Hypertension
python3 -c " import pdfplumber with pdfplumber.open('/tmp/workspace/attachments/18e5d6af-1f11-4d1f-908d-c4a5e8476c06/hypertension.pdf') as pdf: print(f'Pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages[:3]): text = page.extract_text() if text: print(f'--- Page {i+1} ---') print(text[:1500]) "
python3 -c " from pypdf import PdfReader reader = PdfReader('/tmp/workspace/attachments/18e5d6af-1f11-4d1f-908d-c4a5e8476c06/hypertension.pdf') print(f'Pages: {len(reader.pages)}') for i, page in enumerate(reader.pages[:5]): text = page.extract_text() print(f'--- Page {i+1} (chars: {len(text) if text else 0}) ---') if text: print(text[:1000]) else: print('[No extractable text - may be scanned/image-based]') "
python3 -c " from pypdf import PdfReader import base64, json reader = PdfReader('/tmp/workspace/attachments/18e5d6af-1f11-4d1f-908d-c4a5e8476c06/hypertension.pdf') print(f'Total pages: {len(reader.pages)}') # Check if pages have images embedded for i, page in enumerate(reader.pages[:5]): imgs = page.images print(f'Page {i+1}: {len(imgs)} images') if imgs: for j, img in enumerate(imgs): print(f' Image {j}: name={img.name}, size={len(img.data)} bytes') "
ls /tmp/workspace/attachments/ 2>/dev/null || echo "attachments dir not found"; ls /tmp/workspace/ 2>/dev/null
find / -name "hypertension.pdf" 2>/dev/null | head -5
- Goldman-Cecil Medicine - clinical presentation, diagnosis, and treatment
- Guyton & Hall Physiology - pathophysiological mechanisms
- Robbins Pathology - vascular pathology and histology
- Brenner & Rector's The Kidney - renal mechanisms
Make it easy and in points and flow chart so that I can learn it easily
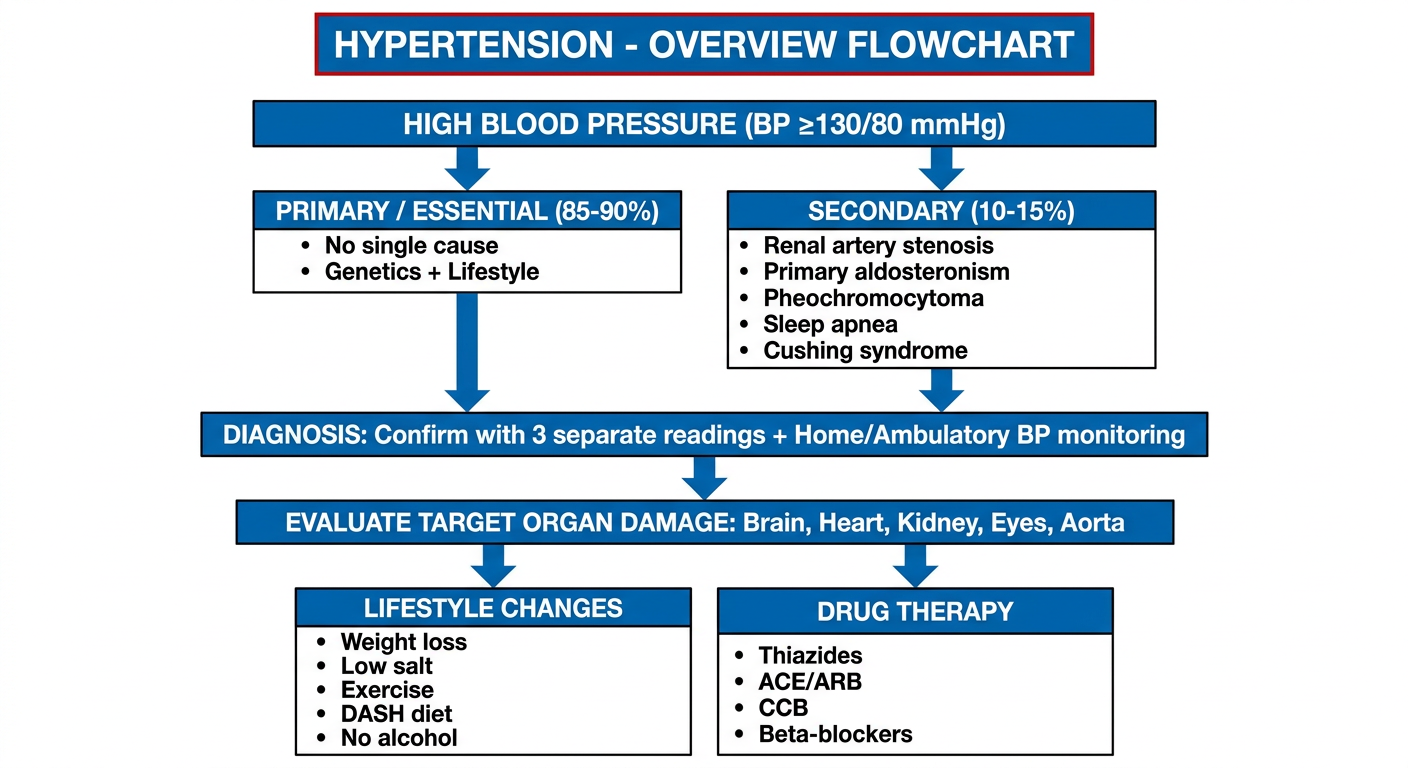
A clean medical flowchart titled "HYPERTENSION - OVERVIEW FLOWCHART" with the following flow: Starting box "HIGH BLOOD PRESSURE (BP ≥130/80 mmHg)" arrows down to two boxes side by side: "PRIMARY / ESSENTIAL (85-90%)" and "SECONDARY (10-15%)". Under PRIMARY: bullet points "No single cause", "Genetics + Lifestyle". Under SECONDARY: bullet points "Renal artery stenosis", "Primary aldosteronism", "Pheochromocytoma", "Sleep apnea", "Cushing syndrome". Both boxes have arrows pointing down to a center box "DIAGNOSIS: Confirm with 3 separate readings + Home/Ambulatory BP monitoring". Then arrow down to "EVALUATE TARGET ORGAN DAMAGE: Brain, Heart, Kidney, Eyes, Aorta". Then arrow down to two side-by-side boxes: "LIFESTYLE CHANGES" (Weight loss, Low salt, Exercise, DASH diet, No alcohol) and "DRUG THERAPY" (Thiazides, ACE/ARB, CCB, Beta-blockers). White background, blue and red color scheme, clear bold text, medical education style.
