I am intern doctor, please show list of all dermatology and venereology illnesses along with clinical pictures , please show clinical pictures along with all illness and also mention their clinical classification, management, diagnosis, laboratory analysis and treatment
dermatology venereology complete list of skin diseases classification 2024
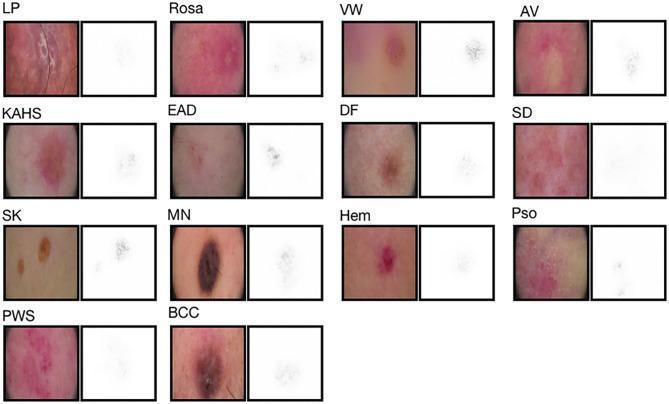
dermatology skin diseases clinical presentation rash
psoriasis eczema acne rosacea fungal infection clinical photo
syphilis gonorrhea STI herpes genitalis clinical photograph
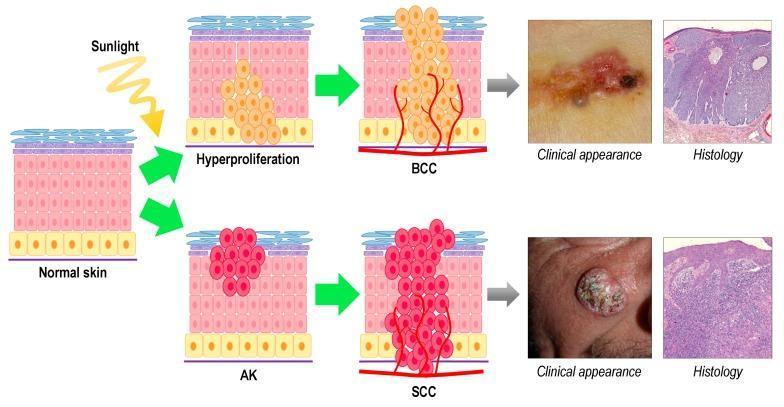
melanoma basal cell carcinoma squamous cell carcinoma skin cancer clinical
urticaria bullous pemphigoid pemphigus vulgaris blistering disorder
vitiligo alopecia areata lichen planus pigmentation disorder
tinea corporis ringworm scabies pediculosis dermatophyte infection
acne vulgaris rosacea perioral dermatitis sebaceous gland disorder
🩺 Complete Dermatology & Venereology Reference for Intern Doctors
CLASSIFICATION FRAMEWORK
- Inflammatory (infectious vs. non-infectious)
- Neoplastic (benign vs. malignant)
PART I — INFLAMMATORY NON-INFECTIOUS DERMATOSES
1. PSORIASIS

- Mild–Moderate (PASI <10): Topical corticosteroids (betamethasone), Vitamin D analogues (calcipotriol), tar preparations, retinoids, keratolytics
- Moderate–Severe (PASI ≥10): Narrow-band UVB phototherapy, PUVA; Methotrexate 7.5–25 mg/week; Ciclosporin 2.5–5 mg/kg/day; Acitretin
- Biologic Agents: Anti-TNF (adalimumab, infliximab), Anti-IL-12/23 (ustekinumab), Anti-IL-17 (secukinumab, ixekizumab), Anti-IL-23 (guselkumab, risankizumab)
- Nail psoriasis: Intralesional triamcinolone, topical tazarotene
2. ECZEMA / ATOPIC DERMATITIS

- Emollients liberally; avoid triggers; tepid baths
- Topical corticosteroids (mild for face: 1% hydrocortisone; moderate-potent for body: betamethasone)
- Topical calcineurin inhibitors (tacrolimus, pimecrolimus) — steroid-sparing on face/flexures
- Antihistamines for pruritus (cetirizine, loratadine)
- Moderate–Severe: Dupilumab (anti-IL-4/IL-13), cyclosporine, methotrexate, azathioprine
- Infected eczema: Flucloxacillin/cephalexin; intranasal mupirocin to decolonize Staph aureus
3. ACNE VULGARIS
- Non-inflammatory: Comedones (open blackheads, closed whiteheads)
- Inflammatory: Papules, pustules, nodules, cysts
- Grading: Mild (comedones ± few papules), Moderate (papulopustular), Severe (nodulocystic, scarring)

- Mild: Topical benzoyl peroxide (2.5–5%), topical retinoids (tretinoin 0.025–0.05%, adapalene), azelaic acid
- Moderate: Topical antibiotic (clindamycin) + benzoyl peroxide (to prevent resistance); or oral antibiotic (doxycycline 100 mg/day × 3 months)
