Can u expalain about thyrodism
Reading File
Finding Sources
Searching the Web
thyroid disorders hypothyroidism hyperthyroidism overview 2024
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced information to write a complete answer. Let me compile everything.
Thyroid Disorders (Thyroidism) - A Complete Guide
The term "thyroidism" refers broadly to disorders of the thyroid gland - a butterfly-shaped gland sitting below the larynx in the neck. It produces two key hormones, thyroxine (T4) and triiodothyronine (T3), which regulate metabolism, growth, heart rate, body temperature, and energy levels throughout the body.
Anatomy & Normal Physiology
The thyroid consists of two lobes joined by an isthmus. Inside, it is made up of follicles - tiny sacs lined by epithelial cells that produce thyroglobulin, an iodinated protein that is the precursor to thyroid hormones.
The control system works via a feedback loop:
- The hypothalamus releases TRH (thyrotropin-releasing hormone)
- TRH signals the pituitary to release TSH (thyroid-stimulating hormone)
- TSH stimulates the thyroid to produce T3 and T4
- T3/T4 in the blood then feed back to suppress TRH and TSH - keeping levels balanced
Most T4 in the blood is converted to the more active T3 in peripheral tissues. T3 binds to nuclear receptors and regulates hundreds of genes - the net effect is an increase in the basal metabolic rate.
Robbins & Kumar Basic Pathology, p. 729
Main Types of Thyroid Disorders
1. Hyperthyroidism (Overactive Thyroid)
Elevated thyroid hormones cause a hypermetabolic state called thyrotoxicosis.
Three most common causes:
- Graves' disease (~85% of cases) - autoimmune; antibodies mimic TSH and continuously stimulate the thyroid
- Toxic multinodular goiter - multiple autonomously functioning nodules
- Toxic adenoma - a single hyperfunctioning nodule
Clinical Features:
| System | Symptoms/Signs |
|---|---|
| Constitutional | Warm, flushed skin; heat intolerance; excessive sweating; weight loss despite increased appetite |
| Cardiac | Palpitations, tachycardia, risk of atrial fibrillation and heart failure in older patients |
| GI | Diarrhea, hypermotility, malabsorption |
| Neuromuscular | Anxiety, tremor, irritability, proximal muscle weakness (~50% of patients) |
| Ocular | Wide staring gaze, lid lag (especially prominent in Graves' disease - exophthalmos) |
Emergencies:
- Thyroid storm - abrupt severe hyperthyroidism, often triggered by infection, surgery, or stress. Medical emergency with high mortality from cardiac arrhythmias.
- Apathetic hyperthyroidism - seen in elderly patients; typical features are blunted; presents as unexplained weight loss or worsening heart disease.
Diagnosis: TSH is the single best screening test - it is low/suppressed in hyperthyroidism. Free T4 (and sometimes T3) are elevated. Radioactive iodine uptake scan helps identify the cause.
Robbins & Kumar Basic Pathology, p. 729-730
2. Hypothyroidism (Underactive Thyroid)
Deficient thyroid hormone production causes a hypometabolic state.
Causes:
| Category | Examples |
|---|---|
| Autoimmune | Hashimoto thyroiditis (most common in iodine-sufficient regions) |
| Iodine deficiency | Most common cause worldwide - affects ~2 billion people |
| Iatrogenic | Thyroid surgery, radioactive iodine treatment, drugs (lithium, amiodarone) |
| Congenital | Thyroid dysgenesis, enzyme defects |
| Central (rare) | Pituitary or hypothalamic failure |
Clinical Features by Age:
- Congenital/Neonatal (Cretinism): If untreated, leads to severe intellectual disability, short stature, coarse facial features, protruding tongue, umbilical hernia. The earlier in pregnancy, the worse the outcome.
- Adults (Myxedema): Fatigue, apathy, mental sluggishness (can mimic depression), constipation, cold intolerance, weight gain, cool/pale skin, bradycardia, deepening voice, non-pitting edema (from accumulation of glycosaminoglycans in tissues), elevated LDL cholesterol.
- Myxedema Coma - life-threatening extreme hypothyroidism: hypothermia, bradycardia, altered consciousness. A medical emergency.
Diagnosis: TSH is elevated in primary hypothyroidism (pituitary is trying harder to stimulate an underperforming thyroid). Free T4 is low.
