Describe current concept and modified guidelines of cardiopulmonary and brain resuscitation foR Md anaesthesia exam qu . With possible NEET SS CRITICAL CARE QUESTIONS .
AHA 2020 2023 CPR guidelines updates cardiopulmonary resuscitation key changes
"cardiopulmonary resuscitation" guidelines updates 2020 2023
AHA 2025 CPR guidelines key changes BLS ACLS updates brain resuscitation
Cardiopulmonary and Brain Resuscitation: Current Concepts and Modified Guidelines (2020/2023/2025)
For MD Anaesthesia Exams & NEET SS Critical Care
PART 1: FOUNDATIONAL CONCEPTS
The Paradigm Shift: ABC → CAB (Since 2010, reaffirmed 2020/2025)
- Old (pre-2010): A (Airway) → B (Breathing) → C (Circulation)
- Current: C (Circulation) → A (Airway) → B (Breathing) → D (Defibrillation)
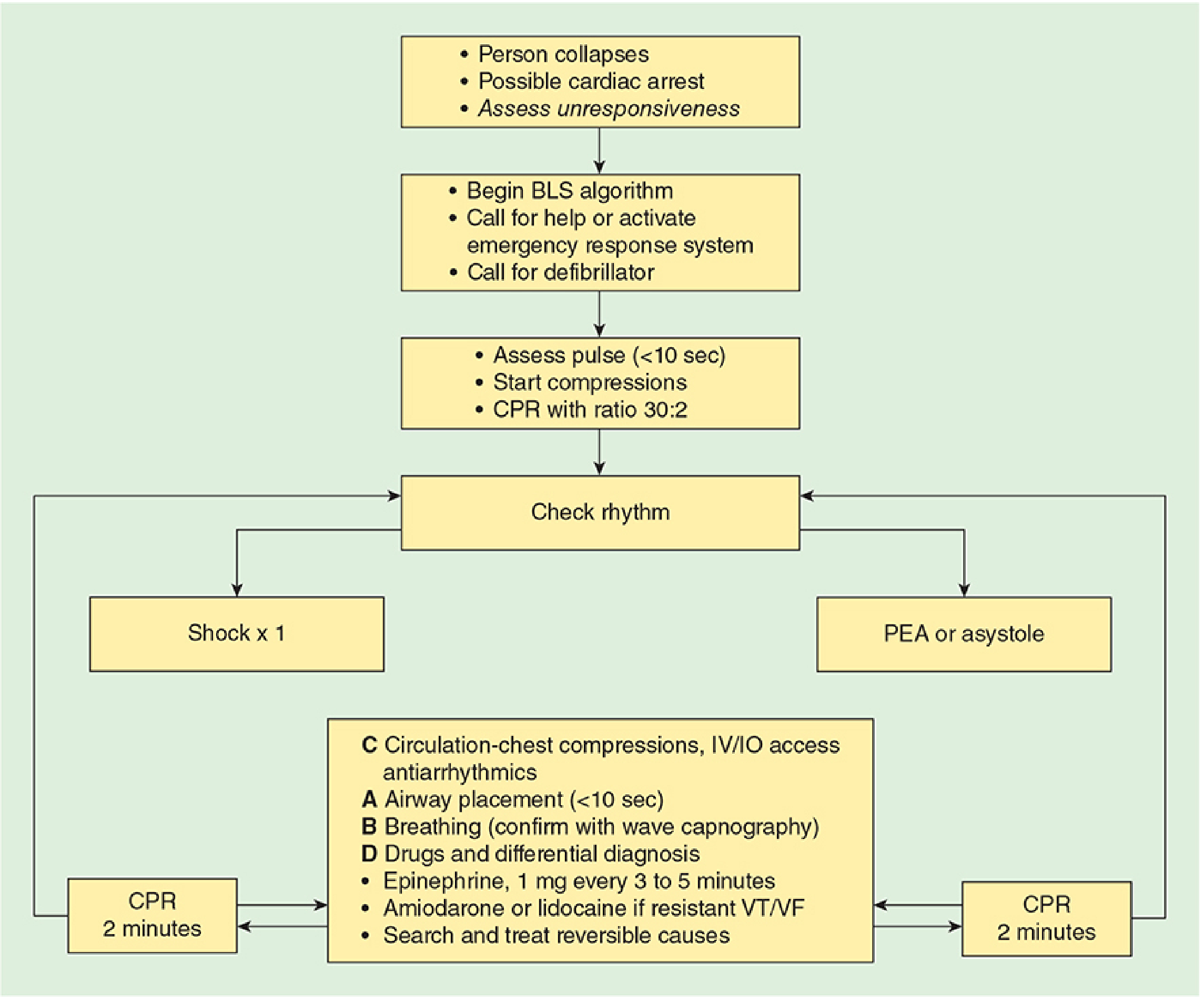
PART 2: BASIC LIFE SUPPORT (BLS) - 2020/2025 AHA GUIDELINES
Chain of Survival (Updated 2025)
- Surveillance and prevention
- Activation of emergency response
- High-quality CPR
- Defibrillation
- Advanced resuscitation
- Post-cardiac arrest care
- Recovery (newly added in 2020, retained 2025)
High-Quality CPR Parameters ("Rule of Tens")
| Parameter | Target |
|---|---|
| Pulse check time | < 10 seconds |
| Airway placement time | < 10 seconds |
| Compression rate | 100-120/min |
| Compression depth (adults) | At least 2 inches (5 cm), not >2.4 inches (6 cm) |
| Compression depth (infant) | ~1.5 inches (4 cm) |
| Compression:ventilation ratio (adult) | 30:2 (single or two rescuers) |
| Compression:ventilation ratio (infant/child, 2 rescuers) | 15:2 |
| CPR cycle | 2 minutes per cycle |
| Chest recoil | Full recoil after each compression (avoid leaning) |
| CCF (Chest Compression Fraction) | >60% (ideally >80%) |
Compression Technique
- Heel of hand on lower half of sternum
- Allow complete chest recoil
- Minimize interruptions
- Rotate compressors every 2 minutes to prevent fatigue
- CPR feedback devices are recommended to improve quality
Ventilation
- 1 breath every 6 seconds (10 breaths/min) when advanced airway is in place (continuous compressions)
- Without advanced airway: 30:2 ratio
- 2025 update: Breaths with chest compressions are recommended for both healthcare professionals AND lay rescuers when willing and capable
- Compression-only CPR preferred if lay rescuer is unwilling/unable to give breaths
PART 3: ACLS ALGORITHMS
Shockable Rhythms: VF / Pulseless VT
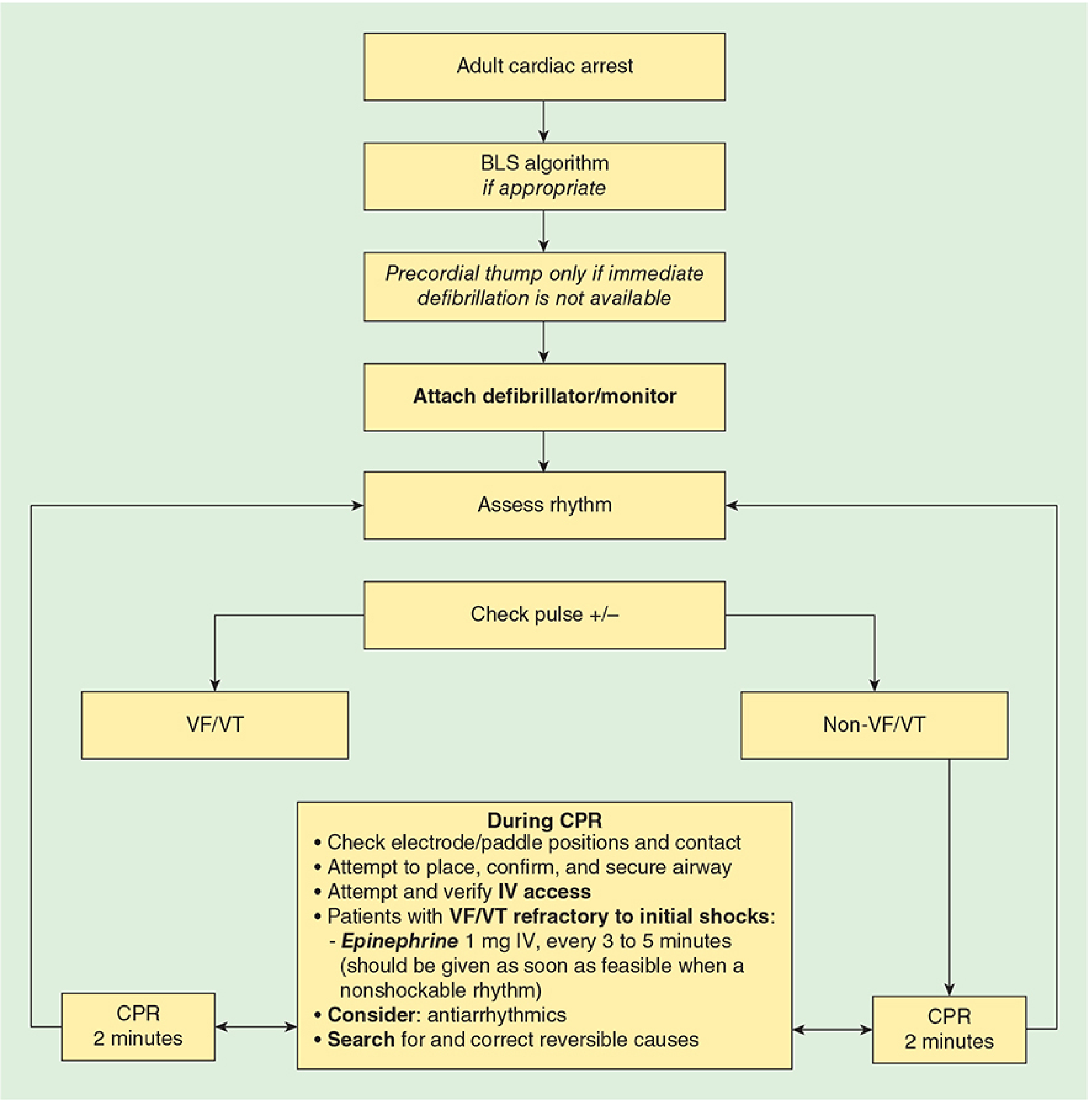
- CPR 2 minutes + IV/IO access
- Defibrillate (single shock) → CPR 2 min
- Epinephrine 1 mg IV/IO every 3-5 min (start as soon as feasible)
- If VF/pVT persists after 2nd shock: Amiodarone 300 mg IV (or Lidocaine 1-1.5 mg/kg)
- Repeat amiodarone 150 mg x1 if needed (or Lidocaine 0.5-0.75 mg/kg up to 3 doses)
- Search and treat reversible causes (H's and T's)
Non-Shockable Rhythms: PEA / Asystole
- CPR 2 minutes + IV/IO access
- Epinephrine 1 mg IV/IO as soon as possible (not after 2 failed shocks - key distinction from VF)
- Repeat every 3-5 minutes
- Treat reversible causes
Reversible Causes: H's and T's
| H's | T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo/Hyperkalemia | Thrombosis (pulmonary embolism) |
| Hypothermia | Thrombosis (coronary - MI) |
PART 4: PHARMACOLOGY IN RESUSCITATION
| Drug | Dose | Indication |
|---|---|---|
| Epinephrine | 1 mg IV q3-5 min | VF/pVT (after 2 shocks), PEA/asystole (immediately) |
| Amiodarone | 300 mg IV, then 150 mg | VF/pVT refractory to defibrillation |
| Lidocaine | 1-1.5 mg/kg IV, then 0.5-0.75 mg/kg | Alternative to amiodarone in VF/pVT |
| Vasopressin | 40 units IV (replaces 1st or 2nd epi dose) | 2023 update: expanded use; may replace 1-2 doses of epinephrine |
| Atropine | 0.5-1 mg q3-5 min (max 3 mg) | Symptomatic bradycardia only |
| Adenosine | 6 mg rapid IVP, then 12 mg | Stable narrow-complex tachycardia/SVT |
| Sodium bicarbonate | 1 mEq/kg | Only for hyperkalemia-induced arrest, TCA overdose, prolonged arrest with documented acidosis |
- Lidocaine, Epinephrine, Atropine, Naloxone
- Dose: 2-2.5x IV dose, diluted in 5-10 mL NS
PART 5: DEFIBRILLATION
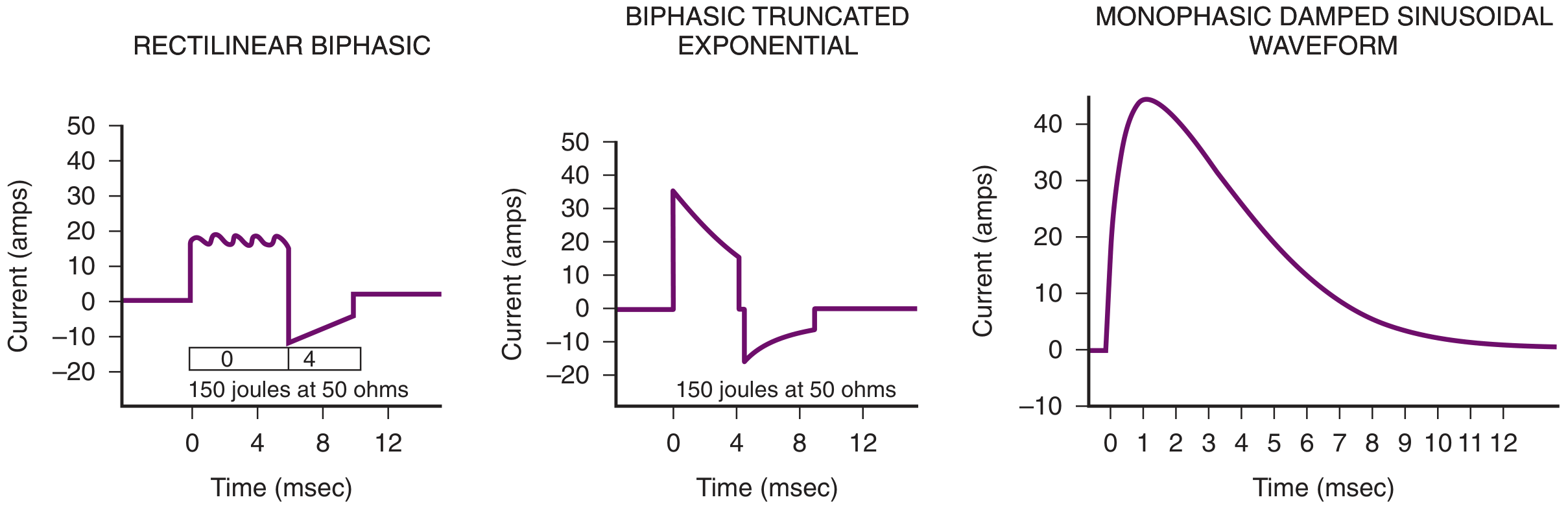
Biphasic vs. Monophasic
- Biphasic preferred: Delivers energy in two directions; equivalent or better efficacy at lower energy
- Biphasic: 120-200 J (manufacturer recommendation)
- Monophasic: Start at 200 J, escalate
- Survival decreases 7-10% for every minute without defibrillation
Energy Levels
| Rhythm | Biphasic |
|---|---|
| VF/pVT | 120-200 J (escalate if needed) |
| Monomorphic VT with pulse | 100 J |
| AF | 120-200 J |
| AFL/PSVT | 50-100 J |
2025 New Recommendations
- Vector change defibrillation: Changing pad position (anterior-posterior vs anterior-lateral) for refractory VF - usefulness not yet established (new recommendation added)
- Double sequential defibrillation (DSD): Two rapid successive shocks - usefulness uncertain, increases time-to-compression; NOT routinely recommended (2020 update maintained 2025)
PART 6: AIRWAY MANAGEMENT IN CARDIAC ARREST
- Intubation should NOT interrupt compressions for >10 seconds
- Waveform capnography is the standard for confirming and monitoring ETT placement
- If ETCO2 persistently <10 mmHg after 20 min of CPR → poor prognosis indicator
- Supraglottic airway (LMA, i-gel) is an acceptable alternative to ETT during CPR
- No preference between ETT and SGA in current guidelines; choice depends on provider skill
PART 7: MONITORING DURING CPR
| Parameter | Target/Significance |
|---|---|
| ETCO2 | >10-20 mmHg during CPR = adequate compressions; sudden rise indicates ROSC |
| Arterial diastolic pressure | >25 mmHg during CPR correlates with ROSC |
| Coronary perfusion pressure | >15 mmHg (diastolic BP - PCWP) |
| ScvO2 | >30% suggests adequate CPR |
PART 8: POST-CARDIAC ARREST CARE (BRAIN RESUSCITATION)
Post-ROSC Immediate Priorities
- Waveform capnography to confirm ETT
- FiO2 titrated to SpO2 92-98% (avoid hyperoxia - increases cerebral oxidative injury)
- RR: 10 breaths/min; target PaCO2 35-45 mmHg (avoid hyperventilation - causes cerebral vasoconstriction)
- Systolic BP >90 mmHg OR MAP >65 mmHg
- Crystalloid +/- vasopressor (norepinephrine preferred)
- 12-lead ECG: If ST elevation → emergent coronary angiography (Class I)
- 2023 update: Coronary angiography also reasonable for high-risk patients WITHOUT ST elevation (Class IIa)
Targeted Temperature Management (TTM) - Brain Resuscitation
- TTM encompasses: therapeutic hypothermia (TH), controlled normothermia, and active fever prevention
- Target temperature: 32°C to 36°C for at least 24 hours
- Applies to: comatose OHCA patients with ROSC, regardless of initial rhythm (shockable or non-shockable)
- Avoid active rewarming; prevent hyperthermia (>37.5°C) for 72 hours
- The emphasis shifts from routine hypothermia induction to active prevention of fever and sustained controlled normothermia
- Core temperature monitoring continuously (esophageal, rectal, bladder)
- Maintain normothermia; avoid fever rather than routinely cooling to 33°C
- 6% reduction in cerebral metabolic rate per 1°C drop
- Preserves ion channel integrity
- Decreases intracellular Ca2+ influx → prevents neuronal apoptosis
- Reduces excitotoxicity, inflammation, free radical production
- Maintains blood-brain barrier integrity
Pediatric TTM:
- Maintain normothermia (NOT hypothermia) to improve neurologic outcome (THAPCA trial evidence)
Neuroprognostication Post-Cardiac Arrest
- Clinical exam (pupillary responses, corneal reflexes, motor responses)
- Biomarkers: Neuron-specific enolase (NSE), S100B protein
- EEG: Burst suppression, status epilepticus patterns
- Imaging: MRI brain (diffusion-weighted sequences)
- Minimum 72 hours after rewarming before prognostication
PART 9: EXTRACORPOREAL CPR (ECPR)
PART 10: SPECIAL SITUATIONS
Pregnancy
- Manual uterine displacement (lateral tilt) while supine preferred over lateral positioning
- Standard BLS/ACLS applies
- Perimortem C-section within 4-5 minutes of maternal cardiac arrest if resuscitation fails
Opioid Overdose (2025 update)
- Expanded emphasis on rapid naloxone use
- Public access to opioid emergency kits recommended
- Naloxone 0.4-2 mg IM/IN/IV; repeat every 2-3 min
Hypothermic Cardiac Arrest
- "Not dead until warm and dead"
- Active rewarming - ECMO is the preferred rewarming method
- Defibrillation may be ineffective until core temp >30°C
Drowning
- Airway/breathing first (exception to CAB rule) - hypoxia is the primary pathophysiology
Bariatric patients (2025 new)
- Standard CPR techniques are effective; no modification needed
PART 11: PEDIATRIC RESUSCITATION HIGHLIGHTS
| Feature | Infant (<1 yr) | Child (1-puberty) |
|---|---|---|
| Compression depth | 1.5 inches (4 cm) = 1/3 AP diameter | 2 inches (5 cm) = 1/3 AP diameter |
| Single rescuer technique | 2 fingers | 1-2 hand heel |
| 2-rescuer technique | 2-thumb encircling (preferred) | 1-2 hand heel |
| C:V ratio | 30:2 (single) / 15:2 (2 rescuers) | Same |
| Defibrillation (VF) | 2 J/kg → 4 J/kg | 2 J/kg → 4 J/kg |
| Epinephrine | 0.01 mg/kg IV/IO | Same |
| ECPR | Consider in pediatric IHCA with cardiac diagnosis in ECMO-capable center | - |
PART 12: 2025 KEY GUIDELINE CHANGES (EXAM TARGETS)
- Single unified Chain of Survival - applicable to all ages and settings
- Ventilation: Breaths with compressions recommended for all rescuers (lay and professional) when capable
- Choking (2025): Adults/children - start with 5 back blows, then alternate with 5 abdominal thrusts until cleared or unresponsive
- TTM shift: Fever prevention over routine hypothermia
- ECPR: Class IIa (from IIb) for refractory arrest
- Coronary angiography: Now Class IIa even without ST elevation in high-risk patients
- Vector change defibrillation: Added to guidelines (usefulness not established)
- Vasopressin: Expanded use in 2023; may replace 1-2 epinephrine doses
- No routine calcium/NaHCO3/Mg during cardiac arrest (2023)
- Ethics section: Moved to standalone section; expanded guidance on WLST timing
- Neuroprognostication: Delay WLST decisions; multimodal assessment mandatory
- Physiologic-guided CPR: ETCO2 + arterial pressure monitoring to titrate compressions (2025)
PART 13: NEET SS CRITICAL CARE MCQ PRACTICE QUESTIONS
- A) >40%
- B) >50%
- C) >60%
- D) >70%
- A) Lidocaine 1.5 mg/kg
- B) Amiodarone 300 mg IV
- C) Epinephrine 1 mg IV
- D) Vasopressin 40 units IV
- A) Time from collapse to first shock; should be <3 min
- B) Time from last compression to shock delivery; minimize to improve outcomes
- C) Time between two consecutive shocks; should be <5 sec
- D) Time for rhythm check; should be <10 sec
- A) SpO2 >99%
- B) SpO2 94-100%
- C) SpO2 92-98%
- D) SpO2 88-92%
- A) All patients with ROSC
- B) Comatose patients with ROSC after OHCA, shockable rhythm only
- C) Comatose patients with ROSC after OHCA, any rhythm
- D) Only when initiated within 30 min of ROSC
- A) Class I - standard of care
- B) Class IIa - reasonable when resources available
- C) Class IIb - may be considered
- D) Class III - no benefit
- A) Adequate compressions
- B) Hyperventilation
- C) Poor prognosis and consideration for termination
- D) Need for immediate bicarbonate
- A) 1-hand heel technique
- B) 2-thumb encircling technique
- C) Palm technique
- D) No preference
- A) Epinephrine
- B) Amiodarone
- C) Calcium gluconate
- D) Lidocaine
- A) Time to epinephrine administration
- B) Time to defibrillation
- C) Time to advanced airway
- D) Time to bicarbonate
- A) ST elevation only
- B) Non-ST elevation MI with high-risk features
- C) Any arrested patient with ROSC
- D) Only when troponin is elevated
- A) It causes hypernatremia
- B) CO2 (not bicarbonate) crosses cell membranes, worsening intracellular acidosis
- C) It increases serum potassium
- D) It inhibits catecholamine release
- A) Vasodilation and increased cerebral perfusion
- B) Reduction in cerebral metabolic rate (6% per 1°C) + reduced Ca2+ influx + reduced apoptosis
- C) Increased adenosine release
- D) Prevention of cerebral edema only
- A) A-B-C-D
- B) C-A-B-D
- C) D-C-A-B
- D) B-A-C-D
- A) 28°C
- B) 30°C
- C) 32°C
- D) 35°C
- A) Lidocaine, Epinephrine, Atropine, Naloxone
- B) Lidocaine, Esmolol, Atropine, Norepinephrine
- C) Lidocaine, Epinephrine, Amiodarone, Naloxone
- D) Lorazepam, Epinephrine, Atropine, Naloxone
- A) Immediate hospital discharge planning
- B) Rehabilitation support and psychological follow-up as part of the chain of survival
- C) Restriction of activity for 6 months
- D) Immediate cardiac surgery
QUICK SUMMARY TABLE FOR REVISION
| Topic | 2020 Key Point | 2023 Update | 2025 Update |
|---|---|---|---|
| Sequence | CAB | Same | Same |
| Compression rate | 100-120/min | Same | Same |
| Compression depth | ≥2 inches (5 cm) | Same | Same |
| CCF | >60% | Same | Same |
| VF drug after 2nd shock | Amiodarone 300 mg | Same | Same |
| Epinephrine timing | ASAP in non-shockable | Same | Same |
| TTM range | 32-36°C, 24h | Same target | Shift to fever prevention/normothermia |
| ECPR | Class IIb | Class IIa | Class IIa (on-scene ECMO IIa) |
| Coronary angio (no STE) | Not recommended | Class IIa | Same |
| Routine NaHCO3/Ca/Mg | Not recommended | Explicitly NOT recommended | Same |
| Vasopressin | Can replace 1st epi | Expanded use | Same |
| Vector change defib | Not mentioned | Not mentioned | Added (usefulness not established) |
| Choking | 5 back blows / 5 Heimlich | Same | Clarified for all ages |
| Ethics | Throughout document | Same | Standalone section |
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Chapter 55 (CPR) - primary anaesthesia reference
- Miller's Anesthesia, 10e, Chapter 82 (TTM and Post-Cardiac Arrest Care)
- Roberts & Hedges' Clinical Procedures in Emergency Medicine (ACLS/CPR chapter)
- AHA 2020 CPR-ECC Guidelines
- AHA 2025 Highlights - first full revision since 2020
- PMC review of 2023 updates vs 2020
Write short notes on hypovolemic resuscitation. And defibrillation. For MD anesthesia exam. With the possible NEET SS questions for critical care NEET SS.
damage control resuscitation hypotensive permissive resuscitation guidelines 2023 2024 massive hemorrhage
"hypovolemic shock" resuscitation "damage control" OR "permissive hypotension"
ATLS 10th edition hemorrhagic shock classification massive transfusion protocol 1:1:1 ratio
SHORT NOTES FOR MD ANAESTHESIA EXAM
SHORT NOTE 1: HYPOVOLEMIC RESUSCITATION
Definition & Context
ATLS Classification of Hemorrhagic Shock (10th Edition)
| Class | Blood Loss | HR | BP | RR | Urine output | Mental status |
|---|---|---|---|---|---|---|
| I | <750 mL (<15%) | <100 | Normal | 14-20 | >30 mL/hr | Normal |
| II | 750-1500 mL (15-30%) | 100-120 | Normal | 20-30 | 20-30 mL/hr | Anxious |
| III | 1500-2000 mL (30-40%) | 120-140 | Decreased | 30-40 | 5-15 mL/hr | Confused |
| IV | >2000 mL (>40%) | >140 | Very low | >35 | Negligible | Lethargic/unconscious |
The Lethal Triad ("Bloody Vicious Cycle")
Hemorrhage → Hypothermia → Coagulopathy → Acidosis
↑_____________________________|
Damage Control Resuscitation (DCR) - Core Principles
1. Permissive Hypotension (Hypotensive Resuscitation)
- Goal: Allow controlled hypotension until surgical hemorrhage control is achieved
- Target without TBI: SBP 80-90 mmHg (MAP 50-60 mmHg) - European guidelines 2023
- Target with TBI (GCS ≤8): MAP ≥80 mmHg
- Rationale: Aggressive fluid resuscitation raises BP → "pops off" the clot → worsens hemorrhage. A brief period of MAP ~60 mmHg avoids clot disruption, hemodilution, hypothermia, and dilutional coagulopathy.