- Severe/Nodulocystic: Oral isotretinoin 0.5–1 mg/kg/day × 16–24 weeks (requires monitoring of LFTs, lipids, pregnancy test)
- Hormonal (females): Combined OCP (especially cyproterone acetate + ethinylestradiol), spironolactone 50–100 mg/day
- Intralesional triamcinolone for cysts; chemical peels, laser for scars
4. ROSACEA
- Subtype 1: Erythematotelangiectatic (ETR) — flushing, redness, telangiectasia
- Subtype 2: Papulopustular (PPR) — resembles acne, no comedones
- Subtype 3: Phymatous — rhinophyma (bulbous nose)
- Subtype 4: Ocular rosacea — blepharitis, conjunctivitis
- Avoid triggers: sun, heat, alcohol, spicy food
- ETR: Topical brimonidine (vasoconstrictor), oxymetazoline; laser/IPL for telangiectasia
- PPR: Topical metronidazole 0.75–1%, azelaic acid 15%, ivermectin 1%; oral doxycycline 40 mg/day (low-dose anti-inflammatory)
- Phymatous: CO₂ laser or dermabrasion for rhinophyma
- Ocular: Lid hygiene, topical ciclosporin eye drops
5. URTICARIA & ANGIOEDEMA
- 1st line: Non-sedating antihistamines (cetirizine 10 mg, loratadine 10 mg, fexofenadine 180 mg) — can up-dose ×4
- 2nd line: Add montelukast or H2-blocker (ranitidine/famotidine)
- Severe/refractory: Omalizumab 300 mg SC monthly (anti-IgE)
- Acute severe/anaphylaxis: IM adrenaline 0.3–0.5 mg
- Hereditary angioedema: C1-inhibitor concentrate, icatibant, lanadelumab (prophylaxis)
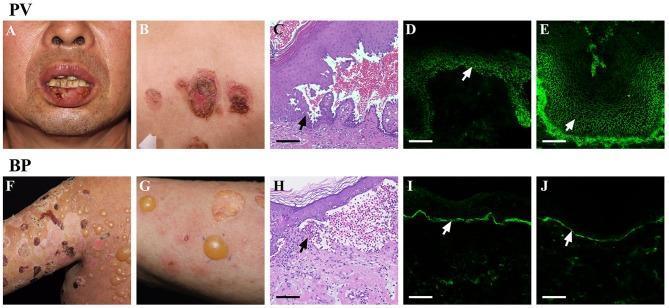
6. PEMPHIGUS VULGARIS

- Oral prednisolone 1 mg/kg/day (mainstay)
- Steroid-sparing: Azathioprine 1–3 mg/kg/day, mycophenolate mofetil 2–3 g/day
- Rituximab (anti-CD20) 1000 mg IV × 2 doses 2 weeks apart — increasingly 1st-line
- IVIG for refractory/life-threatening
- Wound care for erosions; antiseptic mouthwash for oral lesions
7. BULLOUS PEMPHIGOID
- Superpotent topical corticosteroids (clobetasol propionate 0.05%) — for localized disease
- Oral prednisolone 0.5 mg/kg/day
- Doxycycline 200 mg/day + nicotinamide (milder BP, fewer steroid side effects)
- Steroid-sparing: Azathioprine, MMF, methotrexate
- Omalizumab, dupilumab for refractory cases
8. LICHEN PLANUS

- Topical corticosteroids (first-line); intralesional triamcinolone for hypertrophic LP
- Oral prednisolone for widespread or erosive LP 0.5 mg/kg/day
- Topical tacrolimus (oral/genital LP)
- Hydroxychloroquine, acitretin, cyclosporin for resistant disease
- PUVA/NB-UVB for widespread cutaneous LP
9. VITILIGO

- Topical corticosteroids or tacrolimus (small areas)
- NB-UVB phototherapy (most effective for active vitiligo) — 2–3 sessions/week
- Excimer laser (308 nm) for localized lesions
- Ruxolitinib 1.5% cream (JAK1/2 inhibitor) — FDA-approved 2022 for non-segmental vitiligo in ≥12 yrs
- Oral tranexamic acid, oral mini-pulse corticosteroids to halt progression