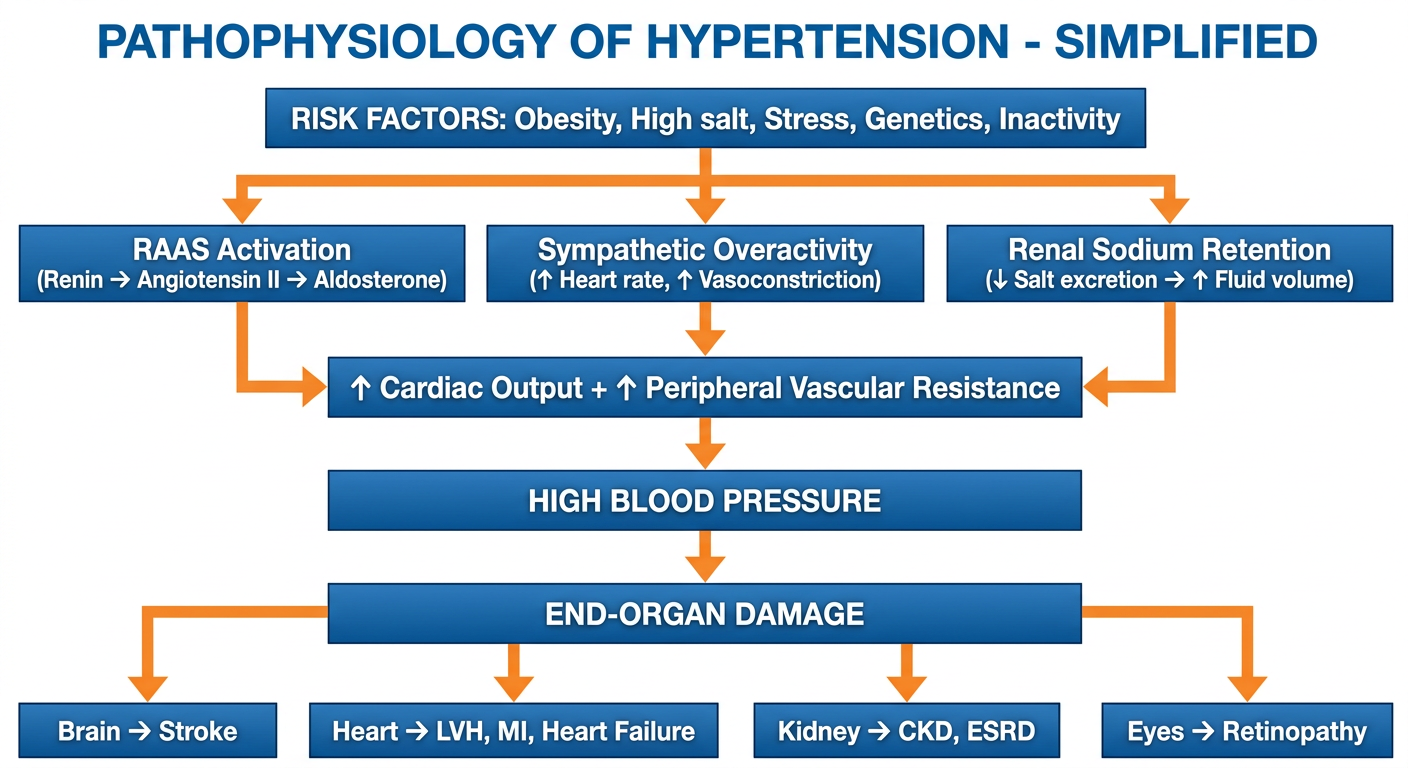
A clean medical education flowchart titled "PATHOPHYSIOLOGY OF HYPERTENSION - SIMPLIFIED" showing a cascade flow. Top box: "RISK FACTORS: Obesity, High salt, Stress, Genetics, Inactivity". Arrow down to three parallel boxes: "RAAS Activation (Renin → Angiotensin II → Aldosterone)", "Sympathetic Overactivity (↑ Heart rate, ↑ Vasoconstriction)", "Renal Sodium Retention (↓ Salt excretion → ↑ Fluid volume)". All three boxes have arrows converging into one box: "↑ Cardiac Output + ↑ Peripheral Vascular Resistance". Arrow down to "HIGH BLOOD PRESSURE". Arrow down to "END-ORGAN DAMAGE" with four branches: "Brain → Stroke", "Heart → LVH, MI, Heart Failure", "Kidney → CKD, ESRD", "Eyes → Retinopathy". White background, clean arrows, blue-orange color scheme, bold text, medical student friendly.