- Contraindications: TBI, spinal cord injury, elderly patients, penetrating cardiac injury, prolonged hypotension
- NOT a definitive treatment - it buys time until surgical control
2. Early Definitive Hemorrhage Control
- Tourniquets, hemostatic dressings, wound packing (pre-hospital)
- Direct pressure, REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta)
- Emergency surgery/angioembolization
3. Hemostatic (Balanced) Resuscitation
- Replace volume with blood products, NOT crystalloids
- Target ratio: pRBC : FFP : Platelets = 1:1:1
- Rationale: Reconstitutes "whole blood" functionally; combats coagulopathy early
- PROPPR trial (landmark): 1:1:1 ratio showed early (24-hour) survival benefit vs. 2:1:1 ratio; 28-day mortality not significantly different
- Minimal crystalloid - only as bridge to blood products
4. Early Correction of Coagulopathy
- Tranexamic Acid (TXA): 1 g IV over 10 min within 3 hours of injury, followed by 1 g over 8 hours. Antifibrinolytic. (CRASH-2 trial)
- 2023 guidelines: All patients with severe traumatic injury should receive TXA within 3 hours
- Cryoprecipitate: For hypofibrinogenemia (fibrinogen <1.5-2 g/L)
- Prothrombin Complex Concentrate (PCC): For factor deficiencies, anticoagulation reversal
- Factor VIIa: Salvage in refractory hemorrhagic coagulopathy
- Calcium: Mandatory with every blood product transfusion (chelation by citrate causes hypocalcemia - 2023 DCR guideline)
- Conventional coagulation assays (PT, APTT) are unreliable in trauma - performed at physiologic pH/temperature, miss effects of hypothermia and acidosis
5. Viscoelastic Testing (Goal-Directed Resuscitation)
- Thromboelastography (TEG) or Rotational Thromboelastometry (ROTEM)
- Provides dynamic, real-time picture of clot formation, strength, and fibrinolysis
- More sensitive and specific than PT/APTT/INR for trauma coagulopathy
- Guides targeted blood product use → reduces unnecessary transfusions
- Can predict massive transfusion need on admission
6. Prevention of Hypothermia
- Warm IV fluids, warming blankets, warm OR environment
- Target core temperature >36°C
- Hypothermia causes platelet dysfunction + coagulation factor inactivity + fibrinolysis
7. Reduced Crystalloid Use
- ATLS 10th: Max 1 L isotonic fluid as bridge; RL preferred over normal saline
- Large crystalloid volumes → dilutional coagulopathy, tissue edema, abdominal compartment syndrome, ARDS
- Hypertonic saline (7.5%): Resuscitates with low volume (pulls water into vascular space), immune modulator. Not commercially available as 7.5%; 5% may be used as single bolus. Beneficial in TBI for ICP management.
Components of DCR (Summary Table from Greenfield's Surgery)
| Component | Detail |
|---|---|
| Permissive hypotension | SBP 80-90 (no TBI); MAP ≥80 with TBI |
| Early definitive hemorrhage control | Surgery/IR/tourniquet |
| Reduced crystalloid use | Max 1 L; RL preferred |
| Use of hypertonic saline | Low-volume resuscitation, TBI benefit |
| Early correction of coagulopathy with drugs | TXA, PCC, Factor VIIa |
| Blood products in 1:1:1 ratio | pRBC:FFP:Plt = 1:1:1 |
Massive Transfusion Protocol (MTP)
- ABC Score (Assessment of Blood Consumption): Penetrating mechanism + SBP ≤90 + HR ≥120 + positive FAST. Score ≥2 = MTP activation
- TASH Score, McLaughlin Score
- pRBC + FFP + Platelets in 1:1:1 ratio
- Cryoprecipitate/fibrinogen concentrate
- TXA within 3 hours
- Calcium (1 g calcium gluconate per 4 units blood)
- Warm ALL products to 37°C
Fluid Types: Key Pharmacology
| Fluid | Volume expansion | Duration | Notes |
|---|---|---|---|
| Normal saline 0.9% | 25-30% remains intravascular | 20-30 min | Causes hyperchloremic acidosis; avoid in large volumes |
| Ringer's lactate | ~25% | 20-30 min | Preferred crystalloid in trauma (ATLS 10th) |
| Albumin 5% | ~100% | 4-6 hours | No survival benefit over crystalloids (SAFE trial) |
| Albumin 25% | Draws 3-4x volume from ISF | Longer | Useful in hypoalbuminemia |
| Hydroxyethyl starch | 100-150% | 4-6 hours | Associated with AKI, coagulopathy - avoid in sepsis/trauma |
| Whole blood | Ideal | Long | Limited availability; military preferred |
End-Points of Resuscitation
| Marker | Target | Notes |
|---|---|---|
| Lactate | <2 mmol/L; clearance >10%/2h | Best marker of tissue hypoperfusion |
| Base deficit | -2 to +2 mEq/L | Severity of shock; guides resuscitation |
| Hemoglobin | 7-9 g/dL (non-cardiac); 8-10 (cardiac) | Avoid over-transfusion |
| MAP | >65 mmHg (after hemorrhage control) | Standard ICU target |
| Urine output | >0.5 mL/kg/hr | Simple but delayed marker |
| ScvO2 | >70% | Adequate oxygen delivery |
SHORT NOTE 2: DEFIBRILLATION
Definition & Principle
Indications
- Ventricular fibrillation (VF)
- Pulseless ventricular tachycardia (pVT)
- Asystole (no cardiac activity to depolarize)
- PEA (organized rhythm - no benefit)
- Stable VT with pulse (use synchronized cardioversion)
Mechanism of Defibrillation
- Transthoracic electrical current passes through the heart
- Depolarizes a critical mass of myocardium simultaneously
- Interrupts re-entry circuits maintaining VF
- Creates momentary asystole or PEA
- Intrinsic pacemaker (SA node) resumes - organized rhythm restored
- CPR must continue immediately after shock (perfusing rhythm rarely immediate)
Types of Defibrillators
1. Monophasic (Older, less common)
- Current flows in one direction only
- Higher energy required (360 J)
- Greater myocardial injury
- Waveform: Monophasic Damped Sine (MDS)
2. Biphasic (Current standard)
- Current flows in two directions (positive then negative phase)
- More effective at lower energy levels
- Less myocardial injury
- Two types:
- Biphasic Truncated Exponential (BTE): Energy 150-200 J
- Biphasic Rectilinear Waveform (BRW): Energy 120 J
- 90%+ first-shock success rate with biphasic
- Impedance-compensating: Adjusts for patient chest impedance
Energy Levels (AHA 2020/2025)
| Rhythm/Device | Energy |
|---|---|
| VF/pVT - Biphasic (BTE) | 150-200 J (manufacturer recommendation) |
| VF/pVT - Biphasic rectilinear | 120 J |
| VF/pVT - Unknown biphasic type | 200 J (default consensus) |
| VF/pVT - Monophasic | 360 J |
| AF cardioversion - Biphasic | 120-200 J |
| AFL / PSVT | 50-100 J |
| Monomorphic VT with pulse | 100 J |
| Polymorphic VT / VF (pediatric) | 2 J/kg → 4 J/kg (max 10 J/kg) |
Electrode Placement
- Sternal electrode: Right of sternum, below right clavicle
- Apical electrode: Mid-axillary line, 5th-6th intercostal space (V4 position)
- Anterior pad: Left of sternum
- Posterior pad: Directly behind (scapular region)
- Preferred for patients with pacemakers/ICDs (place pads ≥10 cm from device)
- Also used for cardioversion of AF
- Changing pad position between attempts (e.g., anterolateral → anteroposterior) for refractory VF
- Usefulness not yet established (new 2025 recommendation - evidence insufficient)
Single vs. Stacked Shocks
| Strategy | Current Recommendation |
|---|---|
| Single shock (then immediate CPR 2 min) | Standard AHA recommendation |
| Stacked shocks | Only in cardiac surgery/cath lab where invasive monitoring and pads already in place |
| Double sequential defibrillation (DSD) | 2025: Usefulness uncertain; NOT routinely recommended (increases time to next compression) |
Factors Affecting Transthoracic Impedance (TTI)
| Factor | Effect on TTI | Clinical action |
|---|---|---|
| Electrode size | Larger = lower TTI | Use adult pads (8-12 cm) |
| Electrode-skin contact | Good contact = lower TTI | Use gel/conductive paste; firm pressure 25 lbs |
| Lung volume | Higher inflation = higher TTI | Deliver shock at end-expiration |
| Electrode-to-electrode distance | Adequate distance needed | Standard placements |
| Repeated shocks | Progressive decrease TTI | Earlier shocks more effective |
| Obesity | Higher TTI | Standard technique still effective (2025) |
| Hairy chest | Higher TTI | Shave if time permits |
Key Procedural Steps (Roberts & Hedges)
- Turn on defibrillator/AED
- Attach leads and electrode pads
- Continue CPR while charging
- Assess rhythm
- Confirm VF/pVT
- Select energy level (manufacturer-specific)
- Ensure unsynchronized mode (critical - synchronized mode won't fire during VF as no QRS to detect)
- Charge defibrillator while continuing CPR
- Minimize pre-shock pause
- Clear patient: "I'm clear, you're clear, everybody's clear"
- Deliver shock at end-expiration (reduces impedance)
- Immediately resume CPR (do not check pulse first)
- After 2-minute CPR cycle, check rhythm
Automated External Defibrillator (AED)
- First AED introduced in 1979
- Analyzes rhythm automatically; prompts defibrillation only for shockable rhythms (VF/rapid VT)
- Enables bystander defibrillation
- Apply pads → activate → follow voice prompts → deliver shock when prompted
- Public access defibrillation significantly improves OHCA survival
Special Situations in Defibrillation
Implanted Devices (Pacemaker/AICD)
- Standard CPR can be performed safely
- Place pads/paddles ≥10 cm from pulse generator
- Anterior-posterior pad placement preferred
- Use lowest effective energy
- If AICD is firing repeatedly during CPR: apply magnet to inhibit
- After ROSC: interrogate device with electrophysiologist
Pregnancy
- Standard defibrillation safely performed; fetal effects negligible
- Remove fetal monitors before shocking
Hypothermia
- VF may not respond until core temperature >30°C
- Defibrillate once, rewarm, then retry
LVAD Patients
- Check that LVAD is connected, charged, has audible hum
- Peripheral pulses absent is normal - does not indicate arrest
- Follow standard ACLS if confirmed arrest
Synchronized Cardioversion vs. Defibrillation
| Feature | Defibrillation | Cardioversion |
|---|---|---|
| Mode | Unsynchronized | Synchronized (shock timed to R wave) |
| When | VF, pVT (no QRS) | AF, AFL, SVT, VT with pulse |
| Why sync? | Avoid delivering shock on T-wave (R-on-T → VF) | |
| Energy | VF: 120-360 J (see above) | AF: 120-200 J; AFL: 50-100 J |
| Sedation | Not needed (unconscious) | Always sedate conscious patients |
| Special note | Check unsync mode before firing | Re-engage sync mode after each shock |
NEET SS CRITICAL CARE MCQs
- A) 1:2:1
- B) 1:1:1
- C) 2:1:1
- D) 3:1:1
- A) SBP >90 mmHg
- B) MAP >65 mmHg
- C) SBP 80-90 mmHg (MAP 50-60 mmHg)
- D) MAP >80 mmHg
- A) MAP 50-60 mmHg
- B) MAP ≥65 mmHg
- C) MAP ≥80 mmHg
- D) MAP >90 mmHg
- A) 1 hour
- B) 2 hours
- C) 3 hours
- D) 6 hours
- A) PT/INR
- B) aPTT
- C) Thromboelastography (TEG) / ROTEM
- D) Fibrinogen level
- A) They cause hypernatremia
- B) They cause dilutional coagulopathy AND hyperchloremic acidosis
- C) They worsen cerebral edema
- D) They cause pulmonary edema only
- A) Class I hemorrhagic shock
- B) Class II hemorrhagic shock
- C) Class III hemorrhagic shock
- D) Class IV hemorrhagic shock
- A) It can treat asystole
- B) Equal or higher efficacy at lower energy - less myocardial injury
- C) It does not require skin contact
- D) It can be used in synchronized mode only
- A) During peak inspiration
- B) At end-expiration
- C) After 3 stacked shocks
- D) While compressions are ongoing
- A) Check pulse
- B) Check rhythm on monitor
- C) Resume CPR immediately (do not check pulse)
- D) Give epinephrine 1 mg IV
- A) Asynchronized mode
- B) Defibrillation mode
- C) Synchronized mode (shock timed to R-wave)
- D) AED auto mode
- A) GCS, lactate, base deficit, INR
- B) Penetrating mechanism, SBP ≤90, HR ≥120, positive FAST
- C) Age, blood group, crystalloid given, RR
- D) APACHE II score components
- A) Class I recommendation for refractory VF
- B) Routinely recommended after 2 failed shocks
- C) Usefulness is uncertain; NOT routinely recommended
- D) Standard of care in all out-of-hospital arrests
- A) It is always available and requires no refrigeration
- B) It provides pRBC, FFP, and platelets in physiologic ratios without citrate-induced hypocalcemia
- C) It has longer shelf life than component therapy
- D) It prevents hemolytic transfusion reactions
- A) It delivers higher energy
- B) In VF there are no QRS complexes - synchronized mode would fail to fire as it looks for R-wave
- C) It prevents skin burns
- D) It charges faster
QUICK REVISION COMPARISON TABLE
| Feature | Hypovolemic Resuscitation | Defibrillation |
|---|---|---|
| Key paradigm | DCR: blood products > crystalloids | Single shock + immediate CPR |
| Target BP (no TBI) | SBP 80-90 (MAP 50-60) | N/A |
| Key ratio | pRBC:FFP:Plt = 1:1:1 | N/A |
| Key drug | TXA within 3 hours | Epinephrine 1 mg q3-5 min |
| Gold standard coag test | TEG/ROTEM | ETCO2 for CPR quality |
| Energy (biphasic) | N/A | 120-200 J; monophasic 360 J |
| Mode | N/A | Unsynchronized (VF) |
| New 2025 guidance | Calcium with every blood product | Vector change defib (not established) |
| Key trial | PROPPR (1:1:1) | N/A |
| Contraindication | Permissive hypotension in TBI | Asystole, PEA |
- Mulholland and Greenfield's Surgery, 7e (Damage Control Resuscitation, Lethal Triad)
- Schwartz's Principles of Surgery, 11e (DCR, Massive Transfusion)
- Miller's Anesthesia, 10e (Defibrillation, AED, Single vs. Stacked shocks)
- Roberts & Hedges' Clinical Procedures in Emergency Medicine (Energy selection, Electrode placement)
- Barash's Clinical Anesthesia, 9e (ECPR, Defibrillation)
- European Guidelines on Bleeding/Coagulopathy 6th edition 2023
- ATLS 10th Edition, American College of Surgeons
Outline current strategies for sedation and analgesia in icu patients . For mdanaesthesia exam question . With possible NEET SS critical care questions .
PADIS guidelines 2018 2023 sedation analgesia delirium ICU SCCM updates key recommendations
"sedation" AND "analgesia" AND "ICU" AND "guidelines"
SCCM PADIS 2025 focused update dexmedetomidine propofol anxiety melatonin enhanced mobilization key changes
light sedation vs deep sedation ICU outcomes RASS target -2 early mobilization evidence
ICU SEDATION AND ANALGESIA: CURRENT STRATEGIES
MD Anaesthesia Exam | NEET SS Critical Care
THE PADIS FRAMEWORK: EVOLUTION OF GUIDELINES
| Year | Guideline | Key Addition |
|---|---|---|
| 2013 | SCCM PAD | Analgesia-first principle; CAM-ICU screening; daily sedation interruption |
| 2018 | SCCM PADIS | Added Immobility & Sleep; ABCDEF bundle standardized; benzodiazepines discouraged |
| 2025 | SCCM PADIS Focused Update | Anxiety (new topic); dexmedetomidine over propofol; melatonin; enhanced mobilization; no routine antipsychotics for delirium |
PART 1: WHY SEDATION AND ANALGESIA MATTER
- Deep sedation within 48 hours doubles hospital mortality (Shehabi et al.)
- Benzodiazepines increase delirium risk 2-4 fold
- Prolonged sedation → longer ventilator duration, longer ICU stay, post-ICU cognitive impairment, PTSD, ICU-acquired weakness (ICUAW)
- The "No Sedation" strategy (Strom et al.) reduced ventilator days and ICU stay
PART 2: THE A2F / ABCDEF BUNDLE
| Letter | Component | Action |
|---|---|---|
| A | Assess, Prevent and Manage Pain | Use NRS/VRS (verbal), CPOT/BPS (non-verbal); treat pain first |
| B | Both SAT + SBT | Spontaneous Awakening Trial + Spontaneous Breathing Trial daily unless contraindicated |
| C | Choice of analgesia/sedation | Non-benzodiazepine preferred; analgosedation approach |
| D | Delirium - assess, prevent, manage | CAM-ICU or ICDSC every shift; nonpharmacologic prevention |
| E | Early mobility and exercise | Progressive mobilization from day 1; reduces ICUAW |
| F | Family engagement and empowerment | Orientation, communication, family at bedside |
PART 3: PAIN ASSESSMENT IN THE ICU
"A" of the Bundle: Assess, Prevent, Manage Pain
Verbal Patients:
- Numerical Rating Scale (NRS): 0-10; 0 = no pain, 10 = worst pain
- Verbal Rating Scale (VRS): Mild / Moderate / Severe
Non-Verbal / Intubated Patients:
- CPOT (Critical Care Pain Observation Tool): Validated, preferred. Assesses:
- Facial expression (0-2)
- Body movements (0-2)
- Muscle tension (0-2)
- Compliance with ventilator (0-2)
- Total score 0-8; score ≥3 = significant pain
- BPS (Behavioral Pain Scale): Facial expression + upper limb movements + compliance with ventilation; score 3-12
- NRS-Visual Analogue Scale for patients who can point but not speak
PART 4: ANALGESIA-FIRST STRATEGY (ANALGOSEDATION)
Current Standard: Analgesia before Sedation
- Analgesia-First Sedation: An opioid is used BEFORE adding a sedative to reach sedation target
- Analgesia-Based Sedation: Opioid ALONE is used instead of a sedative to reach sedation goal (no additional hypnotic drug)
- Reduces total sedative use
- Shorter ventilator duration
- Faster extubation
- Reduced delirium risk
Analgesic Agents in the ICU
Opioids (First-line analgesia)
| Drug | Key Features | ICU Dosing | Considerations |
|---|---|---|---|
| Fentanyl | Rapid onset, short duration, no histamine release, hepatic metabolism | 25-50 mcg IVP q1h PRN; infusion 25-200 mcg/hr | Preferred in hemodynamic instability, renal failure; lipophilic - accumulates with prolonged use |
| Morphine | Low lipid solubility, slow onset | 2-4 mg IVP q2-4h PRN | Active metabolite (M6G) accumulates in renal failure; avoid in renal impairment; histamine release |
| Hydromorphone | 5-7x more potent than morphine | 0.2-0.6 mg IVP q2-4h PRN | Metabolite accumulation in renal failure - use cautiously |
| Remifentanil | Ultra-short acting (T½ 3-10 min), ester hydrolysis by plasma/tissue esterases | Infusion 0.05-0.2 mcg/kg/min | Predictable offset ideal for neuro assessment; expensive; tachyphylaxis; requires coadministered sedative |
Non-Opioid Analgesics (Opioid-Sparing - Multimodal Analgesia)
| Drug | Mechanism | ICU Role | Notes |
|---|---|---|---|
| Acetaminophen (Paracetamol) | COX inhibition (CNS), endocannabinoid modulation | Scheduled 650-1000 mg q6h IV/PO/PR | Safe, opioid-sparing; avoid >4 g/day; reduce dose in hepatic failure |
| Ketamine | NMDA receptor antagonist | 0.1-0.5 mg/kg/hr infusion; 0.1-0.3 mg/kg IVP for procedures | Opioid-sparing; bronchodilator; dissociative; preserves airway reflexes; may cause dysphoria/hallucinations; contraindicated in raised ICP (relative) |
| Gabapentin/Pregabalin | α2δ calcium channel subunit; neuropathic analgesia | 100-300 mg TID-QID PO | Reduces opioid use; sedation side effect; dose reduce in renal failure |
| NSAIDs (Ibuprofen, Ketorolac) | COX-1/COX-2 inhibition | Short-course, adjuvant | Avoid in renal impairment, GI bleeding risk, post-cardiac surgery; reduce opioid by ~30% |
| Lidocaine IV | Sodium channel block; anti-inflammatory | 1-1.5 mg/kg/hr infusion | Reduces opioid needs, especially post-abdominal surgery; monitor for toxicity |
| Regional/neuraxial | Epidural, nerve blocks | Post-op, trauma, rib fractures | Highly effective opioid-sparing; limited by coagulopathy, patient positioning |
PART 5: SEDATION IN THE ICU
Target Sedation Level: LIGHT SEDATION is the goal
Sedation Assessment Scales
Richmond Agitation-Sedation Scale (RASS) - Most widely used
| Score | Term | Description |
|---|---|---|
| +4 | Combative | Overtly combative, violent, immediate danger to staff |
| +3 | Very agitated | Pulls/removes tubes, aggressive |
| +2 | Agitated | Frequent non-purposeful movement, fights ventilator |
| +1 | Restless | Anxious, non-aggressive movements |
| 0 | Alert and calm | Normal |
| -1 | Drowsy | Not fully alert; >10 sec eye opening to voice |
| -2 | Light sedation | Briefly awakens (<10 sec) to voice; eye contact |
| -3 | Moderate sedation | Any eye movement to voice, no eye contact |
| -4 | Deep sedation | No response to voice; any movement to physical stimulation |
| -5 | Unarousable | No response to voice or physical stimulation |
Riker Sedation-Agitation Scale (SAS): 7-point scale; target SAS 3-4
Ramsay Sedation Scale (older): 6 levels; less granular for agitation
Sedative Agents
Non-Benzodiazepines (Preferred - PADIS 2018 and 2025)
| Drug | Mechanism | Dose | Advantages | Disadvantages |
|---|---|---|---|---|
| Propofol | GABA-A receptor agonist, NMDA antagonism | 5-50 mcg/kg/min infusion (start low) | Rapid onset/offset; easy titration; anticonvulsant; antiemetic; bronchodilator | Hypotension, bradycardia, hypertriglyceridemia; PRIS (see below); no analgesia; expensive; lipid vehicle (1.1 kcal/mL - account in TPN) |
| Dexmedetomidine | Selective α2-adrenoceptor agonist (locus coeruleus) | Loading 0.5-1 mcg/kg over 10 min (often omitted); infusion 0.1-1 mcg/kg/hr | Provides sedation WITHOUT respiratory depression; analgesic-sparing (>50% opioid reduction); patients arousable/cooperative; reduces delirium vs lorazepam; facilitates extubation weaning; hemodynamic stability | Bradycardia, hypotension; costly; FDA approved for ≤24h (but safe long-term in studies); SPICE III warning (see below); no amnesia |
"We suggest using dexmedetomidine over propofol for sedation in mechanically ventilated adult patients where light sedation and/or a reduction in delirium are highest priorities." (Conditional recommendation; moderate certainty)
Propofol-Related Infusion Syndrome (PRIS) - High-Yield
- Dose >4 mg/kg/hr (>67 mcg/kg/min)
- Duration >48 hours
- High-carbohydrate, low-fat diet (or total PN)
- Children (especially with respiratory tract infections)
- Catecholamine/glucocorticoid infusions
- Metabolic acidosis (lactic acidosis - high anion gap)
- Rhabdomyolysis
- Myoglobinuria → acute kidney injury
- Lipaemia (hypertriglyceridaemia)
- Cardiac arrhythmias - new RBBB, ST changes, Brugada-like pattern
- Hepatomegaly
- Muscle necrosis
Benzodiazepines (Avoid where possible - PADIS 2018/2025)
| Drug | Key Features | Notes |
|---|---|---|
| Midazolam | Short-acting, active metabolite (1-OH-midazolam); water-soluble → lipophilic in blood | Accumulates with prolonged infusion; metabolite accumulates in renal failure; tachyphylaxis; delirium-promoting |
| Lorazepam | No active metabolites; propylene glycol vehicle | Propylene glycol toxicity with high-dose infusions (osmolar gap, metabolic acidosis, AKI) |
| Diazepam | Very long T½ (20-100h); active metabolites | Not suitable for infusion; IV bolus for acute agitation or alcohol withdrawal |
- Alcohol withdrawal (CIWA protocol; benzodiazepines are first-line)
- Seizures / status epilepticus
- Acute agitation where rapid sedation is needed
- Benzodiazepine or barbiturate withdrawal
- Specific procedures (cardioversion - midazolam)
- Patients with severe ARDS where deep sedation is required
PART 6: SEDATION STRATEGIES
1. Daily Sedation Interruption (Sedation Vacation / SAT)
- Discontinue all sedative infusions once daily at a fixed time
- Re-evaluate neurological status
- Restart at HALF the previous dose if needed (prevents re-accumulation)
- Pairing SAT + SBT (spontaneous breathing trial) = synergistic benefit
- Contraindications to SAT: Active seizures, severe ARDS, elevated ICP, therapeutic paralysis, severe alcohol withdrawal, active hemodynamic instability
2. Protocol-Driven Sedation
- Nurse-driven sedation titration algorithms targeting RASS goal set by physician
- Superior to physician-directed ad hoc dosing
- Reduces total sedative dose and duration of ventilation
3. Target-Based Sedation
- Set daily RASS target (usually -1 to 0)
- Reassess and adjust every 2-4 hours
- Always ask: "Does this patient still need sedation today?"