- Surgical: suction blister grafting, split-thickness skin graft for stable segmental vitiligo
- Camouflage cosmetics
10. ALOPECIA AREATA
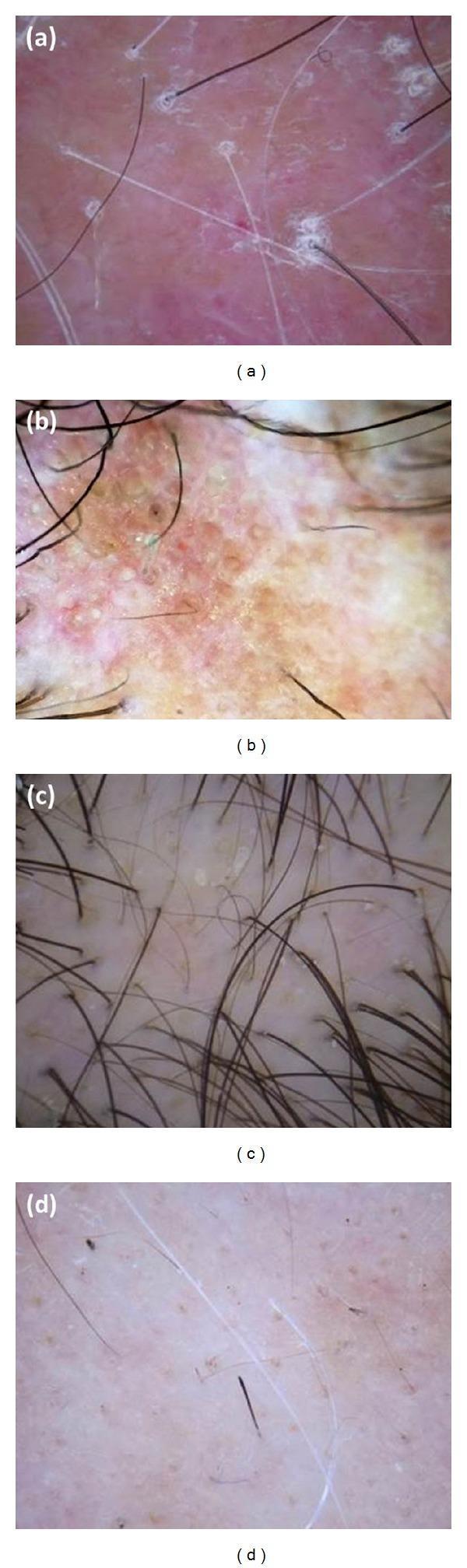
- Limited (<50%): Intralesional triamcinolone 5–10 mg/mL every 4–6 weeks
- Topical minoxidil 5% (adjunct)
- Topical sensitizers: DPCP or DNCB for extensive disease
- Extensive: Oral prednisolone pulse (methylprednisolone 250 mg/day × 3 days monthly)
- JAK inhibitors: Baricitinib 2–4 mg/day and ritlecitinib 50 mg/day (FDA-approved 2022/2023) — highly effective for severe AA
- NB-UVB for extensive cases
PART II — INFECTIONS OF THE SKIN
11. BACTERIAL — IMPETIGO
12. BACTERIAL — CELLULITIS & ERYSIPELAS
- Mild: Oral flucloxacillin 500 mg QDS × 5–7 days
- Severe/hospital: IV benzylpenicillin + flucloxacillin; or co-amoxiclav
- MRSA: IV vancomycin; PO linezolid
- Elevate limb; treat portal of entry (tinea pedis, fissures)
13. FUNGAL — DERMATOPHYTOSES (Tinea)


- Topical (limited): Clotrimazole 1%, miconazole 2%, terbinafine 1%, econazole — apply BID × 2–4 weeks
- Oral (extensive/nail/scalp): Terbinafine 250 mg/day × 6 wks (fingernails) or 12 wks (toenails); Itraconazole 200 mg/day or pulse dosing; Griseofulvin (T. capitis, especially children)
- Tinea versicolor: Selenium sulfide 2.5% shampoo, ketoconazole 2% shampoo; oral itraconazole 200 mg/day × 5–7 days
14. VIRAL — HERPES SIMPLEX (HSV)

- Oral aciclovir 200 mg 5×/day × 5 days (primary), or 400 mg TID × 5 days
- Valaciclovir 500 mg BD × 5 days (better bioavailability)
- Famciclovir 250 mg TID × 5 days
- Suppressive therapy (frequent recurrences): Valaciclovir 500 mg OD daily
- IV aciclovir 5–10 mg/kg TID for severe/systemic/neonatal/encephalitis
15. VIRAL — HERPES ZOSTER (Shingles)
- Oral valaciclovir 1000 mg TID × 7 days (start within 72h of rash)
- Famciclovir 500 mg TID × 7 days; aciclovir 800 mg 5×/day × 7 days
- IV aciclovir for disseminated/ophthalmic/immunocompromised
- PHN: Tricyclic antidepressants (amitriptyline), gabapentin, pregabalin, topical lidocaine 5% patch, capsaicin 8%
- Prevention: Recombinant zoster vaccine (Shingrix) — 2 doses; preferred over Zostavax
16. SCABIES
- Permethrin 5% cream — apply from neck down, leave 8 hours, repeat after 1 week
- Ivermectin 200 mcg/kg orally × 2 doses 2 weeks apart (crusted scabies, treatment failures)
- Malathion 0.5% lotion (alternative)
- Decontaminate clothing/bedding (hot wash 60°C); treat all household contacts simultaneously
- Antihistamines for pruritus (persists weeks post-treatment)
PART III — SKIN CANCERS (NEOPLASTIC)
17. MELANOMA

- Wide local excision (WLE): margins depend on Breslow depth (1 mm: 1 cm margin; >2 mm: 2–3 cm margin)