Robbins & Kumar Basic Pathology, p. 730
3. Autoimmune Thyroid Disease
Hashimoto Thyroiditis (Chronic Lymphocytic Thyroiditis):
- Most common cause of hypothyroidism in iodine-sufficient areas
- Female:male ratio of 10-20:1; peaks at age 45-65
- Mechanism: CD8+ cytotoxic T cells and cytokines destroy thyroid follicular cells; anti-TPO and anti-thyroglobulin antibodies are present in nearly all patients
- The thyroid shows dense lymphocytic infiltration with germinal center formation
Graves' Disease:
- Most common cause of hyperthyroidism
- TSH-receptor-stimulating antibodies (TRAb) continuously activate the thyroid
- Classic triad: hyperthyroidism + goiter + exophthalmos (eye bulging)
Subacute (de Quervain) Thyroiditis:
- Likely post-viral; painful thyroid, fever, transient hyperthyroidism followed by hypothyroidism, then usually full recovery
4. Goiter
Enlargement of the thyroid gland. Can be:
- Simple/non-toxic goiter - from iodine deficiency or increased demand (e.g., puberty, pregnancy)
- Multinodular goiter - multiple nodules, may be toxic (overactive) or non-toxic
5. Thyroid Cancer
Less common but important. Main types:
- Papillary carcinoma (~80%) - most common, best prognosis, spreads to lymph nodes
- Follicular carcinoma - spreads via blood; good prognosis if caught early
- Medullary carcinoma - from C-cells (parafollicular), may be associated with MEN2 syndrome
- Anaplastic carcinoma - rare, very aggressive
Treatment Overview
Hyperthyroidism Treatment:
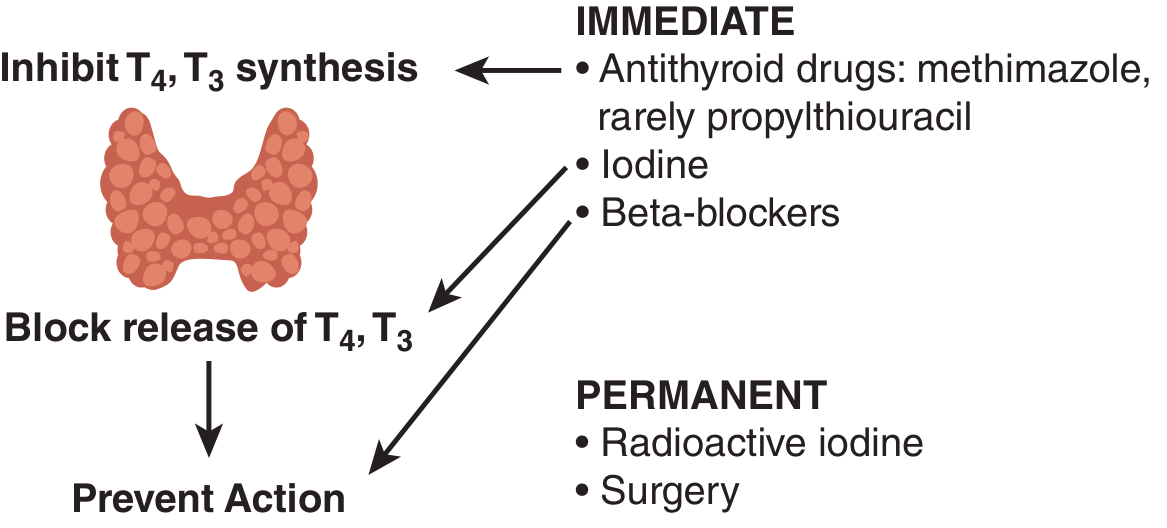
| Treatment | Notes |
|---|---|
| Antithyroid drugs (methimazole, propylthiouracil) | Block thyroid peroxidase; ~50% remission rate in Graves'; methimazole preferred except in thyroid storm or first trimester of pregnancy |
| Beta-blockers (propranolol) | Rapid symptom relief (tremor, palpitations); propranolol also reduces T3 by ~20% |
| Radioactive iodine (¹³¹I) | 75-90% cure rate; up to 80% risk of eventual hypothyroidism |
| Surgery (thyroidectomy) | Definitive cure; results in permanent hypothyroidism requiring lifelong T4 replacement |
Goldman-Cecil Medicine
Hypothyroidism Treatment:
- Levothyroxine (synthetic T4) is the standard treatment - taken once daily, adjusted to normalize TSH
- Lifelong therapy is usually required
- Doses must be increased during pregnancy
Quick Comparison Summary
| Feature | Hyperthyroidism | Hypothyroidism |
|---|---|---|
| Metabolism | Increased (hypermetabolic) | Decreased (hypometabolic) |
| Weight | Loss | Gain |
| Heart rate | Fast (tachycardia) | Slow (bradycardia) |
| Temperature tolerance | Heat intolerance | Cold intolerance |
| Skin | Warm, moist, flushed | Cool, dry, pale |
| Bowel | Diarrhea | Constipation |
| Mood/Nervous system | Anxious, tremor, irritable | Sluggish, depressed, slow |
| TSH level | LOW (suppressed) | HIGH (elevated) |
| T3/T4 levels | HIGH | LOW |
| Main cause | Graves' disease | Hashimoto thyroiditis / Iodine deficiency |
Sources:
- Robbins & Kumar Basic Pathology, pp. 729-731
- Goldman-Cecil Medicine (International Edition)
- Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.