4. Analgosedation (Analgesia-Based Sedation)
- Treat pain first (opioid/non-opioid)
- Add sedative only if pain control alone is insufficient
- Achieves sedation target with lower sedative doses
PART 7: DELIRIUM IN THE ICU
Definition
Types
| Type | Feature | Prognosis |
|---|---|---|
| Hyperactive | Agitated, pulling lines, combative | Easily identified; better outcomes |
| Hypoactive | Quiet, withdrawn, "just sleeping" | Most common; most missed; worse outcomes |
| Mixed | Fluctuates between both | Most common overall |
Assessment Tools
- Feature 1: Acute onset + fluctuating course
- Feature 2: Inattention
- Feature 3: Altered level of consciousness
- Feature 4: Disorganized thinking
- CAM-ICU POSITIVE = Features 1+2, AND either 3 or 4
Delirium Risk Factors (Predisposing + Precipitating)
Prevention (PADIS 2018 - Primarily Non-Pharmacologic)
- Early mobilization (most important single intervention)
- Reorientation (clocks, calendars, natural light, familiar objects)
- Hearing aids and eyeglasses
- Family presence and communication
- Sleep promotion (day/night cycle, cluster care, ear plugs, eye masks)
- Remove precipitants (catheters, restraints, unnecessary drugs)
Treatment of Established Delirium
- Haloperidol: 0.25-1 mg IV/PO q8-12h. Monitor QTc. Avoid in Parkinson's disease (worsens symptoms)
- Quetiapine: 25-100 mg PO BID. Less extrapyramidal effects
- Dexmedetomidine: Preferred for hyperactive delirium in intubated patients; provides sedation while allowing communication
PART 8: SLEEP DISRUPTION IN THE ICU
- Melatonin 3-10 mg at night
- Ramelteon (melatonin agonist) 8 mg: Shows promise in reducing delirium incidence
PART 9: NEUROMUSCULAR BLOCKADE (NMB) IN ICU
- Severe ARDS (PaO2/FiO2 <150) - to improve oxygenation, reduce ventilator asynchrony (ACURASYS trial: 48h cisatracurium improved 28-day mortality - BUT ROSE trial 2019 showed no mortality benefit with routine NMB; guideline now more selective)
- Refractory intracranial hypertension
- Life-threatening ventilator asynchrony
- Status epilepticus refractory to medical therapy
- Tetanus, malignant hyperthermia
- Cisatracurium (preferred): Hoffman elimination; not affected by renal/hepatic failure; less histamine release
- Vecuronium: Hepatic metabolism; intermediate duration
- Atracurium: Hoffman + ester hydrolysis; active metabolite laudanosine (CNS stimulant)
- Rocuronium: Reversible with sugammadex; used in RSI, not prolonged infusion typically
PART 10: SPECIAL SCENARIOS
Alcohol Withdrawal (CIWA-Ar Protocol)
- Benzodiazepines ARE first-line (exception to general ICU rule)
- Lorazepam 2-4 mg IV q1-4h symptom-triggered
- CIWA-Ar score ≥8-10: Initiate treatment
- Phenobarbital as adjunct for refractory withdrawal
- Thiamine 500 mg IV TDS before glucose (prevent Wernicke's)
- Dexmedetomidine as adjunct to reduce agitation (not monotherapy)
Post-Cardiac Surgery ICU
- Propofol infusion standard for short-term sedation post-CABG
- Target extubation within 4-6 hours (fast-track cardiac surgery)
- Dexmedetomidine useful for weaning phase
Traumatic Brain Injury (TBI)
- Sedation needed to control ICP
- Propofol: preferred (reduces CMRO2, ICP; easy to interrupt for neuro assessment)
- Dexmedetomidine: useful in mild-moderate TBI
- Avoid ketamine (relative CI in raised ICP - older recommendation, increasingly challenged)
- Fentanyl preferred opioid (no histamine release, no seizure potential)
- Target CPP >60 mmHg; avoid hypotension
Sepsis
- Analgosedation preferred; minimize benzodiazepines
- Dexmedetomidine or propofol for sedation
- Note SPICE III caution with early dexmedetomidine in non-operative patients ≤65 years
PART 11: DRUG SUMMARY TABLE
| Drug | Class | Target | Dose | Key Advantage | Key Risk |
|---|---|---|---|---|---|
| Fentanyl | Opioid | Analgesia | 25-200 mcg/hr | Hemodynamically stable | Accumulation |
| Morphine | Opioid | Analgesia | 2-4 mg q2-4h | Cheap, effective | Renal failure, histamine |
| Ketamine | NMDA antagonist | Analgesia/sedation | 0.1-0.5 mg/kg/hr | Opioid-sparing, bronchodilator | Dysphoria, secretions |
| Paracetamol | Non-opioid | Analgesia adjunct | 1g q6h IV | Safe, scheduled opioid-sparing | Hepatotoxicity in overdose |
| Propofol | GABA agonist | Light-moderate sedation | 5-50 mcg/kg/min | Rapid offset, neuro exam | PRIS, hypotension |
| Dexmedetomidine | α2 agonist | Light sedation | 0.1-1 mcg/kg/hr | No resp depression, anti-delirium | Bradycardia, SPICE III caution |
| Midazolam | Benzodiazepine | Sedation/procedures | 1-5 mg IVP; 0.02-0.1 mg/kg/hr | Amnesia, anticonvulsant | Delirium, accumulation |
| Lorazepam | Benzodiazepine | Alcohol withdrawal, seizures | 0.02-0.06 mg/kg q2-6h | No active metabolites | Propylene glycol toxicity |
| Haloperidol | Antipsychotic | Hyperactive delirium | 0.5-2 mg IV/PO q8-12h | Reduces hyperactive symptoms | QTc prolongation, EPS |
| Cisatracurium | NMB | ARDS, ventilator sync | 0.1-0.2 mg/kg/hr | Organ-independent metabolism | Requires adequate sedation/analgesia |
| Melatonin | Chrono-agent | Sleep/delirium prevention | 3-10 mg nocte | New 2025 PADIS recommendation | Minimal side effects |
NEET SS CRITICAL CARE MCQs: SEDATION & ANALGESIA
- A) Midazolam
- B) Lorazepam
- C) Dexmedetomidine
- D) Ketamine
- A) RASS -4 to -5 (deep sedation)
- B) RASS -2 to -3 (moderate sedation)
- C) RASS -1 to 0 (light sedation)
- D) RASS 0 to +1 (alert to restless)
- A) Deep sedation - reduce doses
- B) Significant pain requiring analgesic intervention
- C) Delirium - start haloperidol
- D) Adequate pain control - continue current regime
- A) Sepsis-related cardiomyopathy
- B) Pulmonary embolism
- C) Propofol Infusion Syndrome (PRIS)
- D) Hypertriglyceridemia from TPN
- A) Blood gas monitoring and ventilator settings
- B) Both spontaneous awakening trial AND spontaneous breathing trial
- C) Benzodiazepine avoidance
- D) Brain function monitoring (EEG)
- A) Early mobilization
- B) Reorientation strategies
- C) Haloperidol, atypical antipsychotics, dexmedetomidine (as prophylaxis)
- D) Sleep hygiene protocols
- A) Morphine
- B) Hydromorphone
- C) Fentanyl
- D) Codeine
- A) Elderly patients >75 years admitted post-cardiac surgery
- B) Mechanically ventilated patients ≤65 years admitted for non-operative reasons
- C) All septic patients regardless of age
- D) Patients with TBI admitted to neuro-ICU
- A) Acute onset + disorganized thinking alone
- B) Features 1 (acute onset + fluctuating course) + Feature 2 (inattention), AND either Feature 3 (altered consciousness) OR Feature 4 (disorganized thinking)
- C) All 4 features must be present
- D) Any 2 of 4 features
- A) Dexmedetomidine infusion
- B) Propofol infusion
- C) Lorazepam or diazepam (benzodiazepines)
- D) Haloperidol
- A) GABA-A receptor agonism
- B) NMDA receptor antagonism
- C) Selective α2-adrenoceptor agonism at locus coeruleus - produces natural NREM-like sleep
- D) Mu-opioid receptor partial agonism
- A) Zolpidem 10 mg at bedtime
- B) Propofol nocturnal infusions for sleep induction
- C) Melatonin administration
- D) Low-dose quetiapine
- A) Hyperactive delirium (agitated, combative)
- B) Hypoactive delirium (quiet, withdrawn, "just sleeping")
- C) Mixed delirium
- D) Subsyndromal delirium
- A) Should be administered routinely to all ARDS patients
- B) Is reserved for severe ARDS patients not responding to other lung-protective ventilation strategies
- C) Should not be used in ARDS under any circumstance
- D) Should be first-line before trying other ventilator strategies
- A) Gabapentin
- B) Ketamine
- C) Ketorolac
- D) Lidocaine infusion
- A) 0.5 kcal/mL
- B) 1.1 kcal/mL (from 10% lipid emulsion vehicle)
- C) 2.0 kcal/mL
- D) No caloric contribution
RAPID REVISION SUMMARY
| Concept | Key Point |
|---|---|
| PADIS framework | Pain → Agitation → Delirium → Immobility → Sleep |
| Analgesia first | Treat pain BEFORE adding sedative |
| RASS target | -1 to 0 (light sedation) for most patients |
| CPOT ≥3 | Significant pain → treat |
| CAM-ICU | Feature 1+2 + (3 or 4) = delirium positive |
| Preferred sedative 2025 | Dexmedetomidine > propofol > benzodiazepines |
| PRIS | >4 mg/kg/hr propofol >48h → lactic acidosis + rhabdomyolysis + arrhythmia |
| SPICE III caution | Dexmedetomidine ↑ mortality in non-operative patients ≤65y |
| Benzos still needed | Alcohol withdrawal, status epilepticus, acute agitation |
| Daily SAT + SBT | Pair together → shorter ventilation, less ICU stay |
| Delirium treatment | No recommendation for antipsychotics (2025); non-pharmacologic first |
| New 2025 additions | Dexmedetomidine > propofol; melatonin for sleep; anxiety as new topic; enhanced mobility |
| NMB in ARDS | Not routine; reserve for severe ARDS not responding to other measures |
- Miller's Anesthesia, 10e (Dexmedetomidine ICU use, SPICE III, PADIS guidelines)
- Fischer's Mastery of Surgery, 8e (ABCDEF bundle, delirium prevention)
- Sabiston Textbook of Surgery (PRIS, opioid pharmacology, ICU pain)
- SCCM PADIS Guidelines 2018 (Devlin JW et al., Crit Care Med 2018;46(9):e825-e873)
- SCCM PADIS 2025 Focused Update (Lewis K et al., Crit Care Med 2025;53(3):e711-e727)
- PROPPR Trial | CRASH-2 Trial | SPICE III Trial | ROSE Trial
Discuss the , Assessment and Management of Pain in a Critically Ill Adult Patient with Chest Drains and Ryle's Tube Feeding for MD Anesthesia exam. Also with the possible neet ss critical care questions.
pain management chest drain ICU critically ill multimodal analgesia PADIS guidelines 2023 2024
"chest drain" OR "chest tube" AND "pain" AND "ICU" OR "critical care"
pain assessment chest drain Ryle's tube critically ill ICU BPS CPOT multimodal analgesia intercostal block 2024
chest tube pain management serratus plane block intercostal nerve block regional analgesia ICU 2023 2024
ASSESSMENT AND MANAGEMENT OF PAIN IN A CRITICALLY ILL ADULT PATIENT WITH CHEST DRAINS AND RYLE'S TUBE FEEDING
MD Anaesthesia Exam | NEET SS Critical Care
CLINICAL SCENARIO OVERVIEW
- Intubated/mechanically ventilated OR spontaneously breathing but obtunded
- Intercostal chest drain (ICD) in situ (for pneumothorax, haemothorax, pleural effusion, or post-thoracic/cardiac surgery)
- Ryle's tube (nasogastric tube) in situ for enteral nutrition
- In ICU for ≥48 hours
PART 1: WHY PAIN MATTERS - CONSEQUENCES OF UNDERTREATED PAIN
Physiological Stress Response
| System | Effect |
|---|---|
| Cardiovascular | Tachycardia, hypertension, increased myocardial oxygen demand → risk of ischaemia |
| Respiratory | Splinting of chest wall (especially with ICD) → inadequate tidal volumes, atelectasis, hypoxaemia, retained secretions, pneumonia, prolonged ventilation |
| Endocrine/Metabolic | Cortisol, catecholamine surge → hyperglycaemia, protein catabolism, immunosuppression |
| Coagulation | Hypercoagulable state → DVT/PE risk |
| GI | Decreased gut motility → ileus, impaired enteral feeding absorption via Ryle's tube |
| Neurological | Delirium (pain is a precipitant), anxiety, PTSD, post-ICU cognitive impairment |
| Wound healing | Impaired due to vasoconstriction and immunosuppression |
Consequences Specifically With Chest Drain
- Splinting: Patient guards the ICD site → inadequate deep breathing → atelectasis → V/Q mismatch → hypoxaemia → longer ventilation
- Inability to cough: Retained secretions → nosocomial pneumonia
- Agitation: Pulls at ICD → dislodgement risk
With Ryle's Tube
- NGT causes nasopharyngeal and oropharyngeal discomfort/pain
- Gastric distension from feeding (if poorly tolerated) → abdominal pain
- Aspiration risk if agitated/coughing due to pain → aspiration pneumonia
- Pain → reduced gastric motility → feed intolerance → inadequate nutrition
PART 2: SOURCES OF PAIN IN THIS PATIENT
Chronic Background (Resting) Pain
- Primary illness - injury, surgery, sepsis-related tissue damage
- ICD site - continuous pleural irritation by tube against parietal pleura, pressure on intercostal nerve/vessels
- Ryle's tube - nasopharyngeal pressure, oropharyngeal irritation, pharyngeal reflex stimulation
- Immobilisation pain - pressure areas, joint stiffness
- ETT - tracheal/laryngeal discomfort (if intubated)
- IV access sites, arterial lines, urinary catheter
Procedural (Breakthrough) Pain - HIGHEST INTENSITY
| Rank | Procedure | Pain Intensity |
|---|---|---|
| 1 | Chest tube/drain removal | Highest |
| 2 | Wound drain removal | Very high |
| 3 | Arterial line insertion | High |
| 4 | Turning/repositioning | High |
| 5 | Wound dressing change | High |
| 6 | Endotracheal suctioning | Moderate-high |
| 7 | NGT insertion | Moderate |
| 8 | Femoral catheter removal | Moderate |
ICD-Specific Pain Sources
- Insertion: Intercostal nerve trauma, periosteal trauma
- In situ: Continuous irritation of parietal pleura (highly sensitive), tube movement with respiration
- During drainage: Lung expansion causing pleural friction
- Manipulation: Stripping/milking of tube (now discouraged)
- Clamping for transport or drainage assessment
- Removal: Acute procedural pain spike
Ryle's Tube-Specific Discomfort
- Insertion: Severe nasopharyngeal pain, gag reflex activation, oesophageal/laryngeal irritation
- In situ: Persistent nasopharyngeal pressure → mucosal erosion (sinusitis, otitis media with prolonged use)
- Tube misplacement → aspiration → respiratory pain
- Feeding-related: Bloating, cramping if high rate or osmotic load
PART 3: BARRIERS TO PAIN ASSESSMENT IN THE CRITICALLY ILL
- Communication barrier: Intubated patients cannot self-report verbally
- Sedation: May mask pain behaviours without treating pain - "sedation ≠ analgesia"
- Paralysis (NMB): Completely abolishes behavioural signs - assume pain present
- Delirium: Distorts pain expression and interpretation
- Cultural/language differences
- Cognitive impairment (prior dementia, encephalopathy)
- Confounding vital signs: Tachycardia and hypertension may be from sepsis, hypovolaemia, or catecholamines - not just pain
- Provider knowledge gaps: Misconception that a sedated patient is comfortable
- Fear of analgesic side effects (respiratory depression, hypotension)
PART 4: PAIN ASSESSMENT - VALIDATED TOOLS
Step 1: Attempt Self-Report (Verbal Patients)
- "Rate your pain from 0-10" (0 = no pain, 10 = worst imaginable)
- Can be adapted: written scale, visual scale (patient points)
- Most valid when patient can communicate
Step 2: Behavioural Scales (Non-Verbal / Intubated Patients)
CPOT - Critical Care Pain Observation Tool (Recommended by PADIS)
| Domain | 0 | 1 | 2 |
|---|---|---|---|
| Facial expression | Relaxed | Tense (brow lowering, orbit tightening) | Grimacing (all above + eyes tightly closed) |
| Body movements | Absence of movements | Protection (slow, cautious movements) | Restlessness/agitation (pulling at tubes, trying to sit up) |
| Muscle tension (passive flexion/extension of arm) | Relaxed, no resistance | Tense, rigid (resistance) | Very tense/rigid (strong resistance, unable to complete) |
| Compliance with ventilator (intubated) | Tolerating ventilator | Coughing, alarms occasionally | Fighting ventilator |
| OR: Vocalization (extubated) | Talking in normal tone | Sighing, moaning | Crying out, sobbing |
- Score ≥3 = significant pain requiring intervention
- Validated in mechanically ventilated adults; recommended by PADIS 2018
- Superior to BPS in specificity (assesses muscle tension)
BPS - Behavioral Pain Scale
| Domain | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|
| Facial expression | Relaxed | Partially tightened | Fully tightened | Grimacing |
| Upper limb movements | No movement | Partially bent | Fully bent with finger flexion | Permanently retracted |
| Compliance with ventilation | Tolerating movement | Coughing but tolerating | Fighting ventilator | Unable to control ventilation |
- Score ≥5 = significant pain
- Validated, widely used
- Simpler than CPOT; less specific
FACES Pain Scale (Wong-Baker)
- Visual analogue using facial expressions
- For patients who can see and point but not speak
- Score 4-10 = significant pain
Step 3: Surrogate Pain Indicators (Supporting evidence only, NOT primary assessment)
- Sudden tachycardia or hypertension during a procedure
- Diaphoresis, mydriasis, lacrimation
- BUT: these are non-specific - consider other causes first
Step 4: Family Input
Step 5: Assume Pain is Present
- For patients who cannot self-report AND have no visible behaviours (deeply sedated, paralysed):
- Assume pain is present for known painful conditions (ICD, post-surgery, trauma)
- Treat empirically
PART 5: ASSESSMENT FREQUENCY
| Timing | Frequency |
|---|---|
| Routine background assessment | Every 4 hours minimum |
| Before and after procedures (ICD manipulation, repositioning, suctioning) | 30 min pre-procedure + 1 hour post |
| After analgesic intervention | Within 30-60 minutes |
| During weaning/extubation (chest drain still in situ) | Continuous clinical observation |
PART 6: MANAGEMENT PRINCIPLES - THE PADIS FRAMEWORK
Key Principle: "A" of ABCDEF Bundle
- Treat pain BEFORE adding sedation (Analgesia-first/Analgosedation)
- Use validated assessment tools to guide treatment, not vital signs alone
- Protocol-based stepwise approach (not ad hoc)
- Multimodal analgesia - combine drugs with different mechanisms to reduce opioid burden
- Differentiate background pain from procedural pain - different strategies needed
PART 7: PHARMACOLOGICAL MANAGEMENT
A. Background (Continuous) Pain Management
Step 1: Non-Opioid Analgesics (First-line adjuncts)
| Drug | Dose | Mechanism | Notes |
|---|---|---|---|
| Paracetamol (IV/PO/PR/via NGT) | 1 g q6h IV or via Ryle's tube | COX inhibition (CNS), endocannabinoid modulation | Gold standard non-opioid; scheduled around the clock; safe; opioid-sparing 20-30%; can be administered via NGT in liquid form; max 4 g/day; dose reduce in liver failure |
| Ibuprofen / Ketorolac (IV/PO) | Ketorolac 15-30 mg q6h IV (max 5 days) | COX-1/COX-2 inhibition; anti-inflammatory | Opioid-sparing ~30%; avoid in renal impairment, GI bleeding, post-cardiac surgery, coagulopathy; short-term only |
| Gabapentin / Pregabalin (via NGT) | Gabapentin 100-300 mg TID; Pregabalin 25-75 mg BD | α2δ calcium channel; neuropathic | Reduces opioid requirements; particularly useful for neuropathic component (ICD intercostal nerve trauma); administered crushed via Ryle's tube; dose adjust in renal failure |
| Ketamine (IV infusion) | 0.1-0.5 mg/kg/hr | NMDA antagonist | Opioid-sparing; excellent for chest/thoracic pain; bronchodilator (useful in ICD patients with respiratory compromise); no respiratory depression; can reduce splinting |
Step 2: Opioids (Mainstay for moderate-severe pain)
| Opioid | Dose | Key Advantage for this Patient | Cautions |
|---|---|---|---|
| Fentanyl | 25-50 mcg IVP PRN q1-2h; infusion 25-200 mcg/hr | Haemodynamically stable; no histamine (avoids bronchospasm in chest drain patients); renal safe | Accumulates with prolonged use; lipophilic |
| Morphine | 2-4 mg IV q2-4h PRN | Cheap; effective | Active metabolite M6G → respiratory depression and sedation in renal failure; histamine release → bronchoconstriction (caution in chest drain patients with airway disease) |
| Hydromorphone | 0.2-0.4 mg IV q2-4h | 5-7x morphine potency; less histamine | Accumulates in renal failure; constipation |
| Tramadol (via NGT) | 50-100 mg q6-8h | Dual action: weak mu agonist + SNRI; can give via Ryle's tube | Seizure risk; serotonin syndrome risk; not for severe pain |
| Remifentanil | 0.05-0.2 mcg/kg/min infusion | Ultra-short T½ (3-10 min); ideal for neuro assessment; predictable offset | Tachyphylaxis with prolonged use; must co-administer another analgesic or use scheduled nonopioid to prevent pain surges |
- Oral morphine solution, tramadol solution, liquid paracetamol, gabapentin capsules (opened into liquid) - all can be given via NGT
- Check tube position before administration (auscultation + aspiration of gastric contents + pH test; X-ray confirmation for new NGT)
- Hold tube feeding 30-60 min before and after crushed/dissolved oral medications with enteric coating or those affected by food
B. Procedural Pain Management (ICD-Specific)
For ICD Manipulation / In-Situ Care:
- IV opioid (PADIS 2018, Conditional, Moderate QoE): Fentanyl 1-1.5 mcg/kg IV 15-30 min prior to manipulation
- Ketamine: 0.3-0.5 mg/kg IV slow bolus - excellent for procedural pain (short, predictable)
- Local anaesthetic infiltration at ICD site: Lidocaine 1-2% at the insertion site + along tube tract for dressing changes
For ICD Removal:
- Opioid IV: Suggested at lowest effective dose (Conditional, Moderate QoE)
- NSAID IV/oral/rectal: Suggested as alternative to opioid (Conditional, Low QoE)
- Cold (cryotherapy): Suggested - cold pack applied to removal site (Conditional, Low QoE)
- Relaxation techniques: Suggested (breathing exercises, music therapy, distraction) (Conditional, Very Low QoE)
- Local anaesthetic infiltration (subcutaneous around ICD site): NOT specifically recommended due to low evidence, but widely used clinically
- Nitrous oxide (50% N2O/O2): NOT recommended by PADIS 2018 for chest tube removal - Low QoE
- Topical NSAID gel (diclofenac): NOT recommended - insufficient evidence
Regional Anaesthesia for Chest Drain Pain (Current Evidence):
| Block | Coverage | ICU Suitability | Notes |
|---|---|---|---|
| Intercostal Nerve Block (ICNB) | Single to multiple dermatomes | Good; can be done at bedside | Multiple injections needed (at least 2 levels above + 2 below ICD); bupivacaine 0.25-0.5%, 3-5 mL/level; blocks lateral and anterior cutaneous branches; risk of pneumothorax (relatively contraindicated with existing pneumothorax unless ICD is functional) |
| Serratus Anterior Plane Block (SAPB) | T3-T9 lateral cutaneous intercostal nerves; thoracodorsal, long thoracic nerves | Excellent for ICU - safe with anticoagulation, supine positioning, no pneumothorax risk | US-guided; covers ICD drainage site (T4-8 lateral); single injection; continuous catheter possible; opioid-sparing ~40% vs standard care (Vandenbrande 2024) |
| Erector Spinae Plane Block (ESPB) | T3-L1 (spreads to paravertebral space); dorsal + ventral rami | Good; safe with anticoagulation | Posterior approach; variable spread; covers posterior and lateral chest wall; 20-30 mL ropivacaine 0.375%; useful for rib fractures and post-thoracotomy ICD pain |
| Paravertebral Block (PVB) | Multiple thoracic levels (ipsilateral) | Moderate - needs prone/seated position | Gold standard for unilateral chest pain; risk of pneumothorax, epidural spread, hypotension; continuous catheter excellent for prolonged ICD analgesia |
| Thoracic Epidural Analgesia (TEA) | T1-T12 bilateral | Difficult in ICU; coagulopathy risk | Gold standard for bilateral or post-thoracotomy pain; contraindicated in coagulopathy, bacteraemia; requires T4-8 level for ICD coverage; excellent opioid-sparing |
| Intrapleural Analgesia | Ipsilateral pleura | Possible via existing ICD | Bupivacaine instilled via ICD; unreliable absorption; risk if ICD blocked; limited evidence |
- SAPB provides lateral cutaneous intercostal nerve coverage - directly relevant to ICD pain (lateral chest wall)
- Continuous SAPB shown comparable to IV fentanyl for rib-fracture pain with superior early mobilization and shorter ICU stay
- SAPB + ESPB combination provides better anterior and posterior coverage
C. Ryle's Tube-Specific Pain Management
| Source | Intervention |
|---|---|
| NGT insertion pain | Topical lignocaine gel (4%) to nostril; ice chips/cold water to numb pharynx; use smallest appropriate tube (14-16 Fr); lubricate well; distract with swallowing |
| In-situ nasopharyngeal discomfort | Good oral hygiene; nasal care (saline drops); reposition tube externally; use soft NGT; consider PEG (percutaneous endoscopic gastrostomy) if long-term feeding anticipated |
| Sinusitis pain from NGT | Nasal decongestants; early removal of NGT if not needed; consider orogastric tube alternative |
| Feed-related abdominal distension | Prokinetics (metoclopramide 10 mg IV q8h; erythromycin 3 mg/kg IV q6h); reduce infusion rate; semi-recumbent position 30-45°; check residuals q4h |
- Always verify placement before each drug administration
- Flush with 30 mL water before and after each drug
- Crush tablets only if appropriate (NOT modified-release or enteric-coated)
- Use liquid formulations where available
- Optimal drugs via NGT: Paracetamol (Calpol suspension), tramadol drops/liquid, gabapentin capsule contents, pregabalin capsule contents in water
PART 8: NON-PHARMACOLOGICAL PAIN MANAGEMENT
| Intervention | Evidence | Application |
|---|---|---|
| Cold therapy (cryotherapy) | Conditional recommendation, Low QoE (PADIS 2018) | Ice pack at ICD site 15 min before/after procedures; reduces inflammation and nociceptor sensitivity |
| Repositioning | Routine nursing care | Avoid prolonged pressure on ICD site; padded positioning devices |
| Music therapy | Low QoE | Reduces pain perception during procedures; reduces anxiety |
| Relaxation/breathing techniques | Very Low QoE | Guided breathing; reduces procedural pain via distraction + relaxation |
| Family presence | Reduces anxiety | Calming effect during procedures reduces pain perception |
| Communication | Always | Explaining procedures reduces anticipatory anxiety and pain |
| Minimise unnecessary procedures | Best practice | Every ICD manipulation, suctioning episode causes pain - minimise |
| Early mobilization | PADIS 2018 (E of bundle) | Reduces pain from immobilisation; reduces delirium; requires adequate analgesia first |
PART 9: STEPWISE PROTOCOL - PRACTICAL APPROACH
1. ASSESS: Use CPOT or BPS every 4 hours and pre/post procedure
CPOT ≥3 or BPS ≥5 = TREAT
2. ASSUME: If paralysed/unresponsive with known painful condition (ICD, post-surgery) → TREAT
3. BACKGROUND PAIN:
→ Paracetamol 1g IV/NGT q6h (SCHEDULED, not PRN)
→ + Fentanyl infusion 25-100 mcg/hr (titrate to CPOT <3)
→ + Gabapentin 100-300 mg TID via NGT (if neuropathic component)
