median survival | ~12-18 months | ~3-4 years | 6-8+ years |
| Quality of life | Rapidly deteriorating | Reasonably maintained | Well maintained for years |
| Bone pain | Severe, progressive | Controlled | Well controlled |
| Paralysis risk | High (D12 met) | Low | Very low |
The Most Dangerous Risk for THIS Patient Specifically
The D12 vertebral metastasis with SUVmax 18.8 (very active lesion) is sitting on the spine. Without treatment:
Spinal cord compression can happen suddenly - the patient wakes up one morning unable to move his legs. This is irreversible if not treated within hours. It is one of the most feared complications of untreated spinal bone mets.
This alone is a strong reason to start treatment urgently - not just for survival, but to prevent devastating disability.
Why Families Sometimes Hesitate
I understand the concerns - cost, side effects, age (76 years), and wondering "is it worth it at this age?" These are valid questions. The honest answers are:
- Age 76 is not too old - many 76-year-olds live active lives for another 10+ years
- ADT injections are well tolerated - not like chemotherapy; no hair loss, no severe nausea
- The cost of not treating is much worse - severe pain, paralysis, hospital admissions are far more expensive and distressing than preventive treatment
- Quality of life on treatment is significantly better than without it
Bottom Line
| Scenario | Expected Outcome |
|---|---|
| No treatment at all | 12-18 months, with significant suffering |
| Basic medicines only (painkillers, etc.) | Same - pain is managed but cancer keeps growing |
| ADT + ARPI (proper treatment) | 6-8+ years, with good quality of life |
Starting treatment now gives this patient the best chance of several more good years of life. The difference between treating and not treating is not months - it is years.
How d12 is bad in this patient
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Excellent - here is a thorough explanation with the actual textbook MRI image for reference:
Why D12 (T12) is Dangerous in This Patient
First - Where is D12?
D12 = Dorsal 12th vertebra = same as T12 (12th thoracic vertebra). It sits at the very bottom of the thoracic spine, just above the lumbar region - roughly at the level of your lower ribcage.
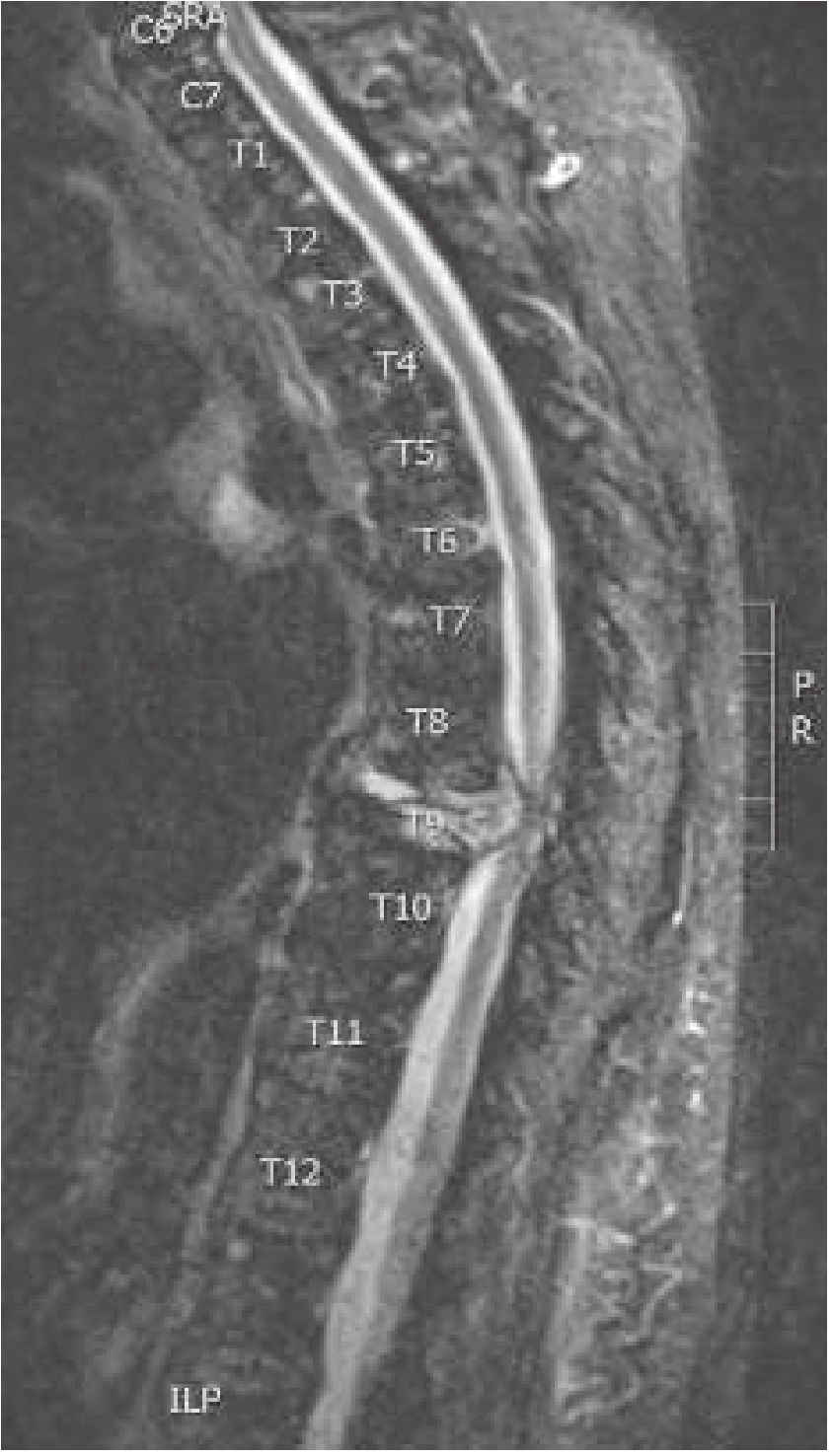
The Anatomy - Why This Location is Critical
Spinal Cord ends at approximately L1-L2
(called the CONUS MEDULLARIS)
D12/T12 is right above this termination point
T10 ─── Spinal cord running here
T11 ─── Spinal cord running here
T12 ─── ← THIS PATIENT'S METASTASIS (SUVmax 18.8)
L1 ─── Conus medullaris (tip of spinal cord)
L2 ─── Cauda equina begins
D12 is one of the most dangerous sites for metastasis because:
- The spinal canal is narrowest in the thoracic region - very little room for any extra mass
- D12 sits right at the conus medullaris - the most critical junction of the entire spinal cord
- Damage here causes both upper and lower motor neuron signs simultaneously
What Happens When the D12 Met Grows
Step 1: Cancer cells in D12 vertebral body multiply (SUVmax 18.8 = very metabolically active = growing fast)