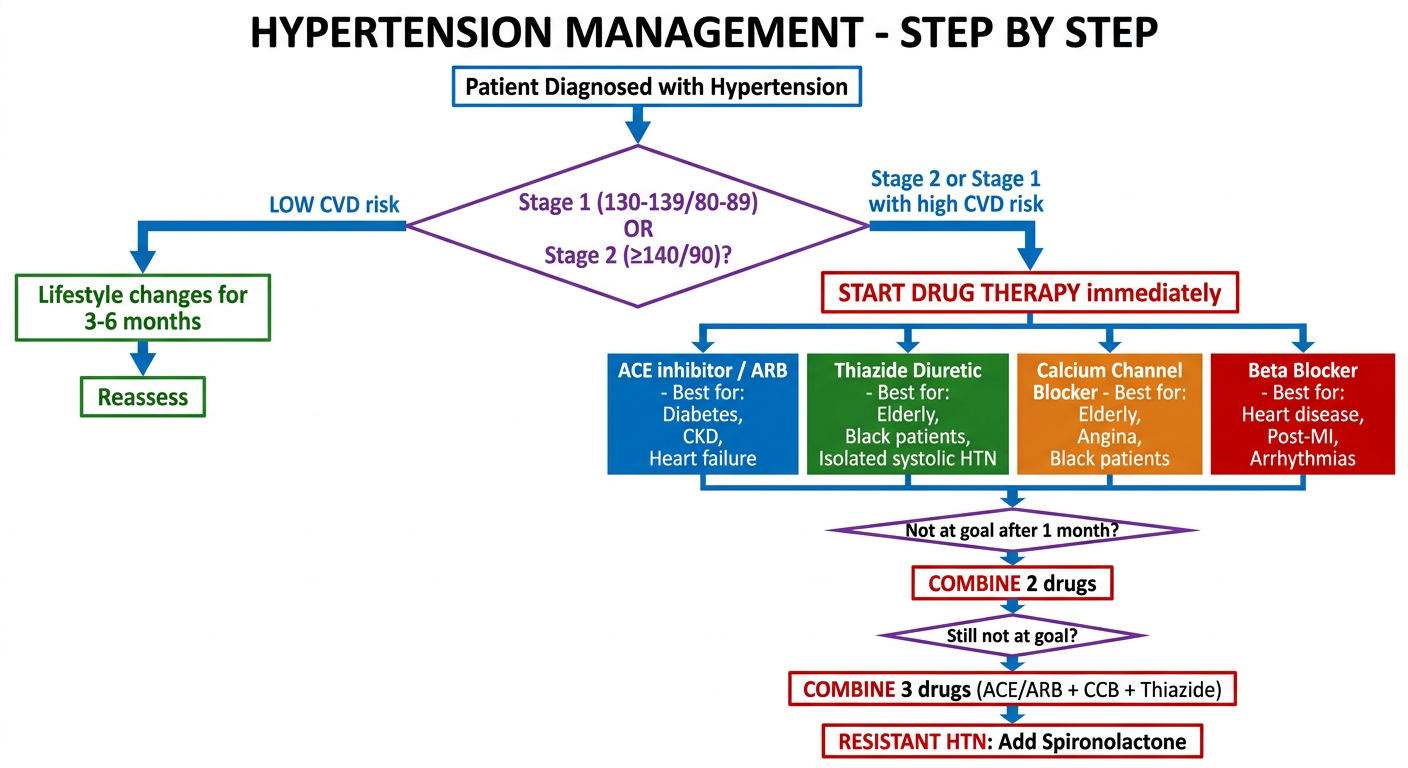
A clean medical treatment flowchart titled "HYPERTENSION MANAGEMENT - STEP BY STEP" showing a decision tree. Start box: "Patient Diagnosed with Hypertension". Arrow to diamond shape: "Stage 1 (130-139/80-89) OR Stage 2 (≥140/90)?". Left branch from Stage 1: "LOW CVD risk → Lifestyle changes for 3-6 months → Reassess". Right branch from Stage 2 or Stage 1 with high CVD risk: "START DRUG THERAPY immediately". Below drug therapy box: 4 colored boxes side by side: Blue "ACE inhibitor / ARB - Best for: Diabetes, CKD, Heart failure", Green "Thiazide Diuretic - Best for: Elderly, Black patients, Isolated systolic HTN", Orange "Calcium Channel Blocker - Best for: Elderly, Angina, Black patients", Red "Beta Blocker - Best for: Heart disease, Post-MI, Arrhythmias". Arrow down from all four: "Not at goal after 1 month?" → "COMBINE 2 drugs" → "Still not at goal?" → "COMBINE 3 drugs (ACE/ARB + CCB + Thiazide)" → "RESISTANT HTN: Add Spironolactone". White background, colorful, bold text, clean lines, medical student friendly.
🩺 HYPERTENSION - Easy Study Notes
📌 FLOWCHART 1 - Overview
📌 FLOWCHART 2 - How HTN Damages the Body
📌 FLOWCHART 3 - Treatment Step-by-Step
1️⃣ WHAT IS IT?