→ ± Regional block (SAPB / ESPB / intercostal) for ICD
4. BREAKTHROUGH PAIN (CPOT ≥3 despite background):
→ Fentanyl 25-50 mcg IV bolus PRN q1h
→ Reassess in 30 min
5. PRE-PROCEDURAL (ICD manipulation, removal, repositioning):
→ Plan 30 min ahead
→ Fentanyl 1-1.5 mcg/kg IV OR Ketamine 0.3 mg/kg IV
→ + Non-pharmacologic: cold pack, patient preparation
→ Reassess CPOT 1 hour post-procedure
6. REASSESS DAILY: Is the ICD still needed? Is NGT still needed?
Early removal = major pain reduction strategy
7. MONITOR: Respiratory depression (RR, SpO2), delirium (CAM-ICU)
PART 10: MONITORING FOR ANALGESIC SIDE EFFECTS
| Drug | Key Monitoring |
|---|---|
| Opioids | RR, SpO2, RASS (oversedation), bowel sounds (ileus), urinary retention, naloxone ready |
| Paracetamol | LFTs weekly if prolonged; daily max dose <4g |
| NSAIDs | Creatinine, urine output, GI complaints via NGT, PT/INR |
| Ketamine | HR, BP (ketamine raises both), dysphoria, secretions |
| Gabapentin/Pregabalin | Sedation score, RR (especially with opioids) |
| Regional blocks | Systemic LA toxicity signs (LAST), infection at catheter site, coagulopathy |
| NGT drugs | Gastric residual volume (if NGT feed), tube position checks |
PART 11: SPECIAL CONSIDERATIONS
Renal Impairment (Common in ICU)
- Avoid morphine (M6G accumulates - prolonged respiratory depression)
- Fentanyl preferred (hepatic metabolism to inactive metabolites)
- Reduce gabapentin/pregabalin dose (renally excreted)
- Avoid ketorolac/NSAIDs (nephrotoxic)
- Paracetamol safe at standard doses
Hepatic Impairment
- Reduce paracetamol (max 2g/day in severe hepatic impairment)
- Fentanyl/morphine increased T½ with cirrhosis - monitor carefully
- Midazolam prolonged sedation - avoid
Haemodynamic Instability
- Fentanyl IV preferred over morphine (less histamine/hypotension)
- Ketamine useful (maintains BP and HR)
- Avoid epidural if haemodynamically unstable (sympathetic block worsens hypotension)
- SAPB/ESPB safe (minimal haemodynamic effect)
Coagulopathy
- Avoid epidural and paravertebral blocks (haematoma risk)
- SAPB, ESPB safe (distant from neuraxis, compressible sites)
- NSAIDs worsen coagulopathy - avoid
Respiratory Failure / Mechanical Ventilation
- Opioids: Titrate carefully to avoid over-suppression; use analgosedation
- Regional blocks (SAPB/ESPB) allow opioid reduction → less respiratory depression → faster weaning
- ICD drainage for pneumothorax/effusion improves respiratory mechanics → reduces pain from respiratory effort
Post-Extubation with ICD Still In Situ
- Critical period - patient now more aware of ICD discomfort
- Multimodal oral/NGT analgesia becomes primary
- Regional block or intercostal nerve block very useful
- Incentive spirometry only feasible with adequate analgesia
- Poor pain control post-extubation → splinting → re-intubation risk
PART 12: SUMMARY TABLE - PAIN MANAGEMENT MATRIX
| Pain Source | Assessment Tool | Background Rx | Procedural Rx | Regional Option |
|---|---|---|---|---|
| ICD in situ | CPOT/BPS | Paracetamol + Fentanyl ± Gabapentin | Fentanyl/Ketamine IV bolus; cold pack | SAPB, ESPB, ICNB, PVB, Epidural |
| ICD removal | CPOT + pain report | Pre-existing analgesic | Opioid IV + cold therapy + relaxation; NOT topical LA gel, NOT N2O | Single-shot ICNB |
| ICD manipulation | CPOT/BPS | Same as above | Fentanyl 1-1.5 mcg/kg pre-procedure | Local infiltration |
| NGT in situ | Patient report (if able) | Oral care, tube positioning | Topical LA gel for insertion; prokinetics for distension | N/A |
| Immobilisation pain | CPOT/NRS | Paracetamol; repositioning schedule | Pre-repositioning opioid | N/A |
| Primary illness/surgical | CPOT/NRS | Multimodal analgesic ladder | Procedure-specific pre-analgesia | Epidural/PVB if applicable |
NEET SS CRITICAL CARE MCQs
- A) Ramsay Scale
- B) BPS (Behavioral Pain Scale)
- C) CPOT (Critical Care Pain Observation Tool)
- D) NRS (Numerical Rating Scale)
- A) Endotracheal suction
- B) Nasogastric tube insertion
- C) Chest tube/drain removal
- D) Arterial line insertion
- A) IV opioid at lowest effective dose
- B) Cold therapy/cryotherapy
- C) Relaxation techniques
- D) Nitrous oxide (50% N₂O/O₂)
- A) Increase propofol infusion rate
- B) Administer IV fentanyl 25-50 mcg as per pain protocol
- C) Perform CAM-ICU to rule out delirium
- D) Check chest X-ray for ICD position
- A) Morphine (IV infusion)
- B) Hydromorphone (IV infusion)
- C) Fentanyl (IV infusion)
- D) Codeine (via NGT)
- A) Thoracic epidural analgesia
- B) Paravertebral block
- C) Serratus Anterior Plane Block (SAPB)
- D) Intercostal nerve block with intrathoracic injection
- A) Administer drug → flush tube → check position → resume feeding
- B) Check tube position → hold feeding → flush 30 mL water → administer drug → flush 30 mL water → resume feeding
- C) Crush tablet → dissolve → flush → administer without checking position
- D) Administer drug directly without flushing - it will reach stomach anyway
- A) Tachycardia and hypertension should be the PRIMARY parameters to assess pain
- B) Vital signs should NOT be used as the primary assessment tool; use validated behavioural scales instead
- C) A heart rate >100/min always indicates uncontrolled pain in ICU
- D) Stable vital signs confirm absence of pain
- A) Morphine
- B) Gabapentin
- C) Ketamine
- D) Ketorolac
- A) No analgesia needed - patient is fully paralysed and cannot feel pain
- B) Assess with BPS/CPOT every 4 hours and treat if score elevated
- C) Assume pain is present and ensure adequate analgesia is in place; pain cannot be assessed behaviourally during NMB
- D) Use only paracetamol as opioids are contraindicated with NMB
- A) Paracetamol should be given only as rescue medication (PRN) when CPOT ≥3
- B) IV paracetamol is scheduled regularly (around the clock) as an opioid-sparing adjunct
- C) Paracetamol is contraindicated via NGT/Ryle's tube
- D) Paracetamol should not be used in ventilated patients due to hepatic risk
- A) Increase background opioid infusion to prevent all pain
- B) Maintain current background analgesic; add pre-procedural IV fentanyl 30 min before physiotherapy; consider regional block (SAPB/PVB/epidural) for cough-induced pain
- C) Administer IV diazepam before physiotherapy for anxiolysis
- D) Avoid physiotherapy until CPOT remains ≤2 at all times
- A) Pregabalin - it undergoes extensive hepatic first-pass metabolism
- B) Gabapentin - it is renally excreted unchanged; accumulates in AKI causing excessive sedation and respiratory depression
- C) Gabapentin - it inhibits CYP450 enzymes causing drug interactions
- D) Pregabalin - it causes severe hypertension in renal failure
EXAM SUMMARY CARD
| Topic | Key Point |
|---|---|
| Most painful ICU procedure | Chest tube removal (Europain Study) |
| Pain scale for intubated patients | CPOT (preferred) - includes muscle tension; BPS |
| CPOT threshold for treatment | ≥3 |
| BPS threshold for treatment | ≥5 |
| Vital signs for pain assessment | NOT recommended as primary tool (PADIS 2018) |
| PADIS on nitrous oxide for ICD removal | NOT recommended |
| PADIS on cold therapy for ICD removal | Suggested (Conditional, Low QoE) |
| Best opioid in renal failure | Fentanyl |
| Regional block safe in coagulopathy | SAPB, ESPB (NOT epidural/PVB) |
| Paracetamol scheduling | ATC (scheduled q6h), NOT PRN only |
| NGT drug rule | Check position → flush 30 mL → drug → flush 30 mL |
| NMB patient pain management | Assume pain present; empirical analgesia; CPOT invalid |
| Ketamine advantage with ICD | Opioid-sparing + bronchodilator + haemodynamically stable |
| Analgosedation principle | Treat PAIN first; add sedative only if insufficient |
- SCCM PADIS Guidelines 2018 (Devlin JW et al., Crit Care Med 2018;46(9):e825-e873)
- Sabiston Textbook of Surgery (ICU pain, opioid pharmacology)
- Fischer's Mastery of Surgery, 8e (ABCDEF bundle, ICU delirium/pain)
- Puntillo KA et al. Determinants of procedural pain intensity in the ICU: The Europain Study. AJRCCM 2014
- Vandenbrande et al. SAPB reduces opioid consumption after minimally invasive cardiac surgery. Reg Anesth Pain Med 2024
- Non-Neuraxial Chest and Abdominal Wall Regional Anesthesia for ICU Physicians - J Clin Med 2024;13:1104
- SCCM ICU Liberation Bundle - Pain assessment tools
ECMO .INDICATIONS AND PROCEDURE OF ECMO IN CRITICALLY ILL PATIENT. FOR MD ANAESTHESIA EXAMINATION. WITH POSSIBILE NEET SS QUESTIONS
ECMO indications procedure VV VA critically ill adult ELSO guidelines 2022 2023 2024 ARDS cardiac arrest
"extracorporeal membrane oxygenation" ECMO indications critically ill adults
VA ECMO VV ECMO procedure cannulation technique complications management anticoagulation weaning 2023 2024
ECMO harlequin syndrome north south differential hypoxia North-South phenomenon management 2023
https://www.ncbi.nlm.nih.gov/books/NBK576426
EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO)
Indications and Procedure in the Critically Ill Adult
MD Anaesthesia Examination | NEET SS Critical Care
PART 1: DEFINITION AND HISTORICAL CONTEXT
- 1972: First successful adult use (Robert Bartlett)
- 2009: H1N1 influenza pandemic → major expansion of ECMO for respiratory failure (CESAR trial)
- 2018: EOLIA trial - VV ECMO for severe ARDS
- 2020-2022: COVID-19 → exponential global expansion
- 2023 ELSO guidelines updated; ATS 2024, ESICM 2023: formal updated recommendations
PART 2: COMPONENTS OF THE ECMO CIRCUIT
Patient → Drainage Cannula (venous) → Centrifugal Pump →
Membrane Oxygenator → Return Cannula (arterial/venous) → Patient
Key Components:
| Component | Function | Details |
|---|---|---|
| Drainage/Access Cannula | Removes deoxygenated blood from patient | Large bore (21-25 Fr); multi-stage drainage holes |
| Centrifugal Pump | Provides non-pulsatile flow (1-7 L/min) | Generates negative pressure up to -100 mmHg; replaces roller pump (less haemolysis) |
| Membrane Oxygenator | Gas exchange (O2 addition, CO2 removal) | Hollow-fibre polypropylene membrane; surface area 1.8-2.0 m²; separate sweep gas line |
| Heat exchanger | Maintains patient normothermia | Prevents circuit-induced hypothermia |
| Return/Reinfusion Cannula | Returns oxygenated blood to patient | Arterial (VA ECMO) or venous (VV ECMO); 15-21 Fr |
| Tubing + connectors | Circuit integrity | Heparin-coated to reduce thrombogenicity |
| Flow meter, pressure monitors | Safety monitoring | Pre/post-oxygenator pressures; circuit flow |
| Sweep gas (FiO2, flow rate) | Controls gas exchange | Sweep flow controls CO2 removal; FiO2 controls oxygenation |
PART 3: TYPES OF ECMO
A. Venovenous ECMO (VV ECMO) - Respiratory Support Only
- Bifemoral VV: Drainage from femoral vein → Return to internal jugular vein (most common)
- Single-site dual-lumen cannula (Avalon/Crescent): Single cannula via right internal jugular vein - drainage from IVC + SVC, return directed at tricuspid valve. Preferred in awake ECMO
- Return cannula tip must point toward tricuspid valve (echocardiographic guidance essential)
B. Venoarterial ECMO (VA ECMO) - Cardiac + Respiratory Support
| Route | Drainage | Return | Notes |
|---|---|---|---|
| Peripheral femoro-femoral | Femoral vein → RA | Femoral artery → aorta (retrograde) | Most common; bedside; percutaneous; risk of limb ischaemia |
| Central (via sternotomy) | Right atrium | Ascending aorta (antegrade) | Post-cardiac surgery; better upper body oxygenation; higher bleeding risk |
| Femoro-axillary/subclavian | Femoral vein | Axillary/subclavian artery | Antegrade flow; avoids limb ischaemia; allows ambulation |
C. Venoarteriovenous ECMO (VAV ECMO)
- Hybrid configuration: Drainage from femoral vein; return to BOTH femoral artery (VA) AND right internal jugular vein (VV)
- Indication: VV ECMO insufficient oxygenation + cardiac dysfunction (or Harlequin syndrome management)
PART 4: INDICATIONS
A. VV ECMO Indications (Respiratory Failure)
| Criterion | Threshold |
|---|---|
| Severe hypoxaemia | PaO₂/FiO₂ <80 mmHg after optimal management including prone positioning (if no CI) |
| Hypercapnic respiratory failure | pH <7.25 despite RR 35/min + Pplat ≤30 cmH₂O |
| Air leak syndrome | Severe (barotrauma/volutrauma preventing adequate ventilation) |
| Murray Lung Injury Score | ≥3 (despite 6-12h of optimal management) |
| Bridge indications | Lung transplant candidate; bridge to recovery while awaiting transplant |
- CESAR Trial (2009): Transfer to ECMO centre → improved survival without severe disability (63% vs 47%)
- EOLIA Trial (2018): VV ECMO for severe ARDS - 60-day mortality 35% ECMO vs 46% conventional (not statistically significant, but 28% ECMO crossover rate)
- PRONECMO Trial (2023): Prone positioning during VV ECMO - safe and feasible; no difference in 60-day ECMO-free survival
- Severe ARDS (PF ratio <80 after prone, optimal PEEP, neuromuscular blockade)
- H1N1/COVID-19/viral pneumonitis with refractory hypoxaemia
- Severe hypercapnia - post-obstructive (asthma, COPD exacerbation) with respiratory acidosis
- Bridge to lung transplantation
- Primary graft dysfunction post-lung transplant
- Pulmonary haemorrhage/massive aspiration where lung-protective ventilation cannot be achieved
B. VA ECMO Indications (Cardiac/Cardiorespiratory Failure)
| Indication | Notes |
|---|---|
| Cardiogenic shock (CS) | Post-AMI, acute myocarditis, acute decompensated HF; evidence growing (EURO SHOCK Trial 2024) |
| Post-cardiotomy shock | Failure to wean from CPB after cardiac surgery - most common VA ECMO indication historically |
| Refractory ventricular arrhythmias | VF/VT storms not responsive to antiarrhythmics; bridge to ablation |
| Acute myocarditis | Particularly fulminant myocarditis; high chance of recovery |
| Acute massive PE | Bridge to thrombolysis, catheter-directed therapy, or surgical embolectomy |
| Drug overdose/toxin | Severe cardiodepression (beta-blocker, CCB toxicity, local anaesthetic toxicity) |
| Hypothermic cardiac arrest | "Not dead until warm and dead" - rewarming via ECMO |
| Refractory cardiac arrest (ECPR) | In-hospital or out-of-hospital; Class IIa AHA 2023 |
| Bi-ventricular failure | Not amenable to LVAD alone |
| Bridge to VAD/transplant | Destination therapy staging |
| Procedural support | High-risk PCI, electrophysiology ablation |
- VA ECMO initiated during active cardiac arrest
- AHA 2023: Class IIa when equipment and trained personnel available, refractory to standard ACLS
- Assessment after ~10 min of unsuccessful conventional CPR
- Candidates: Young, witnessed arrest, reversible cause, short no-flow time, potentially recoverable
- Reversible causes: AMI, PE, refractory VF, hypothermia, drug toxicity, myocarditis
- 2024 NIS analysis: Each 12-hour delay in VA ECMO initiation increases adjusted in-hospital mortality by 6%
PART 5: CONTRAINDICATIONS
Absolute Contraindications
- Irrecoverable condition without bridge plan (no destination therapy - futility)
- Advanced directive refusing ECMO/resuscitation
- Uncontrolled haemorrhage not amenable to surgical control (relative to heparinisation)
- Severe aortic regurgitation (VA ECMO increases afterload → worsens AR)
- Aortic dissection (unless specific plan for repair)
Relative Contraindications (Centre-dependent decisions)
| Factor | Concern |
|---|---|
| Mechanical ventilation >7 days (VV ECMO) | Irreversible lung injury; low chance recovery |
| Age extremes (especially BMI >45) | Increased mortality; difficult cannulation |
| Severe neurological injury (irreversible) | No meaningful recovery |
| Immunosuppression/active malignancy (life expectancy <5 years) | Allocation resource |
| Uncontrolled sepsis/septicaemia | Bacteraemia + circuit = increased risk; relative |
| Chronic respiratory failure on O₂/NIPPV | Non-acute; low recovery chance |
| SAPS-II score >90 | Very high mortality prediction |
| Severe coagulopathy not correctable | Haemorrhagic complications |
| Decision to limit life-sustaining treatment | Ethical grounds |
PART 6: PROCEDURE - STEP-BY-STEP
Pre-ECMO Preparation
- ECMO physician (intensivist/cardiac surgeon/perfusionist)
- Bedside nurse (ECMO-trained)
- Perfusionist
- Vascular surgeon (for surgical cutdown if needed)
- Echocardiographer
- ECMO circuit primed and de-aired (crystalloid/blood prime)
- Centrifugal pump tested
- Membrane oxygenator inspected
- Correct cannula sizes chosen (based on patient weight/BSA - usually 21-25 Fr drainage, 15-21 Fr return)
- Emergency medications: Heparin, vasopressors, emergency drugs
- Imaging: Fluoroscopy OR bedside ultrasound
- ABG, CBC, coagulation (PT, aPTT, fibrinogen, TEG/ROTEM)
- Echo (LV/RV function, valve assessment, thrombus, pericardial effusion)
- CT angiography (vascular anatomy, femoral vessel assessment if time permits)
- 12-lead ECG, CXR
- Blood group and crossmatch
- Baseline ACT (Activated Clotting Time)
VV ECMO Cannulation Procedure (Bifemoral)
- Supine; sedation + analgesia (RASS -2 to -3)
- Sterile draping of groin and neck
- USS-guided or fluoroscopic guidance
- Seldinger technique: Needle → guidewire → serial dilators → 21-25 Fr multi-stage drainage cannula
- Advance to right atrium/IVC junction (tip at RA-IVC junction ~2 cm above diaphragm)
- Confirm position by X-ray/echo
- Right IJV approached in standard fashion (USS-guided)
- 15-21 Fr return cannula advanced to SVC-RA junction
- Echo guidance to confirm tip position near tricuspid valve
- Connect drainage cannula → pump inlet
- Connect return cannula → oxygenator outlet
- Ensure no air in circuit (de-air check)
- Start pump at low flow (1-2 L/min)
- Administer heparin bolus 50-100 units/kg IV
- Gradually increase flow to target (3-5 L/min or 60-80 mL/kg/min)
- Target: SaO₂ >88-92%, ETCO₂ reduced, acidosis correcting
VA ECMO Cannulation Procedure (Femoro-Femoral)
- USS-guided femoral vein puncture (10-15 cm below inguinal ligament)
- 21-25 Fr multi-stage drainage cannula → IVC → right atrium
- Confirm by X-ray/TOE: tip at RA-IVC junction
- USS-guided common femoral artery puncture
- CRITICAL: Document and protect distal perfusion - insert 6-8 Fr antegrade perfusion cannula (downflow cannula) into superficial femoral artery to prevent ipsilateral limb ischaemia
- 15-21 Fr arterial return cannula advanced to common iliac artery (NOT beyond aorto-iliac junction to avoid renal/mesenteric ischaemia)
- As above: heparin bolus → connect → start at low flow → gradually increase
- Fluoroscopy or TOE (transesophageal echo) for VA ECMO
- Assess LV for distension (if non-ejecting LV on VA ECMO)
- Maintain MAP 60-80 mmHg
- Vasopressors titrated as needed
- Initial flow ~50% predicted cardiac output, titrate up
Dual-Lumen Single Cannula (Avalon/Crescent) - VV ECMO
- Right IJV approach
- Single 31 Fr (female) or 27 Fr (male) dual-lumen cannula
- Drainage ports at SVC and IVC (draws from both)
- Return port directed toward tricuspid valve
- Must confirm direction of return port by TOE - critical to avoid recirculation
- Benefits: Single site; enables patient mobilisation; "awake ECMO"
PART 7: ECMO MANAGEMENT
Initial Targets
| Parameter | VV ECMO Target | VA ECMO Target |
|---|---|---|
| ECMO flow | 3-5 L/min (60-80 mL/kg/min) | 2-4 L/min (sufficient to maintain MAP >60) |
| SaO₂ (patient) | >88-92% | >90-95% |
| SvO₂ (venous saturation) | 70-85% | >70% |
| MAP | Conventional targets | 60-80 mmHg |
| PaCO₂ | Controlled by sweep gas flow | 35-45 mmHg |
| ACT (anticoagulation) | 180-220 sec | 180-220 sec |
| Anti-Xa | 0.3-0.7 IU/mL | 0.3-0.5 IU/mL |
| Hb | >10 g/dL | >10 g/dL (higher threshold) |
Protective Ventilation on ECMO ("Ultra-Protective")
- Tidal volume: 3-4 mL/kg PBW (lower than standard 6 mL/kg)
- PEEP: 10-15 cmH₂O
- FiO₂: 0.3-0.4 (allow lung rest)
- RR: 10-15/min
- Plateau pressure: <25 cmH₂O
- Driving pressure: <15 cmH₂O
Anticoagulation
- Heparin infusion (standard): Continuous unfractionated heparin (UFH) targeting ACT 180-220 sec OR anti-Xa 0.3-0.7 IU/mL
- Monitoring: ACT q4h; aPTT; anti-Xa levels; TEG/ROTEM for comprehensive assessment
- Heparin resistance: Use antithrombin III (AT-III) concentrate or fresh frozen plasma
- Heparin-induced thrombocytopenia (HIT): Switch to argatroban or bivalirudin
- Bleeding: Reduce or hold heparin; transfuse platelets, FFP, cryoprecipitate
Haemodynamic Management on VA ECMO
- Vasopressors to maintain MAP >60 mmHg
- LV venting strategies to prevent pulmonary oedema if LV not ejecting:
- Intra-aortic balloon pump (IABP) - first-line LV unloading
- Impella device - more aggressive LV decompression
- Atrial septostomy (for severe LV distension)