- Sentinel lymph node biopsy ± complete lymph node dissection
- Advanced/metastatic: BRAF/MEK inhibitors (vemurafenib + cobimetinib; dabrafenib + trametinib); Immunotherapy: anti-PD-1 (pembrolizumab, nivolumab), anti-CTLA-4 (ipilimumab); combined immunotherapy
- Adjuvant: Pembrolizumab or nivolumab post-surgery for stage III/IV
18. BASAL CELL CARCINOMA (BCC)

- Low-risk: Surgical excision (4–5 mm margins), curettage & cautery
- High-risk/facial: Mohs micrographic surgery (histologically controlled, tissue-sparing)
- Imiquimod 5% cream (superficial BCC); 5-fluorouracil cream
- Photodynamic therapy (PDT) — superficial
- Advanced/unresectable: Vismodegib (Hedgehog pathway inhibitor) 150 mg/day; Sonidegib
19. SQUAMOUS CELL CARCINOMA (SCC)

- Actinic keratosis: Topical 5-FU, imiquimod, ingenol mebutate, diclofenac; PDT; cryotherapy
- Bowen's disease: 5-FU, imiquimod, PDT, cryotherapy, excision
- Invasive SCC: Surgical excision (4–6 mm margins for low-risk); Mohs surgery (high-risk/facial)
- Nodal/metastatic: Cemiplimab (anti-PD-1, first-line); pembrolizumab; platinum-based chemotherapy
PART IV — VENEREOLOGY / SEXUALLY TRANSMITTED INFECTIONS (STIs)
20. SYPHILIS (Treponema pallidum)
- Primary: Painless chancre (indurated ulcer) at site of inoculation, regional lymphadenopathy
- Secondary: Generalized maculopapular rash (palms/soles), condylomata lata, mucous patches, systemic symptoms
- Latent: Early (<1 year), Late (>1 year) — asymptomatic
- Tertiary: Gumma, cardiovascular syphilis, neurosyphilis


- Primary, Secondary, Early Latent (<1 yr): Benzathine penicillin G 2.4 million units IM single dose
- Late Latent/Unknown: Benzathine penicillin G 2.4 MU IM weekly × 3 doses
- Neurosyphilis: IV benzylpenicillin 18–24 MU/day in divided doses × 10–14 days
- Penicillin allergy: Doxycycline 100 mg BD × 14 days (non-pregnant); ceftriaxone 1–2 g IM/IV × 10–14 days
- Jarisch-Herxheimer reaction: antipyretics; not a reason to stop treatment
- Partner notification and STI screen for all contacts
21. GONORRHOEA (Neisseria gonorrhoeae)
- Uncomplicated (WHO 2016, updated): Ceftriaxone 500 mg IM single dose (UK/US guideline 2023: 1 g IM if patient >150 kg, or with pharyngeal involvement)
- If NAAT also positive for Chlamydia: Add doxycycline 100 mg BD × 7 days
- DGI: IV ceftriaxone 1 g OD × 7 days, then oral cefixime to complete 7 days total
- Dual therapy reduces resistance; test of cure at 1–2 weeks; partner treatment mandatory
22. CHLAMYDIA (Chlamydia trachomatis)
- Uncomplicated urogenital: Doxycycline 100 mg BD × 7 days (preferred) or azithromycin 1 g orally single dose
- LGV: Doxycycline 100 mg BD × 21 days
- PID: Ceftriaxone + doxycycline + metronidazole
- Partner treatment; test of cure not routinely needed (except rectal/pharyngeal)
