cardiac cycle essay physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Searching Images
Wiggers diagram cardiac cycle pressure volume ECG heart sounds
I now have comprehensive material. Let me write the essay:
The Cardiac Cycle: A Comprehensive Physiological Essay
Introduction
The cardiac cycle encompasses all mechanical and electrical events that occur from the beginning of one heartbeat to the beginning of the next. At a resting heart rate of 72 beats/min, one complete cycle lasts approximately 0.833 seconds. The cycle is orchestrated by the coordinated interplay of the electrical conduction system, myocardial contractile properties, and valve mechanics. Each cycle is initiated by spontaneous depolarization in the sinoatrial (SA) node — located in the superior lateral wall of the right atrium — from which the action potential propagates through both atria, then is briefly delayed (>0.1 s) at the atrioventricular (AV) node before traversing the His-Purkinje system into the ventricles. This delay is physiologically critical: it allows atrial contraction to complete — priming the ventricles — before ventricular systole begins.
The cycle is classically divided into seven phases, best understood by studying a simultaneous plot of left ventricular (LV) pressure, aortic pressure, left atrial (LA) pressure, LV volume, ECG, and heart sounds — the Wiggers diagram.
Phase 1 — Atrial Systole
ECG correlate: P wave
Atrial systole is atrial contraction. The P wave on the ECG marks atrial depolarization. Contraction of the left atrium raises LA pressure, actively ejecting blood through the already-open mitral valve into the left ventricle. This constitutes the final ~20–30% of ventricular filling (the remainder being passive). The rise in atrial pressure is reflected back into the pulmonary veins and appears on the venous pulse record as the a wave.
The left ventricle is still relaxed at this point; its volume increases slightly to reach the end-diastolic volume (EDV) of approximately 120–140 mL. The fourth heart sound (S4) is associated with atrial systole; it is inaudible in healthy adults but becomes audible when ventricular compliance is reduced (e.g., left ventricular hypertrophy).
Phase 2 — Isovolumetric Ventricular Contraction
ECG correlate: QRS complex | Heart sound: S1
Ventricular depolarization (QRS complex) triggers ventricular contraction. As ventricular pressure rises and exceeds left atrial pressure, the mitral valve closes — producing the first heart sound (S1). The aortic valve has not yet opened because LV pressure has not yet reached aortic diastolic pressure (~80 mmHg). With all four valves closed, no blood can exit or enter the ventricle, so ventricular volume remains constant (isovolumetric) while pressure rises steeply and rapidly. Although shape changes do occur — including the initiation of the twisting/torsional motion — the volume is truly constant during this phase.
This is the phase of maximum rate of pressure rise, expressed as dP/dt max, a useful index of myocardial contractility. The duration of isovolumetric contraction is ~50–70 ms.
Phase 3 — Rapid Ventricular Ejection
ECG correlate: ST segment
When LV pressure exceeds aortic pressure (~80 mmHg), the aortic valve opens. Blood is ejected rapidly into the aorta, driven by the pressure gradient. During the first half of systole, LV pressure slightly exceeds aortic pressure, causing rapid flow acceleration. Aortic pressure rises to its peak (systolic pressure, ~120 mmHg). LV volume falls dramatically as stroke volume is expelled. The ventricle continues its counterclockwise apical rotation (wringing motion), aiding ejection efficiency.
Phase 4 — Reduced Ventricular Ejection (Protodiastole)
ECG correlate: T wave
The rate of ejection slows as ventricular repolarization begins (T wave). In the second half of systole, aortic pressure exceeds LV pressure, yet forward flow continues (deceleration phase) due to momentum of the ejected blood column. LV volume continues to decrease, reaching the end-systolic volume (ESV) of approximately 50–70 mL.
Stroke volume (SV) = EDV − ESV = ~70 mL
Ejection fraction (EF) = SV/EDV = ~55–70% (normal ≥55%)
Ejection fraction (EF) = SV/EDV = ~55–70% (normal ≥55%)
Phase 5 — Isovolumetric Ventricular Relaxation
ECG correlate: isoelectric (post-T wave) | Heart sound: S2
Systole ends and the ventricle relaxes. LV pressure falls below aortic pressure, causing aortic valve closure — marked by the dicrotic notch on the aortic pressure tracing and producing the second heart sound (S2, split into aortic component A2 and pulmonic component P2). All valves are again closed; ventricular volume stays at ESV while pressure falls rapidly. The mitral valve has not yet re-opened. This phase lasts ~50–80 ms and is an active, energy-requiring process (calcium re-uptake into the SR via SERCA2a), not merely passive recoil.
Phase 6 — Rapid Ventricular Filling
ECG correlate: after T wave | Heart sound: S3 (if present)
When LV pressure falls below LA pressure, the mitral valve opens. Blood flows passively from the left atrium — which has been filling from the pulmonary veins throughout systole — into the relaxing ventricle. This is the most rapid filling phase; ventricular volume rises quickly while pressure remains low and relatively constant because the relaxed, compliant ventricle accommodates volume with little pressure rise. The third heart sound (S3) is generated at the end of rapid filling, when ventricular filling suddenly decelerates. S3 is normal in children and young adults; in adults >40 years it suggests ventricular volume overload or reduced compliance (e.g., heart failure).