- Inotropes may reduce LV distension by improving native ejection
PART 8: COMPLICATIONS
A. Circuit Complications
| Complication | Cause | Management |
|---|---|---|
| Oxygenator failure | Plasma leak, clot, protein deposition | Circuit change; check sweep gas; pressure monitoring |
| Pump failure | Mechanical failure, air | Manual backup; circuit change |
| Clot in circuit | Inadequate anticoagulation | Increase heparin; partial/full circuit change |
| Air embolism | High negative pressure (-100 mmHg) from centrifugal pump | Clamp circuit; de-air; never infuse air into drainage limb |
| Circuit rupture | Tubing breach | Clamp immediately; circuit replacement |
B. Patient Complications
1. Bleeding (Most Common - 17-34% incidence)
- Sites: Cannulation sites, intracranial, GI, pulmonary
- Cause: Systemic anticoagulation + acquired von Willebrand factor deficiency + platelet dysfunction from pump + thrombocytopenia
- Management: Reduce/hold heparin; FFP, platelets, cryoprecipitate, factor VIIa (with caution - fatal thrombosis risk); consider tranexamic acid in life-threatening haemorrhage
2. Thromboembolism
- Systemic thromboembolism more common in VA ECMO
- Intracardiac thrombus: stasis in non-ejecting LV → clot → arterial embolism
- Management: Vigilant ACT monitoring; LV venting to improve LV ejection
3. Limb Ischaemia (VA ECMO - femoral cannulation)
- Retrograde arterial flow diverts blood from distal limb
- Prevention: Antegrade distal perfusion cannula (downflow cannula) into superficial femoral artery - inserted at time of primary arterial cannulation
- Monitoring: Near-infrared spectroscopy (NIRS) on lower limb, hourly pulse assessment
- Management: Fasciotomy for compartment syndrome; surgical thrombectomy
4. Neurological Complications (~7% VV, higher in VA)
- Ischemic stroke (thromboembolic)
- Intracranial haemorrhage (anticoagulation + hypertension)
- Hypoxic-ischaemic brain injury
- Management: Tight BP control (avoid SBP >140); reduce anticoagulation if haemorrhagic; neurology consultation
5. HARLEQUIN SYNDROME / NORTH-SOUTH SYNDROME (VA ECMO - CRITICAL EXAM TOPIC)
- Peripheral VA ECMO returns oxygenated blood retrograde via femoral artery → reaches aorto-iliac bifurcation
- As LV function recovers, native cardiac output begins ejecting deoxygenated blood (since lungs still impaired) FORWARD into aortic arch
- Watershed zone where native (deoxygenated) and ECMO (oxygenated) blood meet moves cranially as cardiac output improves
- Result: Cerebral and coronary circulation perfused by native desaturated blood; lower body perfused by oxygenated ECMO blood
- Right radial artery SpO₂/SaO₂ significantly lower than femoral artery SpO₂/SaO₂
- Right radial is critical monitoring site in all femoro-femoral VA ECMO patients
- Tolerate if patient improving and cardiac recovery evident
- Fix the lung: Optimise ventilator (↑FiO₂/PEEP), recruitment, prone, bronchoscopy, diuresis, NO
- Increase ECMO sweep gas FiO₂ → increases oxygenation of ECMO blood
- Increase ECMO flow rate (to push watershed point more cranially)
- Add VV component → VAV ECMO: Add venous return cannula via right IJV to deliver oxygenated blood to RV → perfuses lungs → native cardiac output becomes oxygenated
- Change to central VA ECMO (antegrade flow from ascending aorta)
6. Left Ventricular Distension (VA ECMO)
- ECMO increases afterload → LV cannot eject against increased resistance → LV dilates → pulmonary oedema
- Assessment: Echo (LVIDD, LVOTO velocity, aortic valve opening frequency)
- Management: IABP (reduces afterload), Impella (direct LV drainage), inotropes, surgical LV venting/atrial septostomy
7. Renal Failure
- Non-pulsatile flow → reduced renal perfusion
- Haemolysis → myoglobinuria
- Management: Continuous renal replacement therapy (CRRT) in-line with ECMO circuit
8. Haemolysis
- Pump speed-related; check lactate dehydrogenase (LDH), plasma haemoglobin, haptoglobin
- High circuit pressures → haemolysis
- Management: Reduce pump speed where possible; check for circuit clots
PART 9: WEANING AND DECANNULATION
VV ECMO Weaning (Lung Recovery Assessed)
- Improved lung compliance and gas exchange on ventilator
- Oxygen delivery maintained with lower sweep gas FiO₂
- Reduce sweep gas FiO₂ to 0.21 (room air) and/or reduce sweep gas flow to near zero
- Maintain ventilator support
- If ABG acceptable (PaO₂ >70 mmHg, pH >7.35, SpO₂ >92%) on ventilator alone for 1-4 hours → proceed to decannulation
- Reduce ECMO flow gradually while maintaining sweep gas ("flow trial" vs "cap trial")
VA ECMO Weaning (Cardiac Recovery Assessed - Echo-Guided)
- LVEF >20-25% (recovering)
- Aortic valve opening with each beat
- LVOT VTI >10 cm (surrogate of stroke volume)
- Absence of LV distension
- Absent pericardial effusion/tamponade
- Decreasing vasopressor requirements
- Improving pulse pressure
- Return of HR variability
- Stable MAP on minimal support
- Reduce ECMO flow in stepwise fashion: 3L → 2L → 1.5L → 1L
- At each step: observe MAP, HR, SvO₂, echo findings
- If tolerated at 1-1.5 L/min → proceed to decannulation
- If fails: increase flow; reassess in 12-24 hours
- Improving EF on echo at 1-2 L/min ECMO
- Low lactate, stable haemodynamics
- Vasopressor dose decreasing
- Aortic valve opening regularly
Decannulation
- Femoral artery usually requires surgical repair (arteriotomy closure or patch repair) - in operating theatre under fluoroscopy
- Femoral vein: Manual pressure or suture
- Post-decannulation: Monitor limb perfusion, consider duplex USS
PART 10: MONITORING PARAMETERS ON ECMO
| Parameter | Frequency | Target |
|---|---|---|
| ACT | Every 4-6 hours | 180-220 sec |
| Anti-Xa | Daily (or q12h) | 0.3-0.7 IU/mL |
| CBC (Hb, plt, WBC) | Daily | Hb >10; Plt >100 |
| LDH, plasma Hb | Daily (haemolysis screen) | LDH <600 IU/L |
| ABG (VV: patient AND circuit) | Every 4-6 hours | Per target |
| Right radial SpO₂ (VA ECMO) | Continuous | Same as left radial (no differential) |
| Limb perfusion (VA ECMO) | Hourly nursing check | Warm, pulsatile, SpO₂ >95% |
| Echo (VA ECMO) | Daily | LV function, valve opening, no distension |
| Chest X-ray | Daily | Cannula positions, lung disease progression |
| Circuit inspection | Continuous nursing | No clot, air, kinking |
| Sweep gas parameters | Continuous | CO₂ target; adjust flow |
PART 11: SUMMARY COMPARISON TABLE
| Feature | VV ECMO | VA ECMO |
|---|---|---|
| Indication | Respiratory failure only | Cardiac failure ± respiratory |
| Cardiac support | None | Yes (2-7 L/min) |
| Haemodynamic stability required | Yes | No |
| Drainage cannula | Femoral vein or IJV | Femoral vein or RA (central) |
| Return cannula | IJV or femoral vein (to RA) | Femoral artery or ascending aorta |
| Flow direction | Venous → Venous | Venous → Arterial (retrograde) |
| LV unloading | Not needed | Often needed (IABP/Impella) |
| Harlequin syndrome | No | Yes (femoro-femoral) |
| Limb ischaemia | No | Yes (distal perfusion cannula needed) |
| Anticoagulation | Heparin (ACT 180-220) | Heparin (ACT 180-220) |
| Survival (ELSO registry) | ~60% to hospital discharge | ~40% to hospital discharge |
| Key monitoring | SaO₂, ETCO₂, sweep gas | Right radial SpO₂, echo, limb perfusion |
NEET SS CRITICAL CARE MCQs: ECMO
- A) PaO₂/FiO₂ <150 with FiO₂ >0.9
- B) PaO₂/FiO₂ <80 mmHg after optimal management including prone positioning
- C) PaO₂/FiO₂ <100 with FiO₂ >0.9 and Murray score ≥3-4 after >6 hours of bailout measures
- D) SAPS-II >90
- A) It provides the best measure of ECMO circuit oxygenation
- B) It reflects upper body (cerebral/coronary) oxygenation from native cardiac output - critical for detecting Harlequin/North-South syndrome
- C) The right radial has higher accuracy than left due to dominant hand dominance
- D) Femoral artery lines are always more accurate
- A) Renal failure
- B) Limb ischaemia of the ipsilateral leg
- C) Harlequin syndrome
- D) LV distension
- A) VV provides cardiac support; VA provides only respiratory support
- B) VA provides both cardiac and respiratory support; VV provides respiratory support only
- C) Both provide equivalent haemodynamic support
- D) VV provides better oxygenation than VA ECMO
- A) Circuit failure causing loss of oxygenation
- B) Competition between retrograde oxygenated ECMO return flow and antegrade deoxygenated native cardiac output in a recovering heart with persistent lung failure
- C) Cannula malposition causing venous recirculation
- D) Systemic thromboembolism from LV thrombus
- A) Sweep gas FiO₂
- B) Pump speed
- C) Recirculation fraction (amount of oxygenated blood re-entering drainage cannula before reaching patient)
- D) Patient haemoglobin concentration alone
- A) Conversion to central VA ECMO
- B) Veno-arterio-venous (VAV) ECMO
- C) Increasing ECMO pump speed
- D) Adding a second venous drainage cannula
- A) Class I - standard of care for all witnessed arrests
- B) Class IIa - reasonable when equipment and trained personnel are available
- C) Class IIb - may be considered with very low evidence
- D) Class III - no benefit, possibly harmful
- A) Right ventricular overdistension
- B) Left ventricular distension (LV not unloading against increased afterload from ECMO)
- C) Atrial septal defect caused by ECMO flow
- D) Systemic hypertension
- A) VV ECMO significantly reduced 28-day mortality vs conventional ventilation
- B) Transfer to an ECMO-capable centre improved survival without severe disability (63% vs 47%)
- C) VV ECMO had no benefit over conventional lung-protective ventilation
- D) VV ECMO should be used as first-line therapy before prone positioning
- A) Directed toward the aorta; confirmed by CXR
- B) Directed toward the tricuspid valve; confirmed by transthoracic or transesophageal echocardiography
- C) Directed toward the SVC; confirmed by fluoroscopy only
- D) Direction does not matter as flow is bidirectional
- A) 6 mL/kg predicted body weight (standard lung-protective)
- B) 4-6 mL/kg PBW with PEEP 8-10 cmH₂O
- C) 3-4 mL/kg PBW with Pplat <25 cmH₂O and driving pressure <15 cmH₂O
- D) 8-10 mL/kg PBW to recruit lung
- A) Warfarin is the preferred anticoagulant during ECMO
- B) Unfractionated heparin (UFH) targeting ACT 180-220 sec is the standard; bivalirudin or argatroban used in HIT
- C) No anticoagulation is needed with modern heparin-coated circuits
- D) Anticoagulation is contraindicated if any bleeding occurs on ECMO
RAPID REVISION TABLE
| Key Concept | Answer |
|---|---|
| VV ECMO drainage to return | Venous → Venous (RA) |
| VA ECMO drainage to return | Venous → Arterial |
| VV ECMO haemodynamic support | None |
| VA ECMO cardiac support | Yes |
| VV ECMO PF ratio indication (ELSO) | <80 after optimal management |
| ECPR classification (AHA 2023) | Class IIa |
| Harlequin syndrome diagnosis | Right radial SpO₂ << left radial or femoral |
| Harlequin syndrome solution | Fix lung, add VAV ECMO, or central cannulation |
| Limb ischaemia prevention (VA ECMO) | Distal perfusion (antegrade) cannula into SFA |
| LV distension management | IABP, Impella, atrial septostomy |
| Standard anticoagulant | UFH targeting ACT 180-220 sec |
| Dual-lumen cannula confirmation | Echo (return port → tricuspid valve) |
| Ultra-protective ventilation | Vt 3-4 mL/kg, Pplat <25, FiO₂ 0.3 |
| Survival VA ECMO (ELSO) | ~40% |
| Survival VV ECMO (ELSO) | ~60% |
| CESAR trial finding | Transfer to ECMO centre: 63% vs 47% survival without severe disability |
| EOLIA trial finding | 60-day mortality 35% ECMO vs 46% conventional (not significant; 28% crossover) |
- Miller's Anesthesia, 10e (VA ECMO indications, ECPR, ECMO for cardiac failure)
- Barash's Clinical Anesthesia, 9e (ECPR, invasive resuscitation techniques)
- Fischer's Mastery of Surgery, 8e (VA ECMO components, cardiogenic shock)
- ELSO Guidelines for Adult VV ECMO - ASAIO Journal
- StatPearls: Extracorporeal Membrane Oxygenation in Adults
- CESAR Trial (2009) | EOLIA Trial (2018) | PRONECMO Trial (2023)
- AHA 2023 CPR Guidelines (ECPR Class IIa)
- Harlequin Syndrome in ECPELLA - PMC 2025
short note on weaning from mechanical ventilation. How will you wean a patient from mechanical ventilation in the ICU? For MD Anesthesia exam. Also, with the probable neet ss , critical care exam questions. Okay.
mechanical ventilation weaning guidelines 2022 2023 2024 SBT readiness criteria extubation failure predictors
"mechanical ventilation" weaning "spontaneous breathing trial" liberation
ATS ACCP SCCM ventilator weaning liberation guidelines 2023 2024 SBT cuff leak test NIV post-extubation
https://sccm.org/blog/breathing-easier-evolving-strategies-i…
WEANING FROM MECHANICAL VENTILATION
Short Note for MD Anaesthesia Examination | NEET SS Critical Care
DEFINITION AND TERMINOLOGY
- Failure to pass the Spontaneous Breathing Trial (SBT), OR
- Need for reintubation within 48 hours of extubation, OR
- Death within 48 hours following extubation
CLASSIFICATION OF WEANING (Boles Classification - ATS/ERS Task Force 2007)
| Category | Definition | % of patients |
|---|---|---|
| Simple weaning | First SBT successful → extubated | ~70% |
| Difficult weaning | Fails initial SBT; liberation after up to 3 SBTs or ≤7 days | ~15% |
| Prolonged weaning | Fails ≥3 SBTs or >7 days from first SBT | ~15% |
STEP 1: DAILY READINESS SCREENING (Extubation Readiness Assessment)
Clinical Criteria (STOP-BANG-like screening):
| Criterion | Threshold |
|---|---|
| Underlying cause | Resolved or significantly improved |
| Consciousness | Awake, follows commands (can assess GCS, RASS) |
| Sedation | Minimal or off (RASS -1 to 0 target) |
| Oxygenation | FiO₂ ≤ 0.5; PEEP ≤ 8 cmH₂O; SaO₂ >88% |
| Haemodynamics | Stable; no escalating vasopressors |
| Secretion management | Manageable secretions; adequate cough |
| Respiratory effort | Spontaneous breathing effort present |
| Neuromuscular | Adequate muscle strength (NIF < -25 cmH₂O is favourable) |
STEP 2: WEANING PREDICTORS / INDICES (Pre-SBT)
Rapid Shallow Breathing Index (RSBI) - Tobin Index
- Formula: RSBI = Respiratory Rate (f) ÷ Tidal Volume in litres (Vt)
- Threshold: RSBI ≤ 105 breaths/min/L → weaning likely successful
- RSBI > 105 → likely weaning failure
- Introduced by: Tobin & Yang, 1991 - New England Journal of Medicine
Other Weaning Parameters:
| Parameter | Favourable | Unfavourable |
|---|---|---|
| Negative Inspiratory Force (NIF / MIP) | < -30 cmH₂O | > -20 cmH₂O |
| Vital Capacity (VC) | ≥ 10-15 mL/kg | < 10 mL/kg |
| Tidal Volume | > 5 mL/kg | < 5 mL/kg |
| Respiratory Rate | < 25/min | > 35/min |
| Minute Ventilation (MV) | < 10 L/min | > 15 L/min |
| P0.1 (airway occlusion pressure) | < 4 cmH₂O | > 6 cmH₂O (high drive) |
| Maximum Voluntary Ventilation | > 2× MV | -- |
| RSBI | ≤ 105 | > 105 |
| VO₂ increase during T-piece | < 10% | ≥ 10% (failure predictor) |
STEP 3: THE SPONTANEOUS BREATHING TRIAL (SBT)
Methods of SBT:
| Method | Settings | Notes |
|---|---|---|
| Pressure Support (PSV) - Preferred | PS 5-8 cmH₂O + PEEP 5 cmH₂O | Overcomes ETT resistance; most physiological; recommended by ATS/ACCP as first-choice (2017) |
| T-piece | Disconnects patient from ventilator; oxygen via T-piece attachment | No PEEP; tests true unassisted breathing; higher WOB |
| CPAP | CPAP 5 cmH₂O, no PS | Less than PSV; no inspiratory assistance |
Duration of SBT:
- 30 minutes - adequate and recommended; equivalent to 120 minutes in most studies
- 120 minutes - acceptable; no additional benefit demonstrated over 30 min for simple weaning
Criteria for PASSING SBT (Extubation can proceed):
| Parameter | Pass |
|---|---|
| Respiratory rate | < 35 breaths/min |
| SpO₂ | > 90% (some use >92%) |
| Systolic BP | 90-180 mmHg; <20% change from baseline |
| Heart Rate | < 140/min; <20% change |
| Comfort | No marked anxiety, distress, or dyspnoea |
| Breathing pattern | No accessory muscle use; no paradoxical abdominal movement |
Criteria for FAILING SBT (STOP the trial immediately):
| Clinical sign | Measurement |
|---|---|
| Respiratory rate | > 35/min |
| SpO₂ | < 90% |
| SBP | > 180 or < 90 mmHg |
| HR | > 140/min or sustained >20% increase |
| Accessory muscle use | Present |
| Paradoxical breathing | Present |
| Anxiety, diaphoresis, distress | Present |
| Altered consciousness | Agitation or deterioration |
| Arrhythmia | New onset |
STEP 4: POST-SBT ASSESSMENT - CUFF LEAK TEST
When to Perform:
- Patient passes SBT but is at high risk for post-extubation stridor
Risk Factors for Post-Extubation Stridor:
- Female sex
- Prolonged intubation (>6 days)
- Larger ETT
- Repeated/traumatic intubation, agitation causing laryngeal trauma
- Previous unplanned extubation and reintubation
- High BMI
How to Perform:
- Suction oropharynx
- Deflate ETT cuff
- Occlude ETT - patient breathes around tube
- Volumetric method: Measure difference between exhaled Vt (cuff inflated) and exhaled Vt (cuff deflated) over 6 breaths
- Cuff leak volume ≥110 mL (or >12% of set Vt) = adequate leak = low stridor risk
- Cuff leak < 110 mL = inadequate leak = positive test = higher stridor risk
Cuff Leak Test Failure Management (ATS/ACCP Guideline):
- Administer systemic corticosteroids for ≥4 hours before extubation
- Methylprednisolone 20 mg q4h (×4 doses) OR dexamethasone 8 mg - reduces post-extubation stridor and reintubation rate
- No need to repeat cuff leak test after steroid administration (ATS/ACCP)
- Extubate with staff and equipment ready for emergency reintubation
STEP 5: EXTUBATION PROCEDURE
Pre-Extubation Preparation:
- Explain procedure to patient
- NPO status ensured (or at least 30 min post-feed for NG tube patients)
- Position: Head of bed 30-45°
- Suction oropharynx and ETT thoroughly
- Pre-oxygenate with FiO₂ 1.0 for 3-5 minutes
- Have at bedside: bag-valve-mask, laryngoscope, ETT, succinylcholine/rocuronium, crash trolley, NIV/HFNC ready
Extubation Steps:
- Deflate ETT cuff
- Remove securing tape
- Ask patient to take deep breath (or apply positive pressure)
- Remove ETT on PEAK of inspiration (maximises glottic opening)
- Immediately apply face mask oxygen
- Encourage deep breathing and cough
- Monitor closely for 30-60 min post-extubation
STEP 6: POST-EXTUBATION MANAGEMENT
High-Risk Features for Post-Extubation Failure:
| Risk Factor |
|---|
| Age > 65 years |
| CHF (congestive heart failure) |
| COPD |
| APACHE-II > 12 |
| BMI > 30 |
| Significant secretions |
| > 2 medical comorbidities |
| > 7 days on mechanical ventilation |
Post-Extubation Oxygen Support Strategy:
| Scenario | Recommendation |
|---|---|
| Low risk | Conventional O₂ (facemask/NC) |
| High risk for extubation failure | Preventive NIV (ATS/ACCP 2017 - strong conditional recommendation) OR HFNC (non-inferior to NIV, easier to use) |
| Hypoxaemia on low FiO₂ (PF >300, no hypercapnia) | High Flow Nasal Cannula (HFNC) preferred over conventional O₂; reduces reintubation in non-hypercapnic high-risk patients (FLORALI trial) |
| Hypercapnic/COPD/obese | NIV (BiPAP) preferred; reduces reintubation in hypercapnic patients |
| Therapeutic NIV (signs of failure after extubation) | NIV for early re-emerging respiratory distress (before actual need for reintubation) |
STEP 7: PROLONGED WEANING STRATEGIES
Causes of Prolonged Weaning (7 Ps):
| Cause | Assessment |
|---|---|
| Pulmonary disease unresolved | Repeat CXR, ABG, bronchoscopy |
| Pump failure (respiratory muscle weakness) | Diaphragm ultrasound, NIF, MIP |
| Psychological (anxiety, fear) | CAM-ICU, assess PTSD; consider psychology input |
| Pump (cardiac failure) | Echo; diuresis trial; treat pulmonary oedema |
| Problem with secretions | Physiotherapy, mucolytics, minitracheostomy |
| Polymyopathy / Polyneuropathy (ICU-acquired weakness) | EMG/NCS, grip strength; rehabilitation |
| Post-extubation obstruction | Cuff leak test; airway assessment |
Strategies for Prolonged Weaning:
-
Tracheostomy (if >14 days anticipated)
- Reduces dead space and airway resistance
- Allows talking/eating/mobility
- Facilitates subglottic suctioning
- Early tracheostomy (within 4 days) vs late: Cochrane review shows no mortality difference, but early may reduce ICU stay
- Percutaneous dilational tracheostomy (PDT) preferred in ICU (Ciaglia blue rhino technique)
-
Gradual SBT lengthening
- Start with 5-10 min SBT
- Increase by 10 min each day if tolerating
- Aim for 2-hour SBT before extubation attempt
-
Pressure Support weaning (progressive reduction)
- Start at PS required for comfort (e.g., 20 cmH₂O)
- Reduce by 2-4 cmH₂O every 4-8 hours as tolerated
- Target PS ≤8 cmH₂O before proceeding to SBT/extubation
- Slower than T-piece weaning; less evidence it's superior