- BP = the force of blood pushing against artery walls
- Normal: <120/80 mmHg
- Hypertension = BP stays ≥130/80 mmHg persistently
2️⃣ CLASSIFICATION (Easy Table)
| Stage | Systolic | Diastolic | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Elevated | 120-129 | and | <80 |
| Stage 1 HTN | 130-139 | or | 80-89 |
| Stage 2 HTN | ≥140 | or | ≥90 |
| Crisis / Emergency | ≥180 | or | ≥120 |
3️⃣ TYPES (Simple)
- No single cause found
- Caused by: genetics + bad lifestyle
- Risk factors:
- ☑ Obesity
- ☑ High salt diet
- ☑ Physical inactivity
- ☑ Stress
- ☑ Heavy alcohol
- ☑ Family history
- Has a specific cause - find it and treat it!
| Cause | Clue to Spot It |
|---|---|
| Renal artery stenosis | Abdominal bruit, young woman |
| Primary aldosteronism | Low potassium + high BP |
| Pheochromocytoma | Episodic sweating, headache, palpitations |
| Cushing syndrome | Moon face, buffalo hump, striae |
| Sleep apnea | Snoring, obese, BP high in morning |
| Hypothyroidism | Fatigue, cold intolerance |
4️⃣ HOW IT HAPPENS (Pathophysiology - 3 Pathways)
OBESITY / GENETICS
↓
┌─────────────────────────────────────┐
│ 1. RAAS Activated │ → Aldosterone → Salt retention
│ 2. Sympathetic Nerves Overactive │ → Heart rate ↑, vessels squeeze
│ 3. Kidney can't excrete sodium │ → Fluid builds up
└─────────────────────────────────────┘
↓
↑ Cardiac Output + ↑ Resistance
↓
HIGH BLOOD PRESSURE
5️⃣ SYMPTOMS (Easy to Remember)
- Usually NONE - called the "Silent Killer" 🤫
- Sometimes: headache (back of head), dizziness, nosebleeds
- With severe HTN: blurred vision, chest pain, shortness of breath
6️⃣ TARGET ORGAN DAMAGE (What gets hurt over time)
| Organ | What Happens |
|---|---|
| 🧠 Brain | Stroke, memory loss |
| ❤️ Heart | LVH (enlarged heart), heart attack, heart failure |
| 🫘 Kidney | CKD → kidney failure |
| 👁️ Eyes | Blurred vision, blindness (retinopathy) |
| 🩸 Aorta | Aortic dissection, aneurysm |
7️⃣ DIAGNOSIS
- Measure BP correctly (3 separate readings, both arms, at rest)
- Confirm with home/ambulatory monitor (rules out white-coat hypertension)
- Basic workup:
- Blood: creatinine, electrolytes, glucose, lipids
- Urine: urinalysis for protein
- ECG: look for LVH
- If secondary suspected: aldosterone/renin ratio, renal ultrasound, urine catecholamines
8️⃣ TREATMENT
Step 1 - Lifestyle (for EVERYONE)
| Change | How Much It Lowers BP |
|---|---|
| Lose 10 kg weight | ↓ 5-20 mmHg |
| DASH diet (fruits, veggies, low fat) | ↓ 8-14 mmHg |
| Cut salt to <2.4 g/day | ↓ 2-8 mmHg |
| Exercise 30 min/day | ↓ 4-9 mmHg |
| Limit alcohol | ↓ 2-4 mmHg |
Step 2 - Drugs (4 Pillars)
| Drug Class | Mechanism | Best For |
|---|---|---|
| ACE inhibitor / ARB | Block RAAS | Diabetes, CKD, Heart failure |
| Thiazide diuretic | Remove salt/water | Elderly, black patients |
| Calcium Channel Blocker | Relax blood vessels | Elderly, angina, stroke |
| Beta-blocker | Slow heart, lower output | Post-MI, arrhythmia, angina |
- 1 drug → not controlled → add 2nd drug → not controlled → add 3rd drug
- Best triple combo: ACE/ARB + CCB + Thiazide
- Resistant HTN (on 3 drugs, still not controlled): add Spironolactone
9️⃣ HYPERTENSIVE EMERGENCY (Must Know!)
- BP ≥180/120 + end-organ damage
- Signs: severe headache, confusion, chest pain, blurry vision, no urine
- Treatment: IV drugs in ICU - Labetalol, Nicardipine, Sodium nitroprusside
- Rule: Lower BP by max 25% in first hour only - dropping too fast causes stroke!