The "suction" effect of ventricular relaxation — the release of stored elastic energy from the twisted systolic configuration (recoil) — actively draws blood into the ventricle.
Phase 7 — Reduced Ventricular Filling (Diastasis)
ECG correlate: TP segment
Filling slows as the pressure gradient between atrium and ventricle equalizes. This phase is abbreviated or nearly absent at high heart rates (when the cardiac cycle shortens, diastole is disproportionately curtailed). The cycle then restarts with the next P wave and atrial systole.
Summary Table of the Seven Phases
| Phase | Valve Events | Volume | ECG | Heart Sound |
|---|---|---|---|---|
| A — Atrial Systole | Mitral open, Aortic closed | EDV reached | P wave | S4 (abnormal) |
| B — Isovolumetric Contraction | Mitral closes | Constant | QRS | S1 |
| C — Rapid Ejection | Aortic opens | ↓↓ | ST segment | — |
| D — Reduced Ejection | Aortic open | ↓ (to ESV) | T wave | — |
| E — Isovolumetric Relaxation | Aortic closes | Constant (ESV) | Post-T | S2 |
| F — Rapid Filling | Mitral opens | ↑↑ | — | S3 (can be normal) |
| G — Diastasis | Mitral open | ↑ (slow) | TP interval | — |
The Pressure-Volume Loop
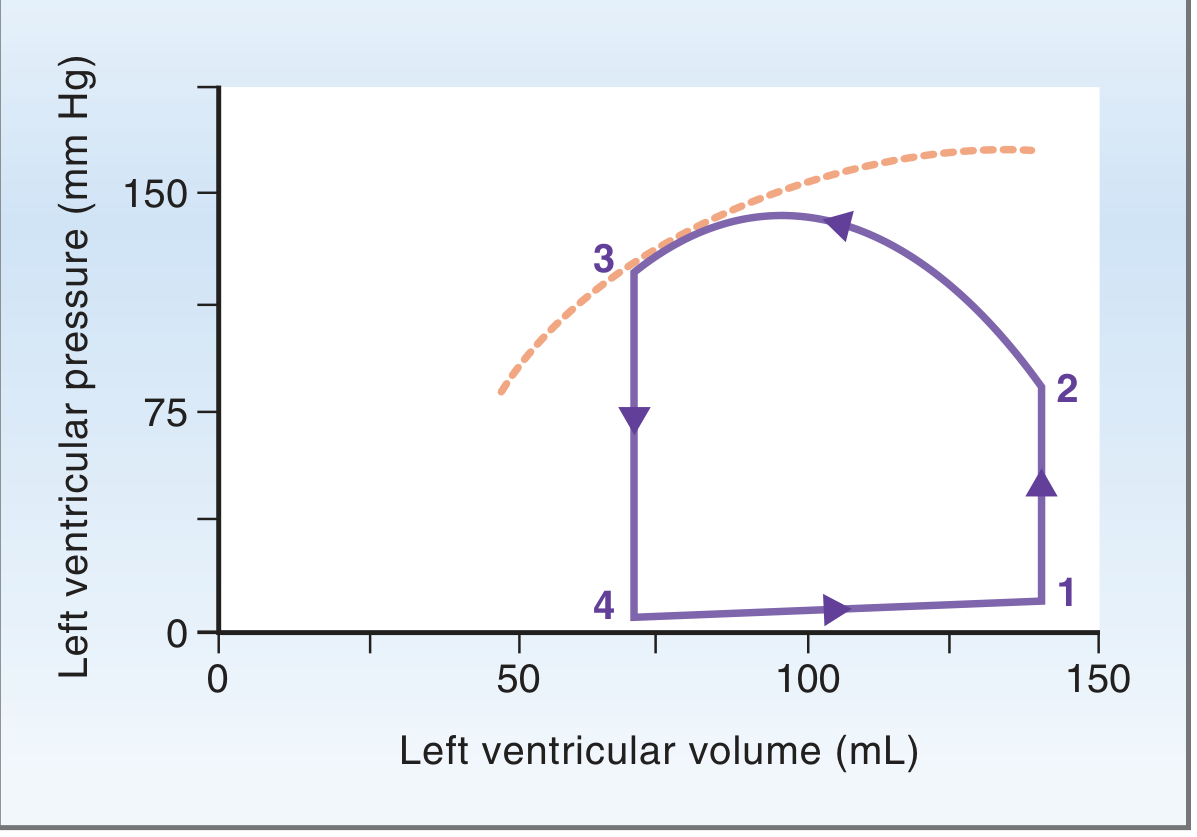
The pressure-volume (PV) loop elegantly summarises a single cardiac cycle. Four corners define four critical events:
- Point 1 (bottom-right): End of diastole — mitral valve closes. Volume = EDV (~140 mL), pressure low.