-
SIMV (Synchronized Intermittent Mandatory Ventilation)
- Reduce mandatory rate gradually (14 → 12 → 10 → 8 → 6 → 4 → 2 → 0)
- No longer recommended as primary weaning mode (Brochard trial 1994, Esteban trial 1995 showed PSV and T-piece superior; SIMV prolongs weaning)
-
Protocolised rehabilitation and early mobility
- ATS/ACCP 2017: protocolised rehabilitation directed toward early mobilisation (conditional recommendation)
- Prevents/treats ICU-acquired weakness
- Daily physiotherapy, passive/active exercises, sitting out, standing
-
Optimise nutrition
- Underfeeding: respiratory muscle wasting
- Overfeeding: ↑CO₂ production → hypercarbia → failed weaning
- Target 20-25 kcal/kg/day; protein 1.2-1.5 g/kg/day
-
Treat reversible co-morbidities
- Anaemia: Hb >8 g/dL target (some use >10 g/dL in weaning)
- Electrolytes: Mg²⁺, PO₄³⁻, K⁺ deficiencies impair respiratory muscle function
- Thyroid: screen for hypothyroidism in prolonged weaning
- CIAW: ICU-acquired weakness - treat with mobilisation, nutrition
-
Psychological support
- PADIS guidelines: manage anxiety; family presence; communication aids
- Passey-Muir valve for tracheostomy patients to facilitate communication and improve cough
-
Weaning unit/step-down centre
- For truly prolonged difficult weaning
- German S2k (2020): patient not permanently ventilator-dependent until 3 months of failed weaning attempts
DIAPHRAGM ULTRASOUND IN WEANING (MODERN TOOL)
| Parameter | Normal | Dysfunction |
|---|---|---|
| Diaphragmatic excursion (quiet) | 1.5-2.5 cm | < 1 cm (paralysis) |
| Diaphragmatic excursion (deep) | > 4 cm | -- |
| Diaphragmatic Thickening Fraction (DTF) | ≥ 20-30% | < 20% (atrophy/weakness) |
| DTF formula | (T insp - T exp) / T exp × 100 | -- |
- DTF < 29% = diaphragm dysfunction = higher weaning failure risk
- VIDD (Ventilator-Induced Diaphragm Dysfunction): occurs as early as 18-24 hours of controlled MV
- Combined cardiac/lung/diaphragm USS predicts weaning failure better than individual parameters (Song et al., Ann Intensive Care 2024)
WEANING FROM MV - ALGORITHM SUMMARY
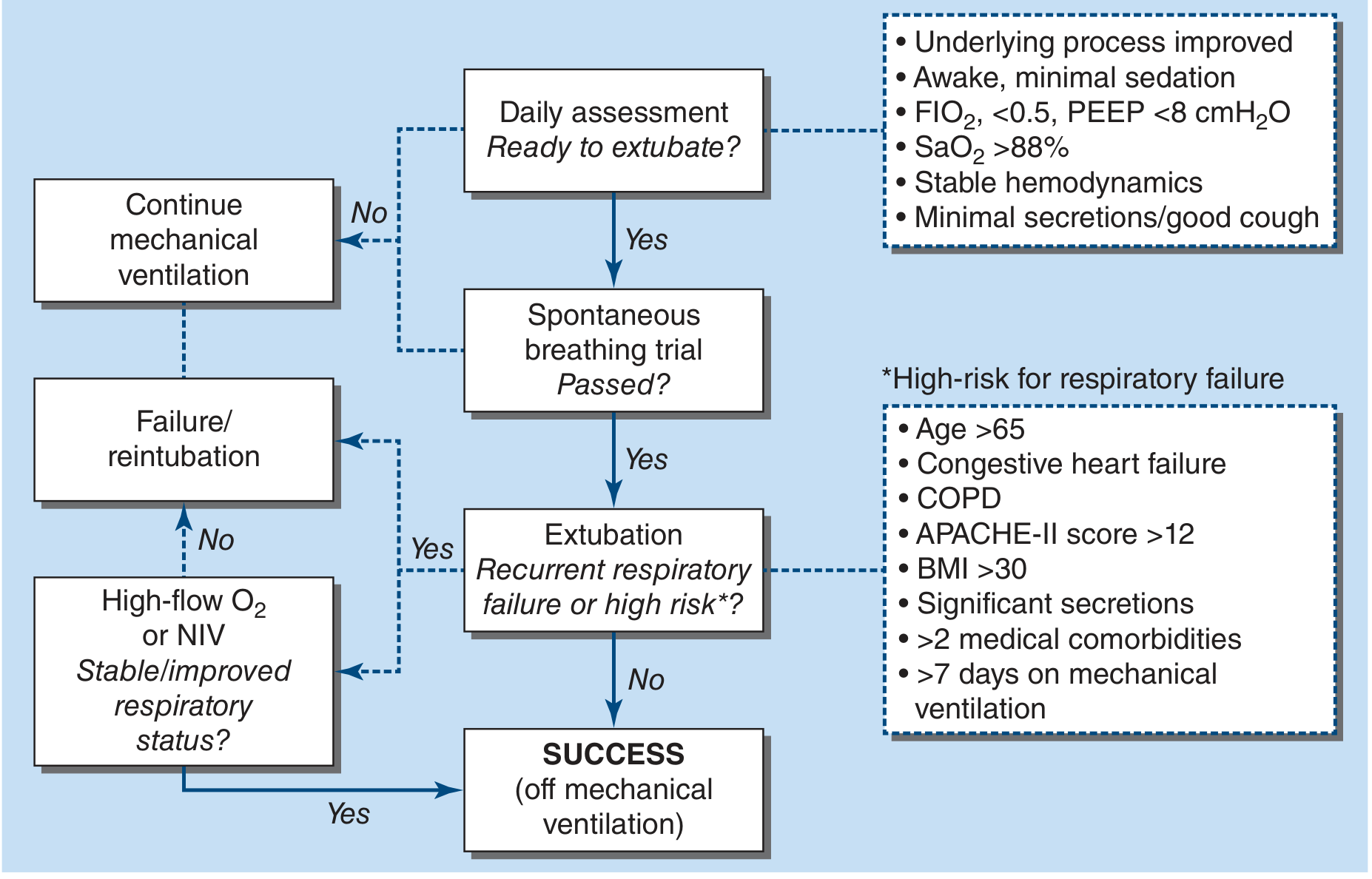
GUIDELINE SUMMARY TABLE
| Guideline | Key Recommendation |
|---|---|
| ATS/ACCP 2017 | Initial SBT with PS 5-8 cmH₂O preferred over T-piece; preventive NIV in high-risk; cuff leak test → steroids ≥4h if failed |
| AARC 2024 | RSBI no longer required before SBT; SBT before noon; FiO₂ NOT increased during SBT; SBT with or without PS both acceptable |
| SCCM PADIS 2025 | Light sedation (RASS -1 to 0); SAT + SBT daily (ABCDEF bundle); dexmedetomidine preferred |
| German S2k 2020 | Prolonged weaning defined ≥7 days; not permanently vent-dependent until 3 months |
NEET SS CRITICAL CARE MCQs: MECHANICAL VENTILATION WEANING
- A) RSBI ≤ 105 must always be confirmed before performing an SBT
- B) RSBI is no longer required to determine readiness for SBT
- C) RSBI has replaced the cuff leak test as a pre-extubation assessment
- D) RSBI ≥ 105 is the threshold for extubation readiness
- A) Conventional oxygen via face mask, monitor
- B) Immediate reintubation prophylactically
- C) Preventive NIV (BiPAP) or HFNC post-extubation
- D) Continue mechanical ventilation for another 24 hours
- A) Is no longer recommended as of 2024 guidelines
- B) Was recommended by ATS/ACCP 2017 as the preferred method for the initial SBT
- C) Is associated with significantly higher extubation failure rates
- D) Should only be used for COPD patients
- A) Perform an emergency tracheostomy
- B) Cancel extubation permanently
- C) Administer systemic steroids for ≥4 hours, then extubate with airway team present
- D) Repeat cuff leak test after 30 minutes
- A) The preferred weaning method in adults according to ATS
- B) Superior to PSV weaning in terms of weaning duration
- C) No longer recommended as primary weaning mode; shown to prolong weaning time compared to PSV or T-piece SBT
- D) Recommended for cardiac post-operative patients
- A) Sodium
- B) Chloride
- C) Phosphate (hypophosphataemia) and Magnesium
- D) Calcium
- A) Normal diaphragm function; proceed to extubation
- B) Diaphragm atrophy or dysfunction - associated with higher weaning failure risk (VIDD)
- C) Hyperinflation of the diaphragm
- D) Diaphragmatic paralysis requiring phrenic nerve stimulation
- A) Using SIMV as the weaning mode
- B) Incorporating a daily extubation readiness screening followed by SBT into a structured care protocol
- C) Administering daily nebulised bronchodilators
- D) Reducing FiO₂ by 10% each hour
- A) NIV was clearly superior to HFNC in preventing reintubation
- B) HFNC was non-inferior to NIV and superior to conventional oxygen for reducing reintubation at 72 hours
- C) T-piece SBT was the only method associated with reduced failure
- D) Extubation was contraindicated without tracheostomy
- A) After midnight to reduce staff workload during day shifts
- B) Before noon each day (AARC 2024)
- C) Only on Mondays, Wednesdays, and Fridays per protocol
- D) 6 hours after each arterial blood gas is obtained
- A) Has proven benefit when used therapeutically (rescue) for post-extubation respiratory failure
- B) Has proven benefit when used preventively in high-risk patients who passed SBT; rescue NIV for frank failure does NOT reduce reintubation or mortality
- C) Should replace standard SBT assessment
- D) Is contraindicated in COPD patients
- A) After 72-96 hours of mechanical ventilation
- B) After 18-24 hours of controlled mechanical ventilation
- C) Only after 7 days of MV
- D) After 1 month of MV
- A) T-piece SBT
- B) Pressure Support Ventilation with gradual reduction
- C) SIMV with gradual reduction of mandatory rate
- D) CPAP SBT
- A) Chest X-ray urgently
- B) Initiate NIV (CPAP)
- C) Administer IV dexamethasone 8 mg, humidified oxygen, nebulised adrenaline (1:1000, 5 mL); reintubation if not responding
- D) Perform tracheostomy at bedside
- A) A - Assess and treat pain
- B) B - Both SAT and SBT performed daily
- C) C - Choice of analgesia and sedation
- D) E - Early mobility and exercise
RAPID REVISION BOX
| Concept | Key Point |
|---|---|
| RSBI formula | f ÷ Vt(L); ≤105 = wean likely |
| RSBI 2024 update | No longer required before SBT (AARC 2024) |
| SBT timing | Before noon each day (AARC 2024) |
| SBT duration | 30 min adequate (equivalent to 120 min) |
| SBT preferred mode | PS 5-8 cmH₂O + PEEP 5 (ATS 2017); either PS or T-piece (AARC 2024) |
| SBT success → extubation success | >70% |
| Cuff leak test - failure management | Steroids ≥4h before extubation; no repeat CLT needed |
| Post-extubation high risk → | Preventive NIV/HFNC immediately |
| Rescue NIV benefit | No benefit once frank post-extubation failure develops |
| SIMV weaning | Avoid - prolongs weaning (Esteban 1995) |
| Prolonged weaning definition | >7 days from first SBT |
| VIDD onset | 18-24 hours of controlled MV |
| DTF < 20% | Diaphragm dysfunction; higher failure risk |
| SAT + SBT | Reduces MV days by 3; ICU LOS by 4 days |
| Protocolised weaning benefit | 25% fewer vent days; 10% less ICU LOS |
| Post-extubation stridor | Dexamethasone + nebulised adrenaline; reintubate if failing |
- Harrison's Principles of Internal Medicine, 22e (Fig. 313-4 algorithm, liberation criteria, high-risk features)
- ATS/ACCP 2017: Liberation from Mechanical Ventilation in Critically Ill Adults (thoracic.org)
- AARC Clinical Practice Guideline 2024: Spontaneous Breathing Trials - PMID 38443142
- SCCM 2024 blog on AARC 2024 guideline changes
- Trivedi V et al., Chest 2022 - RSBI meta-analysis - PMID 34181953
- German S2k Prolonged Weaning Guideline 2020 - PMID 33302267
Discuss the role of the Anaesthesiologist in palliative care medicine. For md anaesthesia exam qn . Also give possible neet ss critical care questions
role of anaesthesiologist palliative care medicine pain management interventional procedures terminal sedation 2023 2024
"palliative care" anaesthesiologist "pain management" interventional terminal sedation
anaesthesiologist role palliative care interventional pain WHO analgesic ladder neuraxial opioids coeliac plexus block terminal sedation ICU withdrawal
"palliative sedation" refractory symptoms terminal illness midazolam propofol
https://link.springer.com/article/10.1007/s12630-019-01482-w
"interventional pain" "palliative" celiac plexus intrathecal drug delivery cancer
ROLE OF THE ANAESTHESIOLOGIST IN PALLIATIVE CARE MEDICINE
MD Anaesthesia Examination | NEET SS Critical Care
INTRODUCTION
DOMAINS OF ANAESTHESIOLOGIST INVOLVEMENT IN PALLIATIVE CARE
1. PAIN MANAGEMENT (pharmacological)
2. INTERVENTIONAL PAIN PROCEDURES
3. PALLIATIVE/TERMINAL SEDATION
4. AIRWAY AND SYMPTOM MANAGEMENT
5. END-OF-LIFE CARE IN THE ICU
6. EDUCATION, ETHICS AND COMMUNICATION
DOMAIN 1: PHARMACOLOGICAL PAIN MANAGEMENT
A. The WHO Analgesic Ladder (Updated 3+1 Step Model)
▲ STEP 4 (Added 2018)
│ Interventional / Neuromodulation
│
▲ STEP 3
│ Strong opioids (Morphine, Oxycodone, Fentanyl, Hydromorphone)
│ ± Non-opioid ± Adjuvant
│
▲ STEP 2
│ Weak opioids (Codeine, Tramadol)
│ ± Non-opioid ± Adjuvant
│
▲ STEP 1
Non-opioids: Paracetamol, NSAIDs
± Adjuvants
- By mouth - preferred oral route
- By the clock - regular dosing, not PRN
- By the ladder - step-wise escalation
- For the individual - titrated to patient need
- Attention to detail - anticipate and treat side effects
B. Opioid Management in Palliative Care
| Drug | Route | Key Features |
|---|---|---|
| Morphine | Oral/IV/SC/epidural/intrathecal | Gold standard; active metabolites (M6G) accumulate in renal failure |
| Fentanyl | IV/TD patch/buccal/OTFC | No active metabolites; preferred in renal failure; patch (72-hourly) for stable pain |
| Oxycodone | Oral/IV | Good oral bioavailability (~60%); useful for neuropathic component |
| Hydromorphone | Oral/IV/SC/intrathecal | 5-10× potent than morphine; useful in renal failure (less accumulation than morphine) |
| Methadone | Oral | NMDA antagonist; excellent for neuropathic pain; complex pharmacokinetics; risk QT prolongation |
| Buprenorphine | TD/SL/IV | Partial agonist; ceiling effect; useful in mild-moderate; renal safe |
- Oral morphine 30 mg = IV morphine 10 mg (3:1 ratio)
- Oral morphine 30 mg = oral oxycodone 20 mg
- Oral morphine 30 mg = fentanyl patch 12.5-25 mcg/h
- Oral morphine 30 mg/day → fentanyl patch = 30/2 = 15 mcg/h (approximate)
- Oral - preferred
- Subcutaneous infusion (syringe driver) - when oral route lost; preferred over IM (painful); most palliative drugs compatible
- Transdermal - stable pain; not for acute titration
- IV PCA - for inpatients with rapid titration needs
- Neuraxial (epidural/intrathecal) - see Domain 2
C. Adjuvant Analgesics (Co-Analgesics)
| Class | Drug | Indication |
|---|---|---|
| Antidepressants (TCA) | Amitriptyline, Nortriptyline | Neuropathic/burning pain |
| Antidepressants (SNRI) | Duloxetine, Venlafaxine | Neuropathic pain; chemotherapy-induced neuropathy |
| Anticonvulsants | Gabapentin, Pregabalin | Neuropathic pain, allodynia |
| Corticosteroids | Dexamethasone | Bone pain, nerve compression, raised ICP, appetite |
| Bisphosphonates | Zoledronic acid | Bone metastases; reduces fracture risk |
| Ketamine | Low-dose oral/SC/IV | Opioid-refractory pain; NMDA antagonism; neuropathic pain |
| Lidocaine | IV infusion | Neuropathic pain, opioid-refractory |
| NSAIDS | Ketorolac, Diclofenac | Bone pain, inflammatory pain |
| Muscle relaxants | Baclofen | Spasm pain, spinal cord compression |
DOMAIN 2: INTERVENTIONAL PAIN PROCEDURES
A. Peripheral Nerve Blocks
| Block | Indication | Technique |
|---|---|---|
| Intercostal nerve block | Rib metastases, chest wall pain, post-thoracotomy | Percutaneous; USS-guided |
| Paravertebral block / ESPB | Unilateral chest/abdominal wall cancer pain | Single shot or catheter; USS-guided |
| Brachial plexus block | Upper extremity tumour pain | Continuous catheter |
| Femoral/sciatic nerve block | Lower limb tumour pain | Continuous catheter |
| Occipital nerve block | Head/neck cancer, cervicogenic headache |
B. Sympathetic and Visceral Nerve Blocks (NEUROLYTIC - Key Exam Topic)
1. Coeliac Plexus Block / Neurolysis (CPB)
- Indication: Visceral pain from upper abdominal malignancies - pancreatic cancer (most common indication), hepatobiliary cancers, gastric cancer
- Anatomy: Coeliac plexus = 2 paired ganglia, anterior to aorta, at T12-L1 level; receives sympathetic input from greater/lesser/least splanchnic nerves + parasympathetic from vagus
- Approach:
- Posterior (most common): Fluoroscopy or CT-guided bilateral posterior approach (paramedian at L1); needle tip anterior to aorta
- Anterior: Endoscopic USS-guided (EUS-CPB) - preferred in advanced pancreatic cancer (direct visualisation, anterior approach avoids aorta)
- Neurolytic agents: Absolute alcohol 50-100% (6-20 mL per side) or phenol 6-10%
- Diagnostic block first: Use LA (bupivacaine 0.5%) before neurolysis
- Evidence (Cochrane 2011): Significantly improved pain at 8 weeks + lower opioid consumption and side effects vs standard analgesia
- Complications: Transient orthostatic hypotension (sympathectomy), diarrhoea (parasympathetics unopposed), pneumothorax, intravascular injection, nerve root injury, retroperitoneal haematoma
- EUS-CPB reduces complications compared to percutaneous approach
2. Superior Hypogastric Plexus Block
- Indication: Pelvic visceral pain (cervical, bladder, prostate, rectal cancers)
- Anatomy: Pre-aortic plexus at L5-S1; bilateral sympathetic ganglia
- Approach: Posterior fluoroscopy-guided bilateral approach; anterior USS-guided
- Neurolysis: Alcohol or phenol
3. Ganglion Impar Block (Walther's Ganglion)
- Indication: Perineal/rectal pain, tailbone pain (coccydynia), anorectal and vulval cancers
- Anatomy: Single midline ganglion at sacrococcygeal junction - last ganglion of the sympathetic chain
- Approach: Transcoccygeal or paracoccygeal
4. Stellate Ganglion Block
- Indication: Upper extremity sympathetically maintained pain, Complex Regional Pain Syndrome (CRPS), some head/neck cancer pain
- Neurolysis: Generally diagnostic blocks only; neurolysis rare due to risk
5. Lumbar Sympathetic Block
- Indication: Sympathetically maintained pain in lower extremities, CRPS type 1, peripheral vascular disease-associated pain
C. Neuraxial Techniques
1. Epidural Analgesia
- Continuous infusion: Opioid (morphine/fentanyl/hydromorphone) ± LA (bupivacaine/ropivacaine) ± adjuvants (clonidine, ketamine)
- Benefits over systemic opioids: Lower doses achieve better analgesia; fewer systemic side effects
- Tunnelled epidural catheter for home/hospice use (weeks to months)
- Used for: Thoracic/abdominal/pelvic cancer pain, vertebral metastases, chest wall pain
2. Intrathecal Drug Delivery (ITDD) / Implantable Drug Delivery Systems (IDDS)
- Mechanism: Drug delivered directly to cerebrospinal fluid → directly at spinal cord receptors; 100-300× more potent than oral morphine; massive reduction in systemic doses and side effects
- Implanted pump (programmable) with intrathecal catheter to appropriate spinal level
- First-line ITDD drugs: Morphine + bupivacaine (PACC 2017 - combination recommended)
- Additional drugs: Ziconotide (N-type calcium channel blocker; non-opioid; first-line for neuropathic pain in ITDD), clonidine, hydromorphone
- Morphine oral:intrathecal ratio: ~300:1
- Indications: Cancer patients with inadequate analgesia or intolerable side effects from systemic opioids; expected survival >3 months (for implanted pump); some centres use external pump for shorter prognosis
- Evidence (Implantable Drug Delivery vs Comprehensive Medical Management trial - Smith et al., JAMA 2002): ITDD reduced pain by 52% vs 39%; significantly less toxicity; 6-month survival improved
3. Intrathecal Neurolytic Procedures
- Intrathecal alcohol/phenol block (Intrathecal neurolysis): For patients with cancer pain refractory to all other measures; may produce saddle anaesthesia and sphincter dysfunction - reserved for patients with pre-existing incontinence/colostomy
- Cervical cordotomy (Percutaneous): Interrupts spinothalamic tract at C1-2 level; used for unilateral cancer pain below C5; high success rate; life-limiting complications (Ondine's curse - loss of automatic respiration if bilateral)
D. Neuromodulation
- Spinal Cord Stimulation (SCS): Less evidence in cancer pain (historically avoided due to concern about disease progression and device interference); some centres use for neuropathic cancer pain
- Deep Brain Stimulation (DBS): Specialist centres; refractory cancer pain
- Transcutaneous Electrical Nerve Stimulation (TENS): Non-invasive adjunct; no systemic effects; useful for bone metastases, localised pain
DOMAIN 3: PALLIATIVE SEDATION (TERMINAL SEDATION)
Definition (EAPC 2023 Revised Framework):
Indications:
- Refractory symptoms unresponsive to all available palliative treatment options:
- Refractory pain
- Intractable dyspnoea
- Refractory agitated delirium
- Refractory nausea/vomiting
- Refractory existential distress (controversial - open debate)
- Patient is terminally ill with expected death in hours to days
- Exhausted all alternatives
Types:
| Type | Definition |
|---|---|
| Proportional sedation | Level of sedation proportional to the degree of suffering; light to deep |
| Intermittent sedation | Periods of sedation with periods of wakefulness; respite sedation |
| Continuous sedation | Uninterrupted sedation; only when intermittent insufficient |
| Continuous Deep Sedation (CDS) | Maintained deep unconsciousness until death; last resort |
Drug Protocol (EAPC 2023 Stepwise Approach):
- Midazolam - drug of choice; titrated SC/IV infusion; start 1-5 mg SC/hour; widely controllable
- Lorazepam - alternative; longer acting; SL/IV
- Levomepromazine (methotrimeprazine) - sedating antipsychotic; SC/IM/IV
- Chlorpromazine - alternative
- Propofol MUST be administered by an anaesthesiologist or person with equivalent expertise (EAPC 2023)
- Used when benzodiazepines + neuroleptics fail
- Continuous infusion: Start 20-50 mg/hour; titrate
- Rapid onset; easily titratable; predictable pharmacokinetics
- Risk: cardiovascular depression, apnoea - requires monitoring
Principle of Double Effect (KEY ETHICAL CONCEPT):
- The action itself is not intrinsically wrong
- The agent intends the good effect, not the harmful one
- The good effect is not produced BY the harmful effect
- There is proportionate reason for tolerating the harm
DOMAIN 4: SYMPTOM MANAGEMENT
Dyspnoea (Breathlessness)
| Intervention | Dose/Route | Rationale |
|---|---|---|
| Morphine (first-line) | 2-4 mg SC/oral q4h | Reduces ventilatory drive, reduces anxiety about breathlessness; DOES NOT hasten death when properly titrated |
| Midazolam | 2.5-5 mg SC PRN | For distress/anxiety component |
| Fan/air flow | -- | Simple non-pharmacologic; activates V2 receptors in face |
| Low-dose corticosteroids | Dexamethasone 4-8 mg/day | If airway obstruction, lymphangitis |
| Oxygen | Only if hypoxaemic (SpO₂ <90%) | Not beneficial if normoxaemic; HFNC provides comfort |
Death Rattle (Noisy Terminal Breathing / Terminal Secretions)
- Caused by pooling of oropharyngeal secretions in semi-conscious/unconscious dying patient (unable to clear)
- NOT distressing to patient (unconscious) - but distressing to family
- Management:
- Reposition patient (lateral/semi-prone)
- Anticholinergics:
- Glycopyrrolate 0.2 mg SC q4h (preferred - does NOT cross BBB, less confusion)
- Hyoscine butylbromide (Buscopan) 20 mg SC q4h
- Hyoscine hydrobromide (scopolamine) - crosses BBB, more sedating
- Do NOT attempt suction (stimulates more secretions; distressing)
Nausea and Vomiting
| Cause | Drug |
|---|---|
| Central (opioid-induced) | Haloperidol 0.5-1.5 mg SC q8-12h; metoclopramide |
| Bowel obstruction | Dexamethasone + octreotide + hyoscine; NG drainage |
| Raised ICP | Dexamethasone; positioning |
| Vestibular | Cyclizine, ondansetron |
Agitated Delirium (Terminal Restlessness)
- Very common in last 24-48 hours of life
- Pharmacological management:
- Haloperidol 0.5-2 mg SC q4-6h (first-line)
- Midazolam 2.5-5 mg SC q1h PRN (for agitation/distress)
- Levomepromazine (sedating antipsychotic) - for severe terminal agitation
DOMAIN 5: END-OF-LIFE CARE IN THE ICU
Withdrawal of Life-Sustaining Treatment (WLST)
- Autonomy: Patient's right to refuse treatment
- Non-maleficence: Avoiding futile/burdensome treatment
- Beneficence: Focusing on comfort goals
- Justice: Fair allocation of scarce resources