Step 2: The vertebral body weakens from inside - pathological fracture risk (bone breaks without any injury, just from body weight)
Step 3: Fractured/expanded vertebra pushes backwards into the spinal canal
Step 4: This compresses the spinal cord = Metastatic Spinal Cord Compression (MSCC)
Normal: With met growing:
[vertebra][cord][space] [collapsed vertebra ──→ CORD SQUEEZED]
What MSCC at D12 Causes - The Warning Signs
The patient or family must be told to go to emergency immediately if any of these appear:
| Symptom | What It Means |
|---|---|
| New or worsening back pain (worse when lying down, worse with coughing) | Earliest warning - 95% of MSCC |
| Weakness in both legs | Cord being compressed - urgent |
| Numbness/tingling in legs or abdomen | Sensory tracts compressed |
| Difficulty walking / feeling unsteady | Motor + spinocerebellar tract involvement |
| Unable to pass urine / urinary retention | Autonomic involvement - late sign, EMERGENCY |
| Constipation / loss of bowel control | Autonomic involvement - late sign, EMERGENCY |
Back pain that is WORSE LYING DOWN is the classic red flag - this is the opposite of disc pain (which is better lying down). In a cancer patient, this pattern = spinal met until proven otherwise.
If MSCC Happens - Time is Everything
MSCC develops
↓
<24 hours: Patient can still walk → treat urgently → good chance of recovery
↓
24-48 hours: Partial weakness → treat now → partial recovery possible
↓
>48 hours complete paralysis: Permanent paralysis very likely
↓
No treatment: Permanent paraplegia (cannot walk ever again)
Once the patient loses the ability to walk, the window to reverse it is measured in HOURS, not days.
Emergency Treatment if MSCC Occurs
- IV Dexamethasone 10mg bolus immediately - reduces edema around cord, buys time
- Urgent MRI whole spine - to confirm level and extent
- Emergency radiotherapy (SBRT/EBRT) to D12 - best option for this patient
- Neurosurgical decompression - if bone collapse is causing direct mechanical compression
What to Do NOW (Preventively)
Since the lesion is already present and active (SUVmax 18.8) but the patient presumably has no paralysis yet:
- Start systemic treatment (ADT + ARPI) urgently - shrinks the met over weeks to months
- Refer to Radiation Oncology for prophylactic SBRT to D12 - local radiotherapy to this specific vertebra to kill the cancer cells there and prevent collapse
- Educate patient and family about the warning signs above
- MRI spine (whole spine) - to see if any cord indentation is already happening that the PET-CT may not have fully captured
Bottom line: D12 is bad because a 76-year-old man with active cancer eating his 12th thoracic vertebra is one fracture or one week of unchecked growth away from permanent paralysis of both legs. This is the single most urgent reason to not delay treatment. - Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine
What about sternum
Finding Sources
Finding Sources
Here is the full explanation - and the honest comparison with D12:
Sternal Body Metastasis - This Patient's Findings
From the PET-CT report:
- Sternal body: sclerotic lesion, SUVmax 3.7
- Compare to D12: SUVmax 18.8
This difference in SUVmax is very telling.