🔑 MEMORY TRICKS
- "ABCD" drugs - ACE inhibitor, Beta-blocker, CCB (Calcium channel blocker), Diuretic
- Silent Killer = no symptoms until organ is damaged
- 3 Pathways = RAAS + Sympathetic + Kidney sodium
- Pheochromocytoma clue = "Spells" of headache + sweating + palpitations
Clinical features and investigations
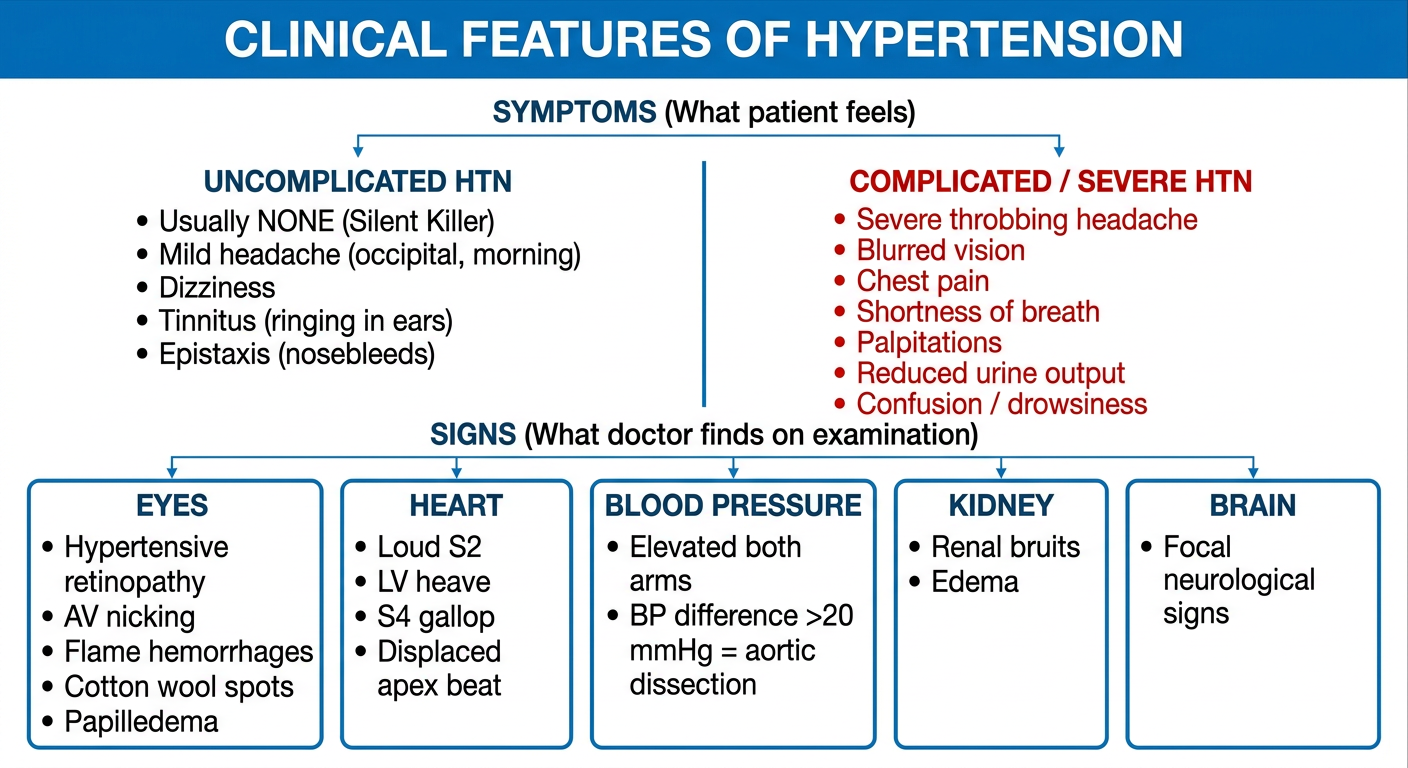
A clean medical education flowchart titled "CLINICAL FEATURES OF HYPERTENSION" divided into clear sections. Top section labeled "SYMPTOMS (What patient feels)" with two columns: Left column "UNCOMPLICATED HTN" with bullet points: "Usually NONE (Silent Killer)", "Mild headache (occipital, morning)", "Dizziness", "Tinnitus (ringing in ears)", "Epistaxis (nosebleeds)". Right column "COMPLICATED / SEVERE HTN" with bullet points: "Severe throbbing headache", "Blurred vision", "Chest pain", "Shortness of breath", "Palpitations", "Reduced urine output", "Confusion / drowsiness". Below that a section "SIGNS (What doctor finds on examination)" with 5 boxes in a row: Box 1 "EYES: Hypertensive retinopathy - AV nicking, flame hemorrhages, cotton wool spots, papilledema"; Box 2 "HEART: Loud S2, LV heave, S4 gallop, displaced apex beat"; Box 3 "BLOOD PRESSURE: Elevated both arms, BP difference >20 mmHg = aortic dissection"; Box 4 "KIDNEY: Renal bruits, edema"; Box 5 "BRAIN: Focal neurological signs". White background, blue header, red for emergency features, clear readable text, medical student style.