| Concept | Definition | Anaesthetic Relevance |
|---|---|---|
| Withholding | Not initiating a new treatment | Decision not to start dialysis, vasopressors, intubation |
| Withdrawing | Removing already-started treatment | Terminal extubation, stopping vasopressors, stopping ECMO |
| DNR/DNAR | Do-not-attempt resuscitation order | Legal document; must be clearly communicated |
| Terminal extubation | Removal of ETT from dying patient | Anaesthesiologist key role; premedicate with morphine + midazolam |
Terminal Extubation Procedure (Anaesthesiologist Leads):
- Goals-of-care discussion with family and team
- DNR order confirmed
- Consent from family/surrogate
- Discontinue monitors if family preference
- Ensure private room, family present
- Morphine 2-5 mg IV (titrate to comfort; dyspnoea anticipated post-extubation)
- Midazolam 1-2 mg IV (anxiolysis; reduces awareness of dyspnoea)
- Glycopyrrolate 0.2 mg IV (reduces secretions/death rattle)
- Start as continuous infusion (morphine 2-10 mg/h + midazolam 1-5 mg/h) via syringe driver to maintain comfort
- Turn off ventilator (or switch to CPAP then off)
- OR deflate cuff and remove ETT (direct terminal extubation)
- Remove all monitors that are not comfort-related
- Provide oxygen only if patient appears distressed
- Continue titrating opioids and benzodiazepines to comfort
- Glycopyrrolate for secretions
- Family at bedside; chaplaincy/spiritual support
- Document physician intent as symptom-directed comfort care
Advance Care Planning and Goals of Care Discussions
- Explain prognosis honestly using validated tools (APACHE II, SOFA, SAPS)
- Facilitate advance directive documentation
- Understand and implement:
- Living will - documented patient preferences
- Health care proxy / Durable Power of Attorney for Healthcare
- POLST (Physician Orders for Life-Sustaining Treatment) - India: equivalent is advance medical directive
- Futility - medical futility when treatment cannot achieve goals
- Lead family meetings using the NURSE communication framework (Naming, Understanding, Respecting, Supporting, Exploring)
DOMAIN 6: AIRWAY MANAGEMENT IN PALLIATIVE SCENARIOS
Malignant Upper Airway Obstruction
- Tumours of larynx, trachea, thyroid, neck can cause stridor and acute obstruction
- Anaesthesiologist is the essential team member for emergency airway management
- Options: Awake fibreoptic intubation, tracheostomy (surgical or percutaneous), airway stenting (interventional bronchoscopy), laser ablation under GA, high-flow oxygen as temporising
- Steroids (dexamethasone 8-16 mg IV) reduce tumour oedema acutely
- Heliox (He:O₂ 70:30) reduces turbulent airflow; temporising measure
Anaesthesia for Palliative Procedures
- Palliative radiation (e.g., for bone metastases) - may need sedation/GA for positioning
- Palliative surgical procedures (e.g., gastrostomy, biliary stenting, vertebroplasty for pathological fracture)
- Thoracocentesis, paracentesis, pericardiocentesis - anaesthesiologist provides sedation/analgesia
- Tracheostomy for malignant airway obstruction
Nutritional Access
- Insertion of PEG (Percutaneous Endoscopic Gastrostomy) under sedation by anaesthesiologist
- Central venous access (PICC, ports) for parenteral nutrition, chemotherapy delivery, medication infusion
MULTIDISCIPLINARY PALLIATIVE CARE TEAM
| Team Member | Role |
|---|---|
| Anaesthesiologist/Pain Specialist | Pharmacological pain management, interventional procedures, palliative sedation, airway management, ICU end-of-life care |
| Palliative care physician | Symptom management, prognosis, goals of care, advance directives |
| Oncologist | Disease-modifying therapy, prognosis |
| Nurse (specialised palliative) | 24h symptom monitoring, medication administration, family support |
| Physiotherapist | Mobility, breathlessness management, lymphoedema |
| Psychologist/Psychiatrist | Anxiety, depression, existential distress |
| Social worker | Family support, home care planning, financial counselling |
| Chaplain/Spiritual care | Spiritual distress |
| Pharmacist | Drug interactions, syringe driver compatibility |
SUMMARY TABLE: ANAESTHESIOLOGIST'S SPECIFIC CONTRIBUTIONS
| Area | Specific Role |
|---|---|
| WHO ladder pharmacology | Opioid prescribing, rotation, titration |
| Interventional pain | Neurolytic blocks, ITDD, SCS |
| Coeliac plexus neurolysis | Pancreatic/GI cancer pain |
| Regional anaesthesia | Continuous nerve catheters for cancer pain |
| Palliative sedation | Propofol administration (Step 3 EAPC 2023); monitoring |
| Terminal extubation | Pre-medication, procedure, post-procedure care |
| WLST | Ethical framework; ICU dying patients |
| Airway emergency | Malignant airway obstruction |
| Anaesthesia for palliative procedures | Sedation/GA for radiation, surgery, procedures |
| Goals-of-care communication | Family meetings, advance directives |
NEET SS CRITICAL CARE MCQs: PALLIATIVE CARE
- A) Lumbar sympathetic block
- B) Intrathecal pump with morphine
- C) Coeliac plexus neurolysis with absolute alcohol
- D) Thoracic epidural catheter
- A) Midazolam
- B) Haloperidol
- C) Propofol
- D) Morphine
- A) The dual mechanism of morphine on μ and κ receptors
- B) A dose of morphine having two simultaneous analgesic effects
- C) The ethical justification for administering high-dose opioids where intended effect is symptom relief even if death may be unintentionally hastened
- D) The combination of two opioids used simultaneously
- A) Performing fasciotomy for limb ischaemia
- B) Administering adequate comfort medications (morphine + midazolam) to ensure no suffering during and after ECMO discontinuation
- C) Converting to VV ECMO as a bridge
- D) Performing emergency tracheostomy
- A) 3:1
- B) 10:1
- C) 100:1
- D) 300:1
- A) Aggressive oropharyngeal suction every 30 minutes
- B) Repositioning + glycopyrrolate 0.2 mg SC q4h (preferred anticholinergic as it does NOT cross the BBB)
- C) High-dose diuretics to reduce secretions
- D) Endotracheal intubation to protect the airway
- A) CRASH-2 trial
- B) Smith et al. JAMA 2002 (Implantable Drug Delivery vs Comprehensive Medical Management)
- C) CESAR trial
- D) PROPPR trial
- A) Administer analgesics in the morning only
- B) Analgesics should be given at regular scheduled intervals to maintain constant blood levels, not just on-demand (PRN)
- C) Analgesics should be given by the fastest available route
- D) Pain should be assessed hourly using a clock-based system
- A) Rocuronium + ketamine (to prevent movement)
- B) Morphine IV + midazolam IV, with glycopyrrolate to reduce secretions; continue as infusion post-extubation
- C) Propofol bolus + sugammadex
- D) No medications; let nature take its course
- A) Upper abdominal visceral cancer pain
- B) Pelvic visceral pain from gynaecological malignancy
- C) Perineal and rectal pain, anorectal and vulval cancers
- D) Bilateral lower extremity CRPS
- A) Stop the pump immediately; naloxone IV titrated in small doses (0.04 mg aliquots)
- B) Flumazenil IV
- C) Neostigmine + glycopyrrolate
- D) Increase the pump rate to flush the drug
- A) The dose of drug administered
- B) The route of administration (IV vs oral)
- C) The intent of the physician - symptom relief (palliative sedation) vs intentional ending of life (euthanasia)
- D) Whether the patient is awake or unconscious
- A) Ketamine + clonidine
- B) Morphine + bupivacaine (combination recommended over single agent)
- C) Fentanyl alone
- D) Ziconotide + midazolam
RAPID REVISION TABLE
| Concept | Key Point |
|---|---|
| WHO ladder steps | 1: Non-opioid → 2: Weak opioid → 3: Strong opioid → 4: Interventional |
| WHO principles | By mouth, by clock, by ladder, for individual, attention to detail |
| Opioid choice in renal failure | Fentanyl or hydromorphone (not morphine - M6G accumulates) |
| Intrathecal:oral morphine ratio | 1:300 (IT 300x more potent) |
| Coeliac plexus neurolysis | Best evidence for pancreatic cancer pain; alcohol/phenol |
| Ganglion impar | Perineal/anorectal/vulval cancer pain; sacrococcygeal junction |
| Superior hypogastric plexus | Pelvic visceral cancer pain |
| EAPC 2023 palliative sedation Step 3 | Propofol - only by anaesthesiologist |
| Palliative sedation first-line | Midazolam SC/IV infusion |
| Death rattle preferred drug | Glycopyrrolate (doesn't cross BBB) |
| Terminal extubation premedication | Morphine + midazolam + glycopyrrolate |
| Double effect principle | Intent = symptom relief; distinguishes from euthanasia |
| WLST ethics | Withdrawing = withholding (ethically equivalent) |
| ITDD Smith et al. JAMA 2002 | ITDD improved pain + survival vs CMM |
| NMB at end of life | Never give alone without sedation/analgesia (constitutes euthanasia) |
- Harrison's Principles of Internal Medicine, 22e (palliative care framework)
- EAPC 2023 Revised Framework on Palliative Sedation (palliativeprojects.eu)
- Interventional Anesthesia and Palliative Care collaboration - Canadian Journal of Anaesthesia (2019)
- StatPearls: Palliative Sedation in Terminal Illness
- Smith TJ et al. JAMA 2002 - Implantable Drug Delivery vs CMM in cancer pain
- WHO Analgesic Ladder (1986, revised 2018)
- PACC 2017 Intrathecal Drug Delivery guidelines
- Cochrane 2011 - Coeliac plexus block in pancreatic cancer
Lung protective ventilation strategy. Short note on ventilator strategies in ARDS , for md anaesthesia exam . Also withpoxsible nett ss critical care questions .
ARDS ventilation strategy 2023 2024 Berlin definition prone positioning neuromuscular blockade PEEP titration driving pressure mortality
ARDS lung protective ventilation prone positioning neuromuscular blockade PEEP
ARDS prone positioning mortality benefit neuromuscular blockade ACURASYS PHARLAP dexamethasone
ATS 2024 ARDS guideline recommendations prone positioning recruitment maneuvers steroids new global definition 2023
ARDS prone positioning PROSEVA corticosteroids dexamethasone neuromuscular blockade ROSE ACURASYS
https://www.scielo.br/j/ccsci/a/Jwv53H3hsPLKtMZqmpV5yJQ?lang…
ARDS dexamethasone corticosteroids mortality benefit mechanical ventilation
LUNG PROTECTIVE VENTILATION AND VENTILATOR STRATEGIES IN ARDS
Short Note for MD Anaesthesia Examination | NEET SS Critical Care
PART 1: DEFINITION AND BACKGROUND
ARDS - Historical Evolution
| Year | Milestone |
|---|---|
| 1967 | First described by Ashbaugh et al. (Lancet) - acute respiratory distress in adults |
| 1988 | Murray Lung Injury Score (LIS) introduced |
| 1994 | AECC Definition (American-European Consensus Conference) - ALI and ARDS distinguished by PF ratio |
| 2012 | Berlin Definition (current clinical standard) |
| 2024 | New Global Definition (Matthay et al., AJRCCM 2024) - expanded to include high-flow nasal oxygen |
Berlin Definition of ARDS (2012 - EXAM STANDARD)
| Criterion | Specification |
|---|---|
| Timing | Acute onset within 1 week of clinical insult or new/worsening respiratory symptoms |
| Imaging | Bilateral opacities not fully explained by effusions, lobar/lung collapse, or nodules (CXR or CT) |
| Origin of oedema | Not fully explained by cardiac failure or fluid overload (echo to exclude if no risk factor) |
| Oxygenation | PaO₂/FiO₂ ratio with PEEP or CPAP ≥5 cmH₂O |
| Category | PaO₂/FiO₂ | Mortality |
|---|---|---|
| Mild | 200-300 mmHg | ~27% |
| Moderate | 100-200 mmHg | ~32% |
| Severe | <100 mmHg | ~45% |
New Global Definition 2024 (Matthay et al.)
- Includes non-intubated patients on high-flow nasal cannula (HFNC) with FiO₂ ≥0.3
- Includes SpO₂/FiO₂ ratio as oxygenation criterion (resource-limited settings where ABG unavailable)
- Allows lung ultrasound as alternative to CXR/CT for bilateral opacities
- Better applicable to low/middle income countries
PART 2: PATHOPHYSIOLOGY UNDERPINNING VENTILATION STRATEGY
"Baby Lung" Concept (Gattinoni)
- ARDS is non-homogeneous - lung involvement is patchy, not uniform
- CT scan reveals: normal aerated lung (anterior), consolidated/collapsed lung (posterior/dependent), and recruitable atelectatic regions
- The total volume of "aerated" lung behaves as if it were a small, healthy "baby lung" (300-500 mL instead of normal 3-4L)
- Tidal volume set by weight but delivered into this small aerated region → high stress/strain per unit volume → ventilator-induced lung injury (VILI)
Types of Ventilator-Induced Lung Injury (VILI)
| Type | Mechanism | Prevention |
|---|---|---|
| Barotrauma | High pressure rupture → pneumothorax, pneumomediastinum | Limit Pplat ≤30 cmH₂O |
| Volutrauma | Over-distension of alveoli by high tidal volumes | Low Vt 4-6 mL/kg PBW |
| Atelectrauma | Cyclic opening/closing of alveoli | Adequate PEEP (alveolar recruitment) |
| Biotrauma | Mechanical stress → inflammatory cytokines → SIRS | All of the above |
| Stress raisers | Heterogeneity of lung → normal zones over-stressed | Homogeneous recruitment |
PART 3: THE ARDSNet ARMA PROTOCOL - THE LANDMARK TRIAL
- Tidal volume 6 mL/kg PBW vs 12 mL/kg PBW
- Result: 6 mL/kg group → 22% reduction in mortality (39.8% vs 31%)
- This established low tidal volume ventilation as standard of care
- Fishman's: "Clinicians should employ the entire ARDSNet protocol rather than selected parts"
PART 4: LUNG PROTECTIVE VENTILATION STRATEGY (CORE)
A. Tidal Volume (Most Important Parameter)
- Target: 4-6 mL/kg Predicted Body Weight (PBW)
- Acceptable range: 4-8 mL/kg PBW
- MUST use Predicted Body Weight, NOT actual body weight (actual weight overestimates by ~20% due to fat/oedema)
- Males: 50 + 0.91 × [Height(cm) - 152.4] kg
- Females: 45.5 + 0.91 × [Height(cm) - 152.4] kg
B. Plateau Pressure (Pplat)
- Target: ≤30 cmH₂O (absolute ceiling)
- Pplat = Pressure during an inspiratory hold (no flow) = reflects alveolar end-inspiratory pressure
- Measured using an inspiratory hold manoeuvre
- If Pplat >30: reduce tidal volume in 1 mL/kg steps (minimum 4 mL/kg)
- Note: "Safe Pplat threshold" concept is NOT supported - lower is better across entire range (ARDSNet ARMA data)
C. Driving Pressure (Delta P, ΔP) - The Most Important Predictor
- Formula: ΔP = Pplat - PEEP
- Target: ≤15 cmH₂O
- Represents the tidal volume normalised to respiratory system compliance (ΔP = Vt/Crs)
- Amato et al. (NEJM 2015) - post-hoc analysis of 9 RCTs: Driving pressure is the best single predictor of mortality in ARDS, stronger than tidal volume or plateau pressure alone
- "Among ventilation variables...driving pressure is the variable that best stratifies risk of mortality" (Fishman's)
- Current thinking: Titrate PEEP and Vt to minimise driving pressure ≤15 cmH₂O
D. PEEP (Positive End-Expiratory Pressure)
- Prevent alveolar collapse at end-expiration (prevents atelectrauma)
- Recruit collapsed/flooded alveoli (improve oxygenation)
- Shift the lung up its compliance curve
| Method | Description |
|---|---|
| FiO₂/PEEP Table (ARDSNet) | Two tables: Low PEEP table and High PEEP table; match FiO₂ and PEEP combination |
| Decremental PEEP trial | Start with high PEEP (20-22 cmH₂O) after recruitment; progressively decrease while monitoring compliance/driving pressure; optimal PEEP = best compliance |
| PEEP-compliance (stress index) | On pressure-time curve: straight line = adequate PEEP; upward concavity = overdistension; downward concavity = derecruitment |
| Electrical Impedance Tomography (EIT) | Direct imaging of ventilation distribution; titrate PEEP to minimise collapsed and overdistended lung |
| Esophageal pressure-guided PEEP | Measures transpulmonary pressure; adjusts PEEP based on chest wall compliance (especially useful in obese patients) |
| Driving pressure-guided PEEP | Titrate PEEP to minimise driving pressure |
| FiO₂ | 0.3 | 0.4 | 0.4 | 0.5 | 0.5 | 0.6 | 0.7 | 0.7 | 0.7 | 0.8 | 0.9 | 0.9 | 0.9 | 1.0 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PEEP | 5 | 5 | 8 | 8 | 10 | 10 | 10 | 12 | 14 | 14 | 14 | 16 | 18 | 18-24 |
- ATS 2024: Conditional recommendation for high PEEP in moderate-severe ARDS (PF <200)
- ESICM 2023: No specific PEEP recommendation (heterogeneous trial results); individualise
- Meta-analysis (ALVEOLI, LOVS, EXPRESS): Higher PEEP in PF <200 shows mortality benefit trend; not significant overall
E. Respiratory Rate and Permissive Hypercapnia
- Respiratory rate: 20-35 breaths/min (titrated to pH, not PaCO₂)
- Permissive hypercapnia: Allow PaCO₂ to rise if needed to maintain low Vt
- pH target: >7.20 (Fishman's: "clinician-allowed hypercapnia...despite an ability to achieve normocapnia with higher tidal volumes")
- If pH <7.15-7.20: sodium bicarbonate IV (to enable further reduction of Vt) or increase RR
- Contraindications to permissive hypercapnia:
- Raised intracranial pressure (TBI, CNS injury)
- Severe pulmonary hypertension
- Severe right ventricular failure
- Metabolic acidosis already present
F. FiO₂ and Oxygenation Targets
- SpO₂ target: 88-95% (acceptable 88-96%)
- PaO₂ target: 55-80 mmHg (55-88 mmHg per ARDSNet)
- Avoid hyperoxia: PaO₂ >100 mmHg → free radical injury; absorption atelectasis
- During SBT assessment: Do NOT increase FiO₂ (AARC 2024)
G. Inspiratory Flow and I:E Ratio
- Inspiratory flow: 40-80 L/min in VCV mode
- I:E ratio: Normal 1:2; can be 1:1 to 1:3 in ARDS
- Inverse ratio ventilation (I:E >1:1) may improve oxygenation but risk auto-PEEP
ARDSNet Protocol Summary (ARMA Study Protocol)
| Parameter | Target |
|---|---|
| Tidal Volume | 6 mL/kg PBW (reduce to 4 mL/kg if Pplat >30) |
| Pplat | ≤30 cmH₂O |
| Driving Pressure | ≤15 cmH₂O |
| RR | 6-35/min (titrate to pH) |
| FiO₂/PEEP | Per ARDSNet table |
| SpO₂ target | 88-95% |
| PaO₂ target | 55-88 mmHg |
| pH target | 7.30-7.45 |
| Permissive hypercapnia | pH >7.20 acceptable |
| Mode | VCV-AC preferred (evidence base); PCV acceptable |
PART 5: ADJUNCT VENTILATION STRATEGIES
1. PRONE POSITIONING (Strongest Evidence After Low Vt)
- Redistributes lung oedema from dorsal to ventral
- Recruits dorsal (previously dependent/collapsed) lung units
- Reduces dorsoventral transpulmonary pressure gradient → more homogeneous ventilation
- Reduces V/Q mismatch; improves dead space
- Reduces VILI (more homogeneous stress distribution)
- Reduces lung compression from heart (cardiac weight effect)
- 466 patients with severe ARDS (PF <150 with PEEP ≥5, FiO₂ ≥0.6)
- Prone ≥16h/day vs supine
- 28-day mortality: 16% (prone) vs 32.8% (supine) - dramatic benefit
- 90-day mortality: 23.6% vs 41%
- Relative Risk Reduction: ~50%
- ATS 2024: >12 hours/day
- ESICM 2023: >16 hours/day (PROSEVA duration)
- Severe ARDS: PaO₂/FiO₂ <150 mmHg with PEEP ≥5, FiO₂ ≥0.6 (PROSEVA criteria)
- Some centres: PF <200 (moderate ARDS) with lack of response to PEEP optimisation
- Unstable spine fractures, open sternum
- Facial trauma, recent tracheal surgery
- Intracranial hypertension (may worsen)
- Massive haemoptysis
- Pregnancy (after 20 weeks)
- Extreme obesity (team-dependent)
- PF ratio >150 with PEEP ≤10 and FiO₂ ≤0.6 for ≥4 hours in supine position
- If complications arise
2. RECRUITMENT MANOEUVRES (RMs)
- Sustained inflation (SI): CPAP 30-40 cmH₂O for 40-60 seconds
- Incremental PEEP (step-up PEEP RM): PEEP 10→15→20→25→30 cmH₂O with assessment at each step (safer)
- Pressure-controlled RM: Peak pressure 40-60 cmH₂O for ≥2 minutes
- ATS 2024: Strong recommendation AGAINST lung recruitment manoeuvres in ARDS
- ESICM 2023: Strong recommendation AGAINST prolonged LRMs; weak recommendation against brief LRMs
- Based on: ART Trial (NEJM 2017) - maximal lung recruitment + PEEP titration strategy INCREASED 28-day mortality vs low PEEP control (55% vs 49%)
- Message: Aggressive sustained recruitment is harmful; the benefit of opening collapsed alveoli does not outweigh the harm from overdistension
3. NEUROMUSCULAR BLOCKING AGENTS (NMBs)
- Eliminates patient-ventilator asynchrony
- Reduces oxygen consumption
- Reduces patient-driven worsening of VILI (P-SILI: Patient Self-Inflicted Lung Injury)
- Improves chest wall compliance, facilitates prone positioning
| Trial | Year | Result |
|---|---|---|
| ACURASYS | 2010 | Cisatracurium 48h → improved 90-day survival (hazard ratio 0.68) |
| ROSE Trial | 2019 | Cisatracurium 48h vs light sedation → No mortality benefit (38.5% vs 33.8%); challenged ACURASYS |
- ATS 2024: Suggests NMBs in early severe ARDS (PF <150) for up to 48h (conditional recommendation)
- ESICM 2023: Does NOT recommend routine NMBs; use for severe patient-ventilator asynchrony or facilitation of prone positioning
- Practical approach: Individualized - consider NMBs when significant asynchrony despite optimised sedation, or to facilitate prone positioning in severe ARDS