What the Sternum Is and Why It Matters Less (But Still Matters)
Anatomy of the Sternum
Manubrium (top)
│
Sternal body ← THIS PATIENT'S MET
│
Xiphoid process (bottom)
Behind the sternum:
Heart (anterior surface)
Great vessels (aorta, SVC)
Thymus / anterior mediastinum
The sternum is a flat bone sitting in the front of the chest, acting like a shield. It is rich in red bone marrow - which is exactly why cancer cells love to lodge there. Prostate cancer has a particular preference for axial skeleton bones (spine, sternum, ribs, pelvis) because of their rich marrow blood supply.
Why the Sternal Met is LESS Dangerous Than D12
| Factor | D12 Vertebra | Sternal Body |
|---|---|---|
| SUVmax | 18.8 (very active) | 3.7 (relatively low activity) |
| Adjacent critical structure | Spinal cord | Heart / mediastinum |
| Risk if it grows | Paralysis | Chest pain, rarely cardiac |
| Risk of catastrophic complication | HIGH - cord compression | LOW - no cord nearby |
| Fracture consequence | Collapse → paraplegia | Pain, deformity only |
| Urgency | URGENT | Less urgent |
The sternal met is essentially in an "open" space - there is no delicate neural tissue immediately behind it that can be crushed. A growing sternal lesion causes:
- Local pain - anterior chest pain / tenderness on pressing the sternum
- Pathological fracture of the sternum - painful but not life-threatening
- In extreme cases of very large lesion - could theoretically encroach on the pericardium or great vessels, but this is rare and would take a very long time
The SUVmax 3.7 - What Does It Mean?
SUVmax is a measure of how much radioactive tracer (PSMA) the lesion is consuming - a proxy for how metabolically active / aggressive the lesion is.
SUVmax 3.7 → Low-moderate PSMA avidity
Sclerotic (bone hardening reaction)
Relatively indolent/slow-growing lesion
SUVmax 18.8 → Very high PSMA avidity
Highly active cancer deposit
Growing fast, high risk
A sclerotic lesion with low SUVmax actually suggests the bone is reacting and trying to heal/wall off the cancer - this is a relatively favorable sign compared to lytic (bone-destroying) lesions.
Symptoms to Watch For from the Sternum Met
Not dangerous in the same way as D12, but the patient may experience:
| Symptom | Cause |
|---|---|
| Tenderness when pressing the chest bone | Local periosteal involvement |
| Dull aching anterior chest pain | Bone pain from met |
| Pain on deep breathing | Rib-sternal junction involvement |
These are manageable with:
- NSAIDs (if renal function allows) or paracetamol for mild pain
- Opioids (tramadol/morphine) if pain is significant
- Local radiotherapy (SBRT) if pain becomes troublesome and uncontrolled
Should SBRT Be Given to the Sternum Too?
- If the patient is asymptomatic from the sternum - systemic treatment (ADT + ARPI) alone is sufficient; the met will likely shrink/stabilize
- If he develops significant sternal pain that is not controlled by oral analgesics - then palliative radiotherapy (single fraction 8 Gy or 20 Gy in 5 fractions) to the sternum gives excellent pain relief in >70% of patients
- No urgency like D12
Summary - Comparing Both Mets
D12 Vertebra (SUVmax 18.8) Sternal Body (SUVmax 3.7)
──────────────────────────── ──────────────────────────
⚠️ HIGH URGENCY ✓ LOW-MODERATE CONCERN
Spinal cord immediately behind No neural tissue nearby
Paralysis risk if untreated Pain / fracture risk only
Needs prophylactic SBRT NOW Treat only if symptomatic
Most dangerous lesion in this pt "Watch and treat if needed"
The sternum met confirms this is truly metastatic disease and justifies systemic therapy, but it is not going to paralyse him or cause an emergency. The D12 lesion is the one that demands urgency.

20260612_102132.jpg
What to do to get good healthy fresh younger skin in this
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.