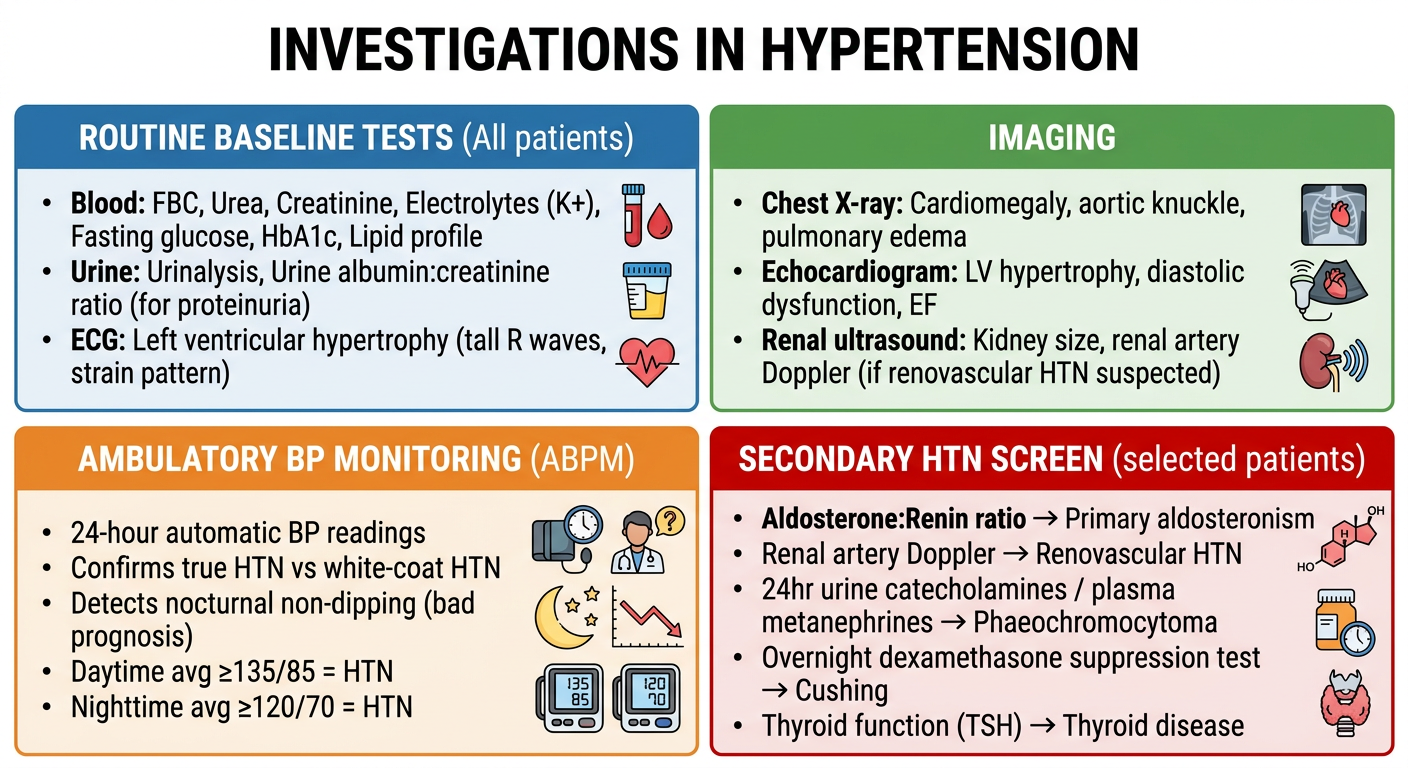
A clean medical education infographic titled "INVESTIGATIONS IN HYPERTENSION" showing a structured layout with 4 main categories arranged in a 2x2 grid. Category 1 (top-left, blue) "ROUTINE BASELINE TESTS (All patients)": bullet points: "Blood: FBC, Urea, Creatinine, Electrolytes (K+), Fasting glucose, HbA1c, Lipid profile"; "Urine: Urinalysis, Urine albumin:creatinine ratio (for proteinuria)"; "ECG: Left ventricular hypertrophy (tall R waves, strain pattern)". Category 2 (top-right, green) "IMAGING": bullet points: "Chest X-ray: Cardiomegaly, aortic knuckle, pulmonary edema"; "Echocardiogram: LV hypertrophy, diastolic dysfunction, EF"; "Renal ultrasound: Kidney size, renal artery Doppler (if renovascular HTN suspected)". Category 3 (bottom-left, orange) "AMBULATORY BP MONITORING (ABPM)": "24-hour automatic BP readings"; "Confirms true HTN vs white-coat HTN"; "Detects nocturnal non-dipping (bad prognosis)"; "Daytime avg ≥135/85 = HTN"; "Nighttime avg ≥120/70 = HTN". Category 4 (bottom-right, red) "SECONDARY HTN SCREEN (selected patients)": "Aldosterone:Renin ratio → Primary aldosteronism"; "Renal artery Doppler → Renovascular HTN"; "24hr urine catecholamines / plasma metanephrines → Phaeochromocytoma"; "Overnight dexamethasone suppression test → Cushing"; "Thyroid function (TSH) → Thyroid disease". White background, color coded, bold headings, clean layout, medical student friendly.
