Natural history or spectrum of atherosclerosis
Reading File
search_medical_text
natural history spectrum atherosclerosis pathogenesis progression
search_medical_image
atherosclerosis plaque progression stages spectrum diagram
GradeResponse
GradeResponse
Here is a comprehensive account of the natural history and spectrum of atherosclerosis, integrating retrieved sources with established pathophysiological knowledge.
Natural History & Spectrum of Atherosclerosis
Atherosclerosis is a chronic, progressive inflammatory disease of large and medium-sized arteries that begins silently in early life and culminates in potentially fatal clinical events decades later.
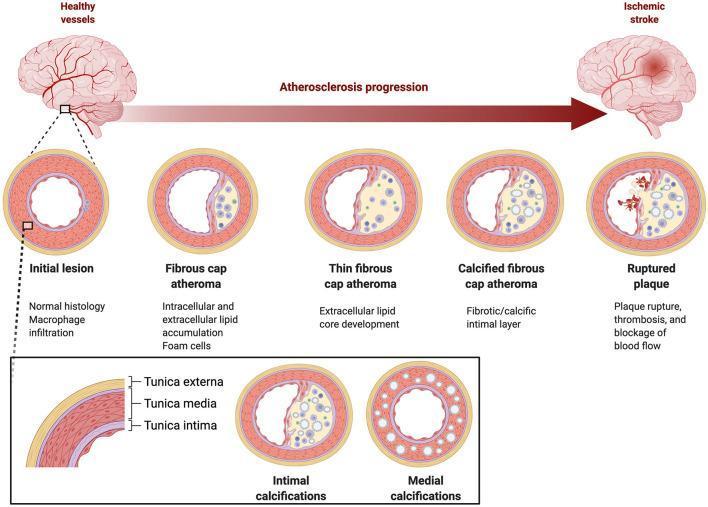
Stages of Progression
The natural history follows a well-defined morphological continuum:
1. Endothelial Dysfunction (Earliest Change)
- Triggered by risk factors: hyperlipidemia, hypertension, smoking, diabetes, oxidative stress
- Endothelial cells upregulate adhesion molecules (VCAM-1, ICAM-1)
- Increased permeability to LDL particles
- No visible lesion at this stage — purely functional
2. Fatty Streak
- LDL enters the intima and undergoes oxidative modification (ox-LDL)
- Monocytes adhere, migrate into the intima, and differentiate into macrophages
- Macrophages engulf ox-LDL → become foam cells (lipid-laden)
- Fatty streaks are flat, yellow, lipid-rich deposits visible as early as the first decade of life
- Found even in children and teenagers at autopsy
- Potentially reversible at this stage
3. Intermediate Lesion (Gelatinous Plaque)
- Smooth muscle cells migrate from tunica media → intima (driven by PDGF, FGF)
- Extracellular lipid accumulates alongside intracellular foam cells
- Early fibrous tissue deposition begins
4. Fibrous Plaque (Atheroma)
- A fibrous cap forms over a lipid-rich necrotic core
- Cap composed of smooth muscle cells, collagen, and proteoglycans
- Plaque enlarges and begins to encroach on the lumen
- Clinically silent — does not cause symptoms until lumen narrows >70%
- Stable angina may appear at this stage
5. Complicated Plaque
The most clinically dangerous stage. Several sub-types:
| Feature | Description |
|---|---|
| Calcification | Calcium deposits within the plaque; marker of advanced disease; detected by coronary calcium scoring (CAC) |
| Ulceration | Erosion of fibrous cap surface; thrombus-prone |
| Hemorrhage into plaque | Intraplaque hemorrhage from vasa vasorum rupture; rapid volume expansion |
| Plaque rupture | Rupture of thin fibrous cap → exposure of lipid core → platelet activation → acute thrombosis → ACS/MI/stroke |
| Plaque erosion | Thrombosis without frank rupture; more common in women and younger patients |
AHA Lesion Classification (Stary Classification)
| Type | Name | Hallmark |
|---|---|---|
| I | Initial lesion | Isolated foam cells |
| II | Fatty streak | Layers of foam cells |
| III | Intermediate lesion | Extracellular lipid pools |
| IV | Atheroma | Confluent lipid core |
| V | Fibroatheroma | Fibrous cap over lipid core |
| VI | Complicated lesion | Surface defect, hematoma, thrombus |
| VII | Calcified lesion | Predominantly calcium |
| VIII | Fibrotic lesion | Fibrous tissue, little lipid |
Temporal Spectrum: Birth to Clinical Event
Childhood Adolescence 20s–40s 40s–60s+
| | | |
Fatty streak → Fibrous plaque → Complicated → Clinical Event
(asymptomatic) (asymptomatic) plaque (ACS, stroke,
(silent or PAD, aneurysm)
angina)
- Childhood: Fatty streaks in aorta