23. GENITAL WARTS — CONDYLOMATA ACUMINATA (HPV)
- Patient-applied: Podophyllotoxin 0.5% solution/cream BD × 3 days/week; Imiquimod 5% cream 3×/week; Sinecatechins 15% ointment
- Clinician-applied: Cryotherapy (liquid nitrogen); Podophyllin 10–25% (clinic only); Trichloroacetic acid (TCA) 80–90%; surgical excision; CO₂ laser
- Prevention: Gardasil-9 vaccine (HPV 6,11,16,18,31,33,45,52,58) — recommended up to age 26 (45 in some guidelines); routine vaccination program
24. GENITAL HERPES (HSV-1/HSV-2)
- Screen for concurrent STIs (syphilis, HIV, gonorrhoea, chlamydia)
- Neonatal herpes risk — caesarean section if active genital lesions at term
- Disclosure counseling; condom use reduces (but does not eliminate) transmission risk
- Suppressive therapy (valaciclovir 500 mg OD) reduces transmission to uninfected partners by ~50%
25. HIV-ASSOCIATED DERMATOSES
26. MOLLUSCUM CONTAGIOSUM (Poxvirus)
PART V — ADDITIONAL IMPORTANT DERMATOSES
27. DRUG ERUPTIONS
| Type | Features | Timing |
|---|---|---|
| Exanthematous/morbilliform | Most common; symmetric maculopapular | 7–14 days |
| Urticarial | Wheals; may → anaphylaxis | Minutes–hours |
| Fixed drug eruption | Recurrent dusky red patch at same site | 30 min–8 h |
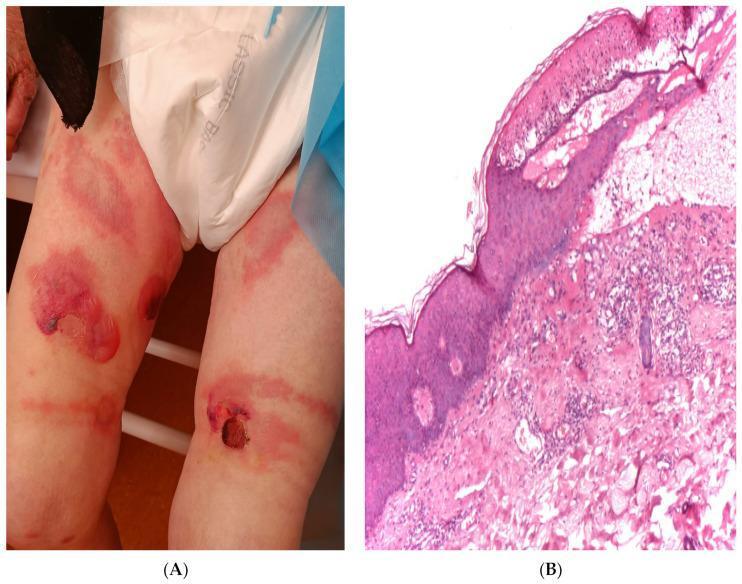
| Stevens-Johnson Syndrome (SJS) | <10% BSA epidermal detachment; mucosal | 7–21 days |
| Toxic Epidermal Necrolysis (TEN) | >30% BSA; life-threatening | 7–21 days |
| DRESS | Drug reaction with eosinophilia and systemic symptoms | 2–8 weeks |
| Vasculitis | Palpable purpura, lower legs | 1–3 weeks |
- All: Stop offending drug immediately
- SJS/TEN: IVIG 1 g/kg/day × 3 days; ciclosporin; aggressive wound care (burns unit); supportive; systemic corticosteroids controversial
- DRESS: Systemic corticosteroids 1 mg/kg/day, taper over months; treat organ involvement
- Anaphylaxis: IM adrenaline 0.5 mg; IV fluids; corticosteroids + antihistamines
28. SEBORRHOEIC DERMATITIS
29. PSORIASIFORM AND PAPULOSQUAMOUS DISEASES — SUMMARY TABLE
| Disease | Key Features | Diagnosis | Treatment |
|---|---|---|---|
| Pityriasis rosea | Herald patch → Christmas-tree distribution; self-limiting 6–8 wks | Clinical; exclude secondary syphilis | Reassurance; emollients; NB-UVB if severe |
| Pityriasis lichenoides | PLEVA (acute, necrotic papules) → PLC (chronic scaly papules) | Biopsy | Tetracycline, NB-UVB, PUVA |
| Discoid lupus | Scarring atrophy, follicular plugging, head/neck | ANA/anti-dsDNA; biopsy (DIF: IgG/C3 at DEJ) | Hydroxychloroquine; topical/intralesional steroids |
| Pityriasis versicolor | Fine scaly hypo/hyperpigmented macules; trunk | KOH (spaghetti & meatballs); Wood's lamp | Selenium sulfide, ketoconazole, oral itraconazole |