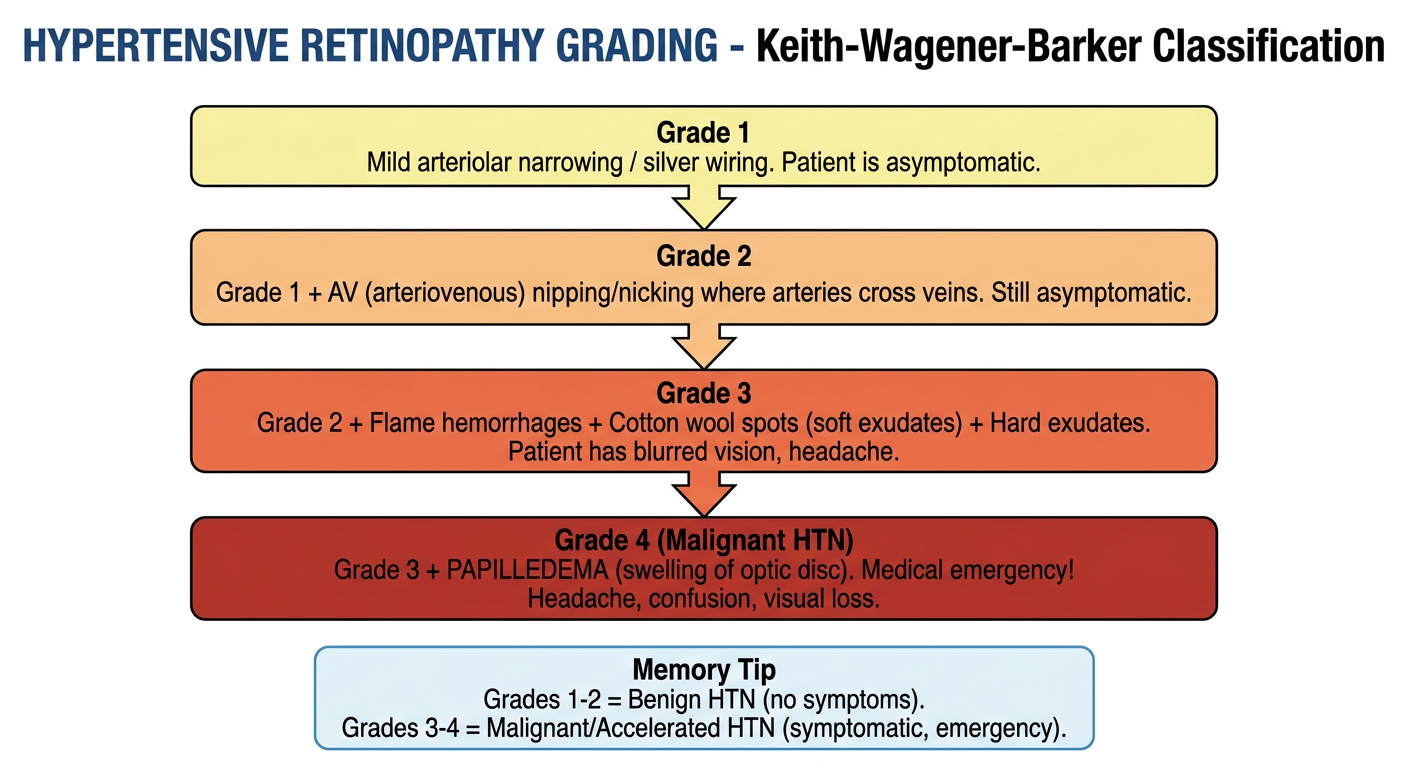
A clean medical education flowchart titled "HYPERTENSIVE RETINOPATHY GRADING - Keith-Wagener-Barker Classification" with 4 grade boxes arranged vertically with arrows between them. Grade 1 box (light yellow): "Grade 1: Mild arteriolar narrowing / silver wiring. Patient is asymptomatic." Grade 2 box (light orange): "Grade 2: Grade 1 + AV (arteriovenous) nipping/nicking where arteries cross veins. Still asymptomatic." Grade 3 box (orange-red): "Grade 3: Grade 2 + Flame hemorrhages + Cotton wool spots (soft exudates) + Hard exudates. Patient has blurred vision, headache." Grade 4 box (dark red): "Grade 4 (Malignant HTN): Grade 3 + PAPILLEDEMA (swelling of optic disc). Medical emergency! Headache, confusion, visual loss." Memory tip box at bottom: "Grades 1-2 = Benign HTN (no symptoms). Grades 3-4 = Malignant/Accelerated HTN (symptomatic, emergency)." White background, color-coded severity from yellow to dark red, clear bold text, medical student friendly.
🩺 CLINICAL FEATURES & INVESTIGATIONS OF HYPERTENSION
📌 FLOWCHART 1 - Clinical Features at a Glance
📌 FLOWCHART 2 - Investigations Summary
📌 FLOWCHART 3 - Hypertensive Retinopathy Grades (Very Exam-Important!)
PART A: CLINICAL FEATURES
1️⃣ SYMPTOMS
Key Rule: Hypertension is the "Silent Killer" - Most patients have NO symptoms!
🔵 Uncomplicated Hypertension (No organ damage yet)
- Usually completely asymptomatic
- Mild symptoms (non-specific, often ignored):
- Morning headache (occipital - back of head)
- Dizziness / lightheadedness
- Tinnitus (ringing in ears)
- Epistaxis (nosebleeds) - rare
- Fatigue, poor exercise tolerance
🔴 Complicated / Severe Hypertension (Organ damage present)
| Organ Affected | Symptoms |
|---|---|
| 🧠 Brain | Severe headache, confusion, visual disturbances, seizures (encephalopathy) |
| ❤️ Heart | Chest pain, palpitations, shortness of breath, orthopnea |
| 🫘 Kidney | Oliguria (reduced urine), frothy urine (proteinuria), ankle swelling |
| 👁️ Eyes | Blurred vision, sudden visual loss |
| 🩸 Aorta | Sudden tearing chest/back pain (dissection) |
2️⃣ SIGNS (What you find on examination)
🔵 General
- Elevated BP on both arms (measure both!)