- Adolescence/Young adulthood: Fatty streaks in coronary arteries (found in trauma autopsies of soldiers in Korea and Vietnam wars)
- Middle age: Raised fibrous plaques; coronary artery disease may become symptomatic
- Advanced age: Complicated plaques with calcification, stenosis, thrombosis
Clinical Manifestations by Vascular Territory
| Territory | Stable Disease | Acute Event |
|---|---|---|
| Coronary arteries | Stable angina, silent ischemia | STEMI, NSTEMI, sudden cardiac death |
| Cerebral/carotid | TIA, amaurosis fugax | Ischemic stroke |
| Peripheral arteries | Intermittent claudication | Critical limb ischemia, gangrene |
| Renal arteries | Renovascular hypertension | Renal infarction |
| Mesenteric arteries | Post-prandial angina | Mesenteric ischemia |
| Aorta | Asymptomatic AAA | Aortic dissection, rupture |
Key Concepts in Natural History
Vulnerable Plaque vs. Vulnerable Patient
- A vulnerable (high-risk) plaque has: thin fibrous cap (<65 µm), large lipid core (>40% of plaque volume), intraplaque inflammation, positive remodeling
- A vulnerable patient has: multiple vulnerable plaques, systemic inflammation, hypercoagulable state
- Most ACS events arise from non-flow-limiting plaques (<50% stenosis) — this is why angiography alone underestimates risk
Plaque Regression
- Aggressive LDL lowering (statins, PCSK9 inhibitors) can induce plaque regression — reduction in noncalcified plaque volume
- Coronary CT Angiography (CCTA) studies show: in patients with LDL reduction >10%, regression of all noncalcified plaque components occurs; without LDL reduction, progression occurs across all components (Coronary CT Imaging of Atherosclerotic Plaque, p. 11)
- Plaque progression by serial CCTA is an independent predictor of ACS (HR: 33.4), with events in 14.3% of progressors vs. 0.3% of non-progressors (Coronary CT Imaging, p. 11)
Rate of Progression
- Annualized increase in total coronary plaque volume: ~50 mm³/year in diabetics vs. ~21 mm³/year in non-diabetics
- Noncalcified plaque grows far faster in diabetics (~31 mm³/year) vs. non-diabetics (~2.5 mm³/year) (Coronary CT Imaging, p. 11)
Response-to-Injury Hypothesis (Ross)
The dominant paradigm: endothelial injury → lipid infiltration → inflammatory response → smooth muscle proliferation → fibrosis → plaque formation. Atherosclerosis is fundamentally an inflammatory disease, not merely a lipid storage disorder.
Risk Factor Influence on Natural History
| Risk Factor | Effect on Progression |
|---|---|
| Hyperlipidemia (high LDL) | Accelerates all stages |
| Diabetes mellitus | Markedly accelerates noncalcified plaque growth |
| Hypertension | Promotes endothelial injury, plaque rupture |
| Smoking | Oxidative stress, endothelial dysfunction, plaque destabilization |
| Age/male sex | Independent accelerants |
| Inflammation (high CRP) | Predicts future events independent of lipids |
Summary
Atherosclerosis spans a lifetime continuum — from invisible endothelial dysfunction and fatty streaks in childhood, through decades of clinically silent fibrous plaque accumulation, to the acute complications (plaque rupture, thrombosis) that manifest as heart attacks, strokes, and peripheral vascular disease. The transition from stable to unstable disease is governed more by plaque composition and inflammation than by degree of stenosis, which is why vulnerable plaques causing <50% obstruction account for the majority of acute coronary events.
This is a shared conversation. Sign in to Orris to start your own chat.