- Point 2 (top-right): End of isovolumetric contraction — aortic valve opens. Pressure = diastolic aortic pressure (~80 mmHg).
- Point 3 (top-left): End of ejection — aortic valve closes. Volume = ESV (~70 mL), pressure = peak systolic (~120 mmHg).
- Point 4 (bottom-left): End of isovolumetric relaxation — mitral valve opens. Volume = ESV, pressure = ~5–8 mmHg.
The width of the loop = SV. The area within the loop = stroke work (external work performed by the ventricle per beat).
Effects of preload, afterload, and contractility on the PV loop:
- Increased preload (↑EDV, e.g., increased venous return): Loop shifts rightward; stroke volume increases per the Frank-Starling law (greater end-diastolic fibre length → greater force of contraction → larger SV).
- Increased afterload (↑aortic pressure, e.g., hypertension): Loop shifts upward; isovolumetric contraction phase is prolonged; SV decreases and ESV increases.
- Increased contractility (e.g., sympathetic stimulation, catecholamines): Loop shifts left; ESV decreases; SV and EF increase. This is reflected as an upward shift of the end-systolic pressure-volume relationship (ESPVR).
Cardiac Muscle Mechanics
Cardiac muscle is a functional syncytium: individual cardiomyocytes are connected via intercalated discs containing gap junctions (connexin-43), enabling rapid electrical propagation throughout the myocardium as if it were a single cell. This all-or-none behaviour ensures coordinated contraction.
The action potential in ventricular myocytes is characterised by a prolonged plateau (Phase 2), driven by L-type Ca²⁺ channel influx. This triggers calcium-induced calcium release (CICR) from the sarcoplasmic reticulum via ryanodine receptors (RyR2), producing the calcium transient necessary for actin-myosin cross-bridge cycling. Relaxation requires active re-sequestration of Ca²⁺ by SERCA2a (phospholamban-regulated) and extrusion via the Na⁺/Ca²⁺ exchanger — explaining why isovolumetric relaxation is an active, ATP-consuming process.
The left ventricle contracts in a helical, wringing motion: subepicardial fibres rotate the apex counterclockwise while subendocardial fibres rotate the base. This torsion maximises ejection efficiency and stores elastic energy that fuels early diastolic suction.
Right vs. Left Heart Timing
The right heart undergoes essentially the same sequence but at lower pressures (RV systolic pressure ~25 mmHg; pulmonary artery diastolic ~10 mmHg). This means:
- The pulmonic valve opens later than the aortic valve (lower RV pressure threshold)
- The tricuspid valve closes slightly after the mitral valve
- At end-inspiration, increased venous return to the right heart slightly delays pulmonic valve closure relative to aortic closure, producing physiological splitting of S2 (A2 before P2, with the gap widening on inspiration).
Effect of Heart Rate on the Cardiac Cycle
When heart rate increases, both systole and diastole shorten, but diastole shortens disproportionately. At 72 bpm, systole is ~40% of the cycle. At ~200 bpm, systole may occupy ~65% of the cycle. This has two major implications:
- Coronary perfusion occurs predominantly in diastole; tachycardia reduces coronary perfusion time, particularly relevant in the presence of coronary artery disease.
- Ventricular filling is curtailed; if diastasis is entirely eliminated, atrial contribution becomes essential to maintain adequate EDV, explaining why loss of atrial kick (e.g., in atrial fibrillation) is especially detrimental in tachycardia.
Clinical Correlates
| Physiological Event | Clinical Relevance |
|---|---|
| Prolonged isovolumetric relaxation | Diastolic dysfunction (impaired SERCA2a, fibrosis) |
| Elevated ESV / low EF | Systolic heart failure |
| S3 in adults >40 yrs | Volume overload, dilated cardiomyopathy |
| S4 | Stiff ventricle, hypertensive heart disease, hypertrophic cardiomyopathy |
| Fixed split S2 | Atrial septal defect |
| Paradoxical split S2 | Left bundle branch block, aortic stenosis |
| Dicrotic notch loss | Aortic regurgitation |
Conclusion
The cardiac cycle is a precisely timed sequence of mechanical and electrical events, governed by pressure gradients and valve mechanics. Its seven phases — atrial systole, isovolumetric contraction, rapid ejection, reduced ejection, isovolumetric relaxation, rapid filling, and diastasis — repeat ~72 times per minute throughout life. The pressure-volume loop integrates these events into a geometric representation that enables quantification of stroke volume, stroke work, and the effects of preload, afterload, and contractility. Understanding the cardiac cycle in this mechanistic detail is foundational to interpreting heart sounds, interpreting haemodynamic data, and managing conditions from heart failure to valvular disease.
Sources:
- Guyton and Hall Textbook of Medical Physiology (p. 122, p. 131)
- Costanzo Physiology, 7th Edition (p. 156–160)
- Textbook of Clinical Echocardiography (p. 168)
This is a shared conversation. Sign in to Orris to start your own chat.