- BP difference >20 mmHg between arms → suspect aortic dissection
- Obesity (BMI >30)
- Cushingoid features (if secondary)
👁️ Eyes - MOST IMPORTANT CLINICAL SIGN
| Grade | What you see | Clinical status |
|---|---|---|
| Grade 1 | Arteriolar narrowing, "silver wiring" | Asymptomatic |
| Grade 2 | Grade 1 + AV nicking/nipping | Asymptomatic |
| Grade 3 | Grade 2 + Flame hemorrhages + Cotton wool spots + Hard exudates | Symptomatic |
| Grade 4 | Grade 3 + Papilledema | Malignant HTN - Emergency! |
💡 Memory trick: Grades 1-2 = Benign HTN | Grades 3-4 = Malignant/Accelerated HTN
❤️ Heart (Cardiovascular)
- Apex beat - displaced laterally (LV enlargement)
- Heaving apex - pressure overload
- Loud S2 at aortic area (aortic valve closes forcefully)
- S4 gallop - stiff, hypertrophied left ventricle
- Later: signs of heart failure (S3, crepitations, JVP raised)
🫘 Kidney / Abdomen
- Renal bruit (bruit over kidney area) → renovascular hypertension
- Abdominal bruit → renal artery stenosis
- Palpable kidneys → polycystic kidney disease
🧠 Neurological
- Focal neurological deficits → stroke
- Confusion, altered GCS → hypertensive encephalopathy
- Papilledema → raised intracranial pressure
🔍 Clues for Secondary Hypertension
| Finding | Think of |
|---|---|
| Central obesity, striae, moon face | Cushing syndrome |
| Hypokalemia + HTN | Primary aldosteronism (Conn) |
| Episodic sweating, pallor, palpitations | Phaeochromocytoma |
| Abdominal bruit | Renal artery stenosis |
| Delayed femoral pulse | Coarctation of aorta |
| Bradycardia, dry skin | Hypothyroidism |
PART B: INVESTIGATIONS
3️⃣ ROUTINE BASELINE (Do in EVERY patient)
🩸 Blood Tests
| Test | What you're looking for |
|---|---|
| Urea + Creatinine + eGFR | Renal damage (nephrosclerosis) |
| Electrolytes (K+, Na+) | Low K+ → aldosteronism; raised K+ → renal failure |
| Fasting glucose + HbA1c | Diabetes (major co-risk factor) |
| Lipid profile | Dyslipidaemia (CVD risk assessment) |
| Full blood count | Anaemia, polycythaemia |
| Thyroid function (TSH) | Hypothyroidism / hyperthyroidism |
🚽 Urine Tests
| Test | What you're looking for |
|---|---|
| Urinalysis (dipstick) | Proteinuria, haematuria, glucose |
| Urine albumin:creatinine ratio (ACR) | Early kidney damage (microalbuminuria) |
| Urine microscopy | Red cell casts → glomerulonephritis |
📋 ECG (Electrocardiogram)
- Look for Left Ventricular Hypertrophy (LVH):
- Tall R waves in V5, V6
- Deep S waves in V1, V2
- ST depression + T wave inversion ("strain pattern")
- Sokolow-Lyon index: S(V1) + R(V5 or V6) > 35 mm
- Also: AF, ischaemia
4️⃣ IMAGING
| Investigation | What it shows |
|---|---|
| Chest X-ray | Cardiomegaly, aortic knuckle, pulmonary oedema, rib notching (coarctation) |
| Echocardiogram | LV wall thickness, diastolic dysfunction, EF, valve disease |
| Renal Ultrasound | Kidney size (small = CKD), cysts (PCKD), hydronephrosis |
| Renal Artery Doppler | Renal artery stenosis |
| CT Aorta | Aortic dissection / aneurysm (if suspected) |
| MRI Brain | Stroke, posterior leukoencephalopathy (PRES) |
5️⃣ AMBULATORY BP MONITORING (ABPM)
Used to confirm diagnosis and rule out white-coat hypertension
| Setting | HTN Threshold |
|---|---|
| Office / clinic | ≥140/90 mmHg |
| Home BP monitoring | ≥135/85 mmHg |
| ABPM - Daytime average | ≥135/85 mmHg |
| ABPM - Night-time average | ≥120/70 mmHg |
| ABPM - 24-hour average | ≥130/80 mmHg |
- Diagnoses white-coat hypertension (high in clinic, normal at home - no treatment needed)
- Diagnoses masked hypertension (normal in clinic, high at home - dangerous, needs treatment)
- Detects nocturnal non-dipping (BP doesn't fall at night = worse prognosis, more organ damage)
6️⃣ SECONDARY HYPERTENSION SCREEN (Only if suspected)
| Suspected cause | Test to order |
|---|---|
| Primary aldosteronism (Conn) | Plasma aldosterone : renin ratio (ARR) |
| Renovascular HTN | Renal artery Doppler; CT/MR angiography |
| Phaeochromocytoma | 24-hr urine catecholamines & metanephrines; Plasma fractionated metanephrines |
| Cushing syndrome | Overnight dexamethasone suppression test; 24-hr urinary cortisol |
| Coarctation of aorta | CT aorta; delayed femoral pulse; rib notching on CXR |
| Sleep apnea | Overnight polysomnography (sleep study) |
| Renal parenchymal disease | Creatinine, GFR, urine ACR, renal biopsy |
- Age <30 with HTN
- Resistant HTN (on 3 drugs, still uncontrolled)
- Sudden onset or rapidly worsening HTN
- Spontaneous hypokalaemia
- Diastolic HTN in elderly
🔑 QUICK MEMORY SUMMARY
SYMPTOMS: Usually NONE → Silent Killer
Headache + blurred vision + chest pain = EMERGENCY
SIGNS: Eyes first! (Earliest sign = hypertensive retinopathy)
Grade 1-2 = Benign | Grade 3-4 = Malignant
ROUTINE: Blood (Creatinine, K+, glucose, lipids)
Urine (protein, ACR)
ECG (LVH)
CXR (cardiomegaly)
CONFIRM: ABPM - confirms true HTN vs white-coat
SECONDARY: ARR → Conn's
Doppler → Renal artery stenosis
Metanephrines → Phaeochromocytoma
Dexamethasone test → Cushing