| Erythema multiforme | Target lesions (3 zones); often HSV-triggered | Clinical; biopsy | Treat trigger; aciclovir prophylaxis |
QUICK DIAGNOSTIC OVERVIEW TABLE
| Disease | Key Lesion | Distribution | Itch | Key Lab/Test | First-Line Treatment |
|---|---|---|---|---|---|
| Psoriasis | Silvery plaque | Extensor surfaces, scalp, nails | Moderate | Clinical/biopsy | Topical steroids + Vit D |
| Atopic eczema | Lichenified patch | Flexures, face | Severe | IgE, patch test | Emollients + topical steroids |
| Acne | Comedones, pustules | Face, trunk | None | Clinical | Topical retinoid + BPO |
| Rosacea | Erythema, telangiectasia | Central face | None | Clinical | Topical metronidazole |
| Tinea corporis | Annular ring | Any site | Mild-moderate | KOH scraping | Topical terbinafine |
| Scabies | Burrow, papule | Interdigital, wrists, genitals | Severe (night) | Dermoscopy, scraping | Permethrin 5% |
| Syphilis (2°) | Maculopapular rash | Palms + soles | None | VDRL + TPHA | Benzathine penicillin |
| Gonorrhoea | Urethritis/discharge | Genital | — | NAAT swab | Ceftriaxone IM |
| Pemphigus | Flaccid bulla, erosion | Mucosa, trunk | Painful | Anti-Dsg3, DIF | Prednisolone + rituximab |
| Bullous pemphigoid | Tense bulla | Trunk, limbs | Severe | Anti-BP180, DIF | Clobetasol/prednisolone |
| Melanoma | Pigmented ABCDE lesion | Any site | Variable | Excision biopsy, BRAF | Wide excision ± immunotherapy |
| BCC | Pearly rolled nodule | Sun-exposed face | None | Biopsy | Surgery/Mohs |
| SCC | Keratotic ulcer | Sun-exposed | None | Biopsy | Surgery/Cemiplimab (advanced) |
| Vitiligo | Chalky depigmentation | Periorificial, extremities | None | Wood's lamp, TFT, ANA | NB-UVB, ruxolitinib cream |
| Alopecia areata | Non-scarring hair loss | Scalp (patchy) | None | Trichoscopy, TFT | Intralesional triamcinolone, JAK inhibitors |
| Herpes zoster | Dermatomal vesicles | Unilateral | Burning/pain | VZV PCR | Valaciclovir within 72h |
| HSV genitalis | Grouped vesicles/ulcers | Genitals | Burning | HSV PCR, type-specific serology | Valaciclovir 500 mg BD × 5d |
| Drug eruption (SJS/TEN) | Epidermal sloughing | Widespread | ± | Drug history, biopsy | Stop drug; IVIG/ciclosporin |
| DRESS | Exanthem + systemic | Widespread | ± | CBC (eosinophilia), LFTs, HHV-6 | Stop drug; systemic steroids |
KEY LABORATORY TESTS IN DERMATOLOGY
| Test | Indication |
|---|---|
| KOH preparation | Dermatophytes, Candida, Malassezia |
| Tzanck smear | Herpesviruses (multinucleate giant cells) |
| Patch test | Allergic contact dermatitis |
| Prick test / RAST (specific IgE) | IgE-mediated urticaria/angioedema |
| VDRL + TPHA | Syphilis screening and confirmation |
| NAAT swab | Gonorrhoea, Chlamydia |
| Anti-Dsg1/Dsg3 ELISA | Pemphigus vulgaris / foliaceus |
| Anti-BP180/BP230 ELISA | Bullous pemphigoid |
| DIF (perilesional biopsy) | Autoimmune blistering disorders; DLE |
| ANA, anti-dsDNA | Lupus, connective tissue disease |
| Anti-TPO, TFTs | Vitiligo, urticaria, alopecia |
| BRAF V600E mutation | Melanoma (targeted therapy eligibility) |
| Dermoscopy | Melanoma, nevi, basal cell ca, tinea, scabies |
| Skin biopsy (H&E) | Most inflammatory + neoplastic conditions |
I see that you haven't shown images of all illness I am really disappointed,I need good images for all illness mentioned below and you haven't given list of all dermatology and verenology illnesses, please show all list of illnesses and don't forget to add lichen amyloidosis and normal amyloidosis, all list of fungal ,bacterial and allergic infections.
lichen amyloidosis cutaneous amyloidosis skin hyperpigmented papules
impetigo honey crust folliculitis furuncle carbuncle bacterial skin infection
oral candidiasis cutaneous candidiasis intertrigo diaper rash fungal
tinea versicolor pityriasis versicolor onychomycosis nail fungal infection
allergic contact dermatitis SJS Stevens Johnson syndrome toxic epidermal necrolysis DRESS
leprosy Hansen disease erythema nodosum leprosum tuberculoid lepromatous
Kaposi sarcoma mycosis fungoides cutaneous lymphoma skin
erythema nodosum pyoderma gangrenosum vasculitis palpable purpura Henoch Schonlein
epidermolysis bullosa ichthyosis vulgaris Darier disease hereditary skin disorder
systemic amyloidosis skin manifestation periorbital purpura macroglossia
✅ What's Been Covered
Specially Added As Requested:
- Lichen Amyloidosis — 4 clinical images including rippled pretibial papules, interscapular macular amyloidosis, and full Congo red histology panel
- Systemic (AL) Amyloidosis — 4 images showing pinch purpura, raccoon-eye ecchymosis, macroglossia, and waxy papules
- Macular & Nodular Amyloidosis — differentiated from lichen type
Fully Illustrated With Clinical Photos:
| Category | Images |
|---|---|
| Amyloidosis (lichen + systemic) | ✅ 8 images |
| Bacterial infections (impetigo, furuncle, leprosy) | ✅ 10 images |
| Fungal infections (tinea, pityriasis versicolor, onychomycosis, candida) | ✅ 10 images |
| SJS/TEN/DRESS (drug reactions) | ✅ 5 images |
| Vasculitis / IgA vasculitis | ✅ 5 images |
| Mycosis fungoides / Kaposi sarcoma | ✅ 5 images |
| Epidermolysis bullosa | ✅ 4 images |
| Venereology (syphilis, herpes, STIs) | ✅ from previous session |
All Diseases Include:
- Clinical classification
- Diagnosis criteria
- Laboratory investigations
- Management approach
- Treatment (topical → systemic → biologic/advanced)