- Monitor with TOF (Train-of-Four) if using infusion
4. CORTICOSTEROIDS
- ARDS is partly mediated by dysregulated inflammation
- Corticosteroids reduce pro-inflammatory cytokines (IL-6, TNF-α)
- Also reduce fibroproliferative phase (late ARDS)
| Trial | Finding |
|---|---|
| DEXA-ARDS (Villar 2020) | Dexamethasone 20 mg/day × 5 days → 10 mg × 5 days: reduced 60-day mortality (21% vs 36%) in moderate-severe ARDS |
| CAPE-COVID (2020) | Hydrocortisone did not significantly reduce treatment failure in COVID ARDS |
| RECOVERY Trial (REMAP-CAP 2021) | Dexamethasone 6 mg/day for COVID-19: reduced 28-day mortality in ventilated patients |
| Ho et al. meta-analysis (2020) | Corticosteroids: reduced 28-day mortality and increased VFDs in ARDS |
5. INHALED VASODILATORS
- Both improve PaO₂/FiO₂ transiently (short-term oxygenation benefit)
- No mortality benefit demonstrated in RCTs
- Used as rescue/bridging therapy (to buy time while arranging ECMO or prone positioning)
- iNO dose: 5-40 ppm
- Inhaled epoprostenol: 25-50 ng/kg/min
6. AIRWAY PRESSURE RELEASE VENTILATION (APRV)
- Essentially inverse-ratio ventilation with a long high-pressure phase (Phigh) and brief release phase (Plow)
- Patient breathes spontaneously at Phigh (CPAP baseline)
- Brief release to Plow (near 0 cmH₂O) allows CO₂ elimination
- Maintains "open lung" with minimal alveolar cycling
- Phigh: 25-30 cmH₂O (alveolar recruitment pressure)
- Plow: 0-5 cmH₂O
- Thigh: 4-6 seconds (long phase)
- Tlow: 0.5-0.8 seconds (short release; titrate to terminate when expiratory flow = 50-75% peak expiratory flow)
- Better patient comfort; less sedation needed
- Mean airway pressure high → excellent oxygenation
- Spontaneous breathing preserved → less diaphragm atrophy
- Lower peak inspiratory pressures
- No RCT evidence of mortality benefit over standard LPV
- Risk of volutrauma if spontaneous efforts generate high tidal volumes
- Complex settings management
- Current evidence: APRV appears safe in TBI (per ARDS management guide)
7. HIGH-FREQUENCY OSCILLATORY VENTILATION (HFOV)
- OSCAR Trial (2013): HFOV vs conventional LPV - no mortality difference
- OSCILLATE Trial (2013): HFOV increased in-hospital mortality (47% vs 35%)
- ATS 2017/2024: Strong recommendation AGAINST routine HFOV in moderate-severe ARDS (high confidence)
- ESICM 2023: Strong recommendation against HFOV
- HFOV is no longer recommended as a standard rescue modality for ARDS
8. VV ECMO (See Previous Comprehensive Answer)
- Indication: Refractory ARDS - PF <80 after optimal management including proning
- ATS 2024: Conditional recommendation for VV ECMO in severe ARDS
- ESICM 2023: Strong recommendation for VV ECMO in ECMO-capable centre
- EOLIA Trial: 60-day mortality 35% vs 46% (not significant; 28% crossover)
- On VV ECMO: ultra-protective ventilation (Vt 3-4 mL/kg, Pplat <25 cmH₂O, RR 4-15)
PART 6: VENTILATION BY ARDS SEVERITY - MANAGEMENT ALGORITHM
ALL ARDS → LUNG PROTECTIVE VENTILATION (Vt 4-6 mL/kg PBW, Pplat ≤30, DP ≤15)
→ Optimise sedation, minimise sedation depth (RASS -2 to 0)
→ Conservative fluid management (FACTT trial: neutral/negative balance)
→ No recruitment manoeuvres (ATS 2024)
PF <200 (MODERATE-SEVERE):
→ HIGH PEEP strategy (ATS 2024 conditional)
→ Corticosteroids (ATS 2024 conditional)
→ Consider iNO/epoprostenol as bridge if not responding
PF <150 (SEVERE):
→ PRONE POSITIONING ≥12-16h/day (STRONG recommendation, ATS/ESICM)
→ Deep sedation (RASS -4/-5) + consider NMBs for asynchrony or proning
→ Inhaled vasodilators as rescue bridge
→ If still <80 after all measures → VV ECMO
RESCUE THERAPIES (Not first-line; no mortality evidence):
→ APRV (mode alternative)
→ Inhaled NO / Prostacyclin
→ VV ECMO (definitive rescue)
→ NOT HFOV (harmful)
PART 7: SUMMARY COMPARISON TABLE - GUIDELINE RECOMMENDATIONS
| Intervention | ATS 2024 | ESICM 2023 | Evidence |
|---|---|---|---|
| Low Vt (4-8 mL/kg PBW) | Strong ↑ | Strong ↑ | ARDSNet ARMA |
| Prone positioning (severe, PF<150) | Strong ↑ (>12h) | Strong ↑ (>16h) | PROSEVA trial |
| High PEEP (moderate-severe) | Conditional ↑ | No recommendation | ALVEOLI/LOVS/EXPRESS |
| Prolonged recruitment manoeuvres | Strong ↓ | Strong ↓ | ART Trial |
| Brief RMs | Conditional ↓ | Weak ↓ | Limited data |
| HFOV | Strong ↓ | Strong ↓ | OSCAR, OSCILLATE |
| Corticosteroids | Conditional ↑ | Conditional ↑ | DEXA-ARDS, RECOVERY |
| NMBs (severe ARDS <48h) | Conditional ↑ | ↓ routine use | ROSE vs ACURASYS |
| VV ECMO (refractory) | Conditional ↑ | Strong ↑ (ECMO centre) | EOLIA trial |
| iNO/prostacyclin | No benefit in mortality; bridge only | Bridge only | Multiple RCTs |
NEET SS CRITICAL CARE MCQs: ARDS & LUNG PROTECTIVE VENTILATION
- A) PaO₂/FiO₂ 200-300 mmHg with any PEEP
- B) PaO₂/FiO₂ 100-200 mmHg with PEEP ≥5 cmH₂O
- C) PaO₂/FiO₂ <100 mmHg with PEEP ≥5 cmH₂O
- D) PaO₂/FiO₂ <150 mmHg with any FiO₂
- A) PBW = 60 kg; Vt = 360 mL
- B) PBW = 73.6 kg; Vt = 442 mL
- C) PBW = 70.2 kg; Vt = 421 mL (6 mL/kg)
- D) PBW = 80 kg; Vt = 480 mL
- A) Peak pressure - PEEP
- B) Plateau pressure - PEEP
- C) Peak pressure - Plateau pressure
- D) Tidal volume × respiratory rate
- A) No significant difference in 28-day mortality between prone and supine
- B) Prone positioning increased mortality due to complications
- C) 28-day mortality 16% (prone) vs 32.8% (supine) - approximately 50% relative risk reduction
- D) Prone positioning was only beneficial in mechanically ventilated patients with COVID-19
- A) Strong recommendation for use in all ARDS patients at initiation of ventilation
- B) Conditional recommendation to use stepwise PEEP increments as routine LRM
- C) Strong recommendation AGAINST use of prolonged LRMs; both guidelines advise against routine use
- D) LRMs are recommended only in combination with HFOV
- A) Cisatracurium 48h significantly reduced 90-day mortality compared to light sedation
- B) Cisatracurium 48h provided no mortality benefit compared to light sedation; 38.5% vs 33.8% mortality
- C) NMBs should be used for all patients with moderate ARDS
- D) NMBs were harmful and associated with increased ARDS mortality
- A) After the first prone session regardless of results
- B) After 7 days of proning
- C) When PF >150, PEEP ≤10, FiO₂ ≤0.6 maintained for ≥4 hours in supine position
- D) When RASS reaches -2 and sedation can be reduced
- A) Maximal lung recruitment strategy improved survival and reduced ICU stay
- B) Maximal recruitment + PEEP titration significantly INCREASED 28-day mortality (55% vs 49% control)
- C) Stepwise PEEP increases of 2 cmH₂O were safe and effective
- D) Recruitment manoeuvres only cause harm in mild ARDS
- A) HFOV (High-Frequency Oscillatory Ventilation)
- B) APRV (Airway Pressure Release Ventilation)
- C) Volume-Controlled Assist-Control (VCV-AC) with ARDSNet low tidal volume protocol
- D) Pressure Support Ventilation (PSV) alone
- A) A disease exclusively affecting neonates and infants
- B) A uniform process where all lung regions are equally affected
- C) A heterogeneous injury where the aerated functional lung behaves as if it were a small neonatal lung - only 300-500 mL available for ventilation despite normal adult body weight
- D) A condition where the lungs shrink in size due to fibrosis
- A) Methylprednisolone 1 mg/kg/day for 7 days
- B) Dexamethasone 20 mg/day for 5 days, then 10 mg/day until day 10 or extubation
- C) Hydrocortisone 200 mg/day for 7 days only in septic ARDS
- D) Prednisolone 40 mg/day for 14 days
- A) Strongly recommended for severe ARDS as rescue when prone fails
- B) Strongly recommended AGAINST by both ATS 2024 and ESICM 2023 based on the OSCILLATE and OSCAR trials
- C) Equivalent in efficacy to ARDSNet protocol with no difference in mortality
- D) Recommended as first-line mode in all moderate-severe ARDS
- A) 28 cmH₂O
- B) 12 cmH₂O
- C) 16 cmH₂O
- D) 40 cmH₂O
- A) Deliberately increasing CO₂ by decreasing RR to promote bronchodilation
- B) Accepting elevated PaCO₂ as a consequence of low tidal volume lung protection, maintaining pH >7.20
- C) Ventilating patients with FiO₂ 1.0 to compensate for rising CO₂
- D) Adding CO₂ to the inspiratory gas mixture
- A) Start HFOV immediately
- B) Initiate VV ECMO without delay
- C) Return to prone position; optimise ventilator settings; consider VV ECMO if criteria met (PF <80 after proning + optimal management for >6 hours)
- D) Increase PEEP to 24 cmH₂O and perform sustained recruitment manoeuvre
RAPID REVISION: KEY NUMBERS IN ARDS
| Parameter | Target/Threshold |
|---|---|
| Tidal Volume | 4-6 mL/kg PBW (range 4-8) |
| Plateau Pressure | ≤30 cmH₂O |
| Driving Pressure | ≤15 cmH₂O |
| Minimum PEEP | ≥5 cmH₂O |
| SpO₂ target | 88-95% |
| PaO₂ target | 55-88 mmHg |
| pH (permissive hypercapnia) | >7.20 |
| PROSEVA proning duration | ≥16 hours/day |
| ATS proning duration | ≥12 hours/day |
| Prone indication (PROSEVA) | PF <150 with PEEP ≥5, FiO₂ ≥0.6 |
| ECMO indication (ELSO) | PF <80 after optimal management |
| Corticosteroids (DEXA-ARDS) | Dexamethasone 20 mg × 5d → 10 mg × 5d |
| Mode of choice | VCV-AC (evidence base) |
| HFOV | Strongly recommended AGAINST |
| Recruitment manoeuvres | Strongly recommended AGAINST |
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (ARDSNet protocol, driving pressure, PEEP, ECMO ventilation strategy)
- ARDSNet ARMA Trial - NEJM 2000 (Vt 6 mL/kg)
- PROSEVA Trial (Guerin et al., NEJM 2013 - prone positioning)
- ART Trial (NEJM 2017 - LRMs increase mortality)
- ACURASYS (2010) vs ROSE Trial (NEJM 2019 - NMBs)
- Amato et al., NEJM 2015 (driving pressure as mortality predictor)
- DEXA-ARDS Trial (Villar 2020) + ATS 2024 corticosteroid recommendation
- ATS 2024 ARDS Guidelines update
- ESICM 2023 ARDS Guidelines + ATS/ESICM comparison
- EOLIA Trial (2018 - VV ECMO in severe ARDS)
- Matthay et al. AJRCCM 2024 (New Global ARDS Definition)
Shock, sepsis and organ dysfunction. Discuss the recent guidelines in the management of septic shock. What is shock? What are the different types of shock? Write briefly about the management of septic shock in an ICU. Write a short note on SOFA and QSOFA in sepsis. For md anaesthesia exam . With possible neet ss critical care questions .
Surviving Sepsis Campaign 2021 guidelines septic shock management vasopressors fluids antibiotics organ dysfunction recommendations
septic shock management guidelines norepinephrine vasopressin hydrocortisone fluid resuscitation
https://link.springer.com/article/10.1007/s00063-023-01028-5
Surviving Sepsis Campaign 2021 sepsis guidelines international management
sepsis 3 definition 2016 Sepsis-3 Singer SOFA organ dysfunction SIRS comparison qSOFA bedside screening
https://dig.pharmacy.uic.edu/faqs/2022-2/march-2022-faqs/upd…
SHOCK, SEPSIS AND ORGAN DYSFUNCTION
Management of Septic Shock | SOFA and qSOFA
MD Anaesthesia Examination | NEET SS Critical Care
PART 1: DEFINITION OF SHOCK
Oxygen Delivery Equation:
- DO₂ = CO × CaO₂
- CaO₂ = (Hb × 1.36 × SaO₂) + (0.0034 × PaO₂)
- Normal DO₂ = 1000 mL/min; Normal VO₂ = 250 mL/min
- When DO₂ falls below critical threshold (~330 mL/min) → oxygen extraction cannot compensate → anaerobic metabolism → lactic acidosis
Clinical Hallmarks of Shock:
- Hypotension (MAP <65 mmHg or SBP <90 mmHg)
- Tachycardia
- Altered mental status (confusion, obtundation)
- Oliguria (<0.5 mL/kg/h)
- Elevated serum lactate (>2 mmol/L)
- Peripheral shutdown (cold clammy extremities - except distributive shock)
PART 2: CLASSIFICATION OF SHOCK
1. DISTRIBUTIVE SHOCK (Most Common)
| Type | Cause | Key Feature |
|---|---|---|
| Septic | Bacterial/fungal infection → cytokine storm | Most common ICU cause; high lactate |
| Anaphylactic | IgE-mediated (drugs, foods, venom) | Urticaria, bronchospasm; epinephrine first-line |
| Neurogenic | High spinal cord injury (≥T6) | Bradycardia + hypotension (no reflex tachy) |
| Endocrine | Adrenal crisis, myxoedema coma | History of steroids/thyroid disease |
| Pancreatitis/Burns | Massive third-space fluid losses + vasodilation | Context dependent |
2. CARDIOGENIC SHOCK
| Cause | Notes |
|---|---|
| AMI (most common) | Loss of >40% LV mass → pump failure |
| Acute myocarditis | Viral; potentially reversible |
| Severe arrhythmia (VT/AF) | Rate control/cardioversion |
| Severe valvular disease | Acute MR/AR/critical AS |
| Post-cardiotomy | After cardiac surgery |
| Stress cardiomyopathy | Takotsubo; catecholamine-related |
3. HYPOVOLEMIC SHOCK
| Type | Cause |
|---|---|
| Haemorrhagic | Trauma, GI bleed, ruptured ectopic, aortic aneurysm |
| Non-haemorrhagic | Vomiting/diarrhoea, burns, polyuria (DKA, DI) |
| Class | Blood loss | HR | SBP | RR | Mental Status |
|---|---|---|---|---|---|
| I | <750 mL (<15%) | <100 | Normal | 14-20 | Normal |
| II | 750-1500 mL (15-30%) | 100-120 | Normal | 20-30 | Anxious |
| III | 1500-2000 mL (30-40%) | >120 | Decreased | 30-40 | Confused |
| IV | >2000 mL (>40%) | >140 | Very low | >35 | Lethargic |
4. OBSTRUCTIVE SHOCK
| Cause | Specific Feature | Treatment |
|---|---|---|
| Tension pneumothorax | Absent breath sounds; tracheal deviation | Immediate needle decompression → chest drain |
| Cardiac tamponade | Beck's triad (hypotension, JVD, muffled heart sounds); pulsus paradoxus | Emergency pericardiocentesis |
| Massive PE | RV strain on echo; S1Q3T3 ECG | Thrombolysis; surgical embolectomy; catheter-directed therapy |
| Constrictive pericarditis | Kussmaul sign; pericardial knock | Pericardiectomy |
| Aortic dissection | Differential pulses; mediastinal widening | Emergency surgery |
HAEMODYNAMIC PROFILES IN SHOCK - SUMMARY TABLE
| Parameter | Distributive | Cardiogenic | Hypovolemic | Obstructive |
|---|---|---|---|---|
| CO/CI | ↑ (or normal) | ↓↓ | ↓ | ↓ |
| SVR | ↓↓ | ↑ | ↑ | ↑ |
| PCWP | ↓ (or normal) | ↑↑ | ↓ | ↓ (or ↑ in tamponade) |
| CVP | ↓ (or normal) | ↑ | ↓ | ↑ (except PE) |
| SvO₂ | ↑ (shunting) | ↓ | ↓ | ↓ |
| MAP | ↓ | ↓ | ↓ | ↓ |
PART 3: DEFINITIONS - SEPSIS AND SEPTIC SHOCK (SEPSIS-3, 2016)
- SIRS: 2 of 4 criteria (temp, HR, RR, WBC)
- Sepsis = SIRS + infection
- Severe sepsis = Sepsis + organ dysfunction
- Septic shock = Severe sepsis + refractory hypotension
- SIRS is non-specific (can occur in pancreatitis, burns, surgery)
- Focuses only on inflammatory components; ignores non-inflammatory organ dysfunction
- Implies a continuum from SIRS → sepsis → septic shock (which is not always true)
SEPSIS-3 DEFINITIONS (Singer et al., JAMA 2016)
"Life-threatening organ dysfunction caused by a dysregulated host response to infection"
- Organ dysfunction = SOFA score increase ≥2 points from baseline
- SOFA ≥2 associated with >10% in-hospital mortality
- The term "severe sepsis" is abolished (redundant - all sepsis involves organ dysfunction)
"A subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality"
- Vasopressor requirement to maintain MAP ≥65 mmHg, AND
- Serum lactate >2 mmol/L (18 mg/dL) despite adequate volume resuscitation
- In-hospital mortality >40%
PART 4: SOFA SCORE (Sequential Organ Failure Assessment)
SOFA Score Components and Scoring:
| Organ System | Parameter | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| Respiratory | PaO₂/FiO₂ (mmHg) | ≥400 | 300-400 | 200-300 | 100-200 (+ ventilated) | <100 (+ ventilated) |
| Coagulation | Platelets (×10³/µL) | ≥150 | 100-150 | 50-100 | 20-50 | <20 |
| Liver | Bilirubin (mg/dL) | <1.2 | 1.2-2.0 | 2.0-6.0 | 6.0-12.0 | >12.0 |
| Cardiovascular | MAP/vasopressors | MAP ≥70 | MAP <70 | Dopamine <5 or dobutamine | Dopamine 5-15 or NE ≤0.1 | Dopamine >15 or NE >0.1 µg/kg/min |
| CNS | Glasgow Coma Scale | 15 | 13-14 | 10-12 | 6-9 | <6 |
| Renal | Creatinine (mg/dL) / Urine output | <1.2 | 1.2-2.0 | 2.0-3.5 | 3.5-5.0 / <500 mL/day | >5.0 / <200 mL/day |
- Each organ system scored 0-4
- Total score 0-24
- Baseline SOFA assumed = 0 (unless chronic organ dysfunction known)
- Increase ≥2 from baseline = SEPSIS (life-threatening organ dysfunction)
- Higher SOFA scores correlate with increasing mortality
| Total SOFA | Approximate Mortality |
|---|---|
| <9 | ~33% |
| 9-11 | ~50% |
| ≥12 | >75-80% |
- Diagnosis of sepsis (acute SOFA increase ≥2)
- Prognosis of outcome in ICU
- Daily monitoring of organ function trajectory (improving vs. deteriorating)
- Research end-point in sepsis trials
PART 5: qSOFA (Quick SOFA)
qSOFA Criteria (1 point each):
| Criterion | Threshold | Score |
|---|---|---|
| Altered mental status | GCS <15 | 1 |
| Respiratory rate | ≥22 breaths/min | 1 |
| Systolic blood pressure | ≤100 mmHg | 1 |
- qSOFA ≥2 = Suspect sepsis with poor outcome → full SOFA assessment; ICU review
- qSOFA ≥2 predicts: Prolonged ICU stay, high mortality
qSOFA vs SOFA vs SIRS - Comparison:
| Feature | SIRS | qSOFA | SOFA |
|---|---|---|---|
| Criteria | 4 (temp, HR, RR, WBC) | 3 (AMS, RR, SBP) | 6 organ systems |
| Lab required | Partial (WBC, temp optional) | None | Yes |
| Bedside | Partial | Yes | No |
| Setting | ER/ward/ICU | Outside ICU (ward, ER, prehospital) | ICU |
| Sensitivity | High | Low (29.7%) | Moderate |
| Specificity | Low (61.1%) | High (96.1%) | High |
| Purpose | Screening for SIRS | Identify high-risk sepsis patients | Diagnose/quantify organ dysfunction |
"We recommend against using qSOFA alone as a single screening tool for sepsis compared to SIRS, NEWS (National Early Warning Score), or MEWS."
PART 6: SURVIVING SEPSIS CAMPAIGN (SSC) 2021 GUIDELINES - KEY RECOMMENDATIONS
SECTION 1: SCREENING AND EARLY MANAGEMENT
- Suggest routine sepsis screening tools for acutely ill patients at high risk
- Recommend AGAINST using qSOFA alone as the primary screening tool (SSC 2021 - KEY CHANGE)
- Measure lactate (re-measure if >2 mmol/L)
- Obtain blood cultures BEFORE antibiotics
- Administer broad-spectrum antibiotics
- Administer 30 mL/kg crystalloid for hypotension/lactate ≥4 mmol/L
- Apply vasopressors if hypotensive during/after fluid resuscitation to maintain MAP ≥65 mmHg
SECTION 2: INITIAL RESUSCITATION
A. Fluid Resuscitation
- Recommend: 30 mL/kg of IV crystalloid within first 3 hours (weak recommendation - downgraded from 2016 strong recommendation)
- After initial 30 mL/kg: use dynamic fluid responsiveness measures (SV variation, pulse pressure variation, passive leg raise test, echo) to guide further fluid
- 2021 NEW RECOMMENDATION: Use BALANCED CRYSTALLOIDS (Ringer's Lactate / PlasmaLyte) over 0.9% Normal Saline (weak recommendation)
- Based on SMART and SALT-ED trials: balanced crystalloids reduced AKI and death vs saline
- Normal saline → hyperchloraemic metabolic acidosis → renal vasoconstriction → AKI
- Albumin: Suggest using albumin when patients have received LARGE volumes of crystalloids (weak recommendation) - the BIG trial 2022 did not show albumin benefit in all-comers
- Recommend AGAINST hydroxyethyl starches (HES) - increased AKI (VISEP, CRYSTMAS trials)
- Suggest AGAINST gelatins - increased adverse effects; inconclusive mortality benefit
- SSC 2021: INSUFFICIENT EVIDENCE to recommend restrictive vs. liberal fluid strategy beyond initial resuscitation - this remains an important evidence gap
B. MAP Target
- Recommend: Initial MAP target ≥65 mmHg (strong recommendation)
- No benefit to higher MAP target (65-70 vs 80-85: SEPSISPAM trial showed no mortality difference; higher MAP associated with more AF)
C. Resuscitation Endpoints
| Parameter | Target | SSC 2021 Guidance |
|---|---|---|
| Lactate | Normalise lactate (<2 mmol/L) | Suggest lactate-guided resuscitation (weak recommendation) |
| Capillary refill time | <2 seconds | 2021 NEW: suggest capillary refill time as adjunct to guide resuscitation (ANDROMEDA-SHOCK trial) |
| ScvO₂ | >70% | No longer specific target (after PROCESS, ARISE, ProMISe trials refuted EGDT) |
| CVP | NOT a fluid responsiveness target | CVP unreliable marker of fluid responsiveness |
SECTION 3: INFECTION MANAGEMENT
A. Antimicrobial Timing
- Septic shock or high likelihood of sepsis: Antibiotics within 1 hour of recognition (UNCHANGED from 2016)
- Sepsis without shock (possible infection): Rapid clinical + laboratory assessment → if concern persists → antibiotics within 3 hours
B. Blood Cultures
- Obtain AT LEAST 2 sets of blood cultures before antibiotics (aerobic + anaerobic) - Best Practice Statement
- Do NOT delay antibiotics >45 minutes to obtain cultures
C. Antibiotic Selection
- Empiric BROAD-SPECTRUM coverage for likely pathogens + susceptibility patterns
- Combination therapy for:
- Patients at high risk of multi-drug resistant (MDR) organisms
- Septic shock (double gram-negative coverage initially)
- De-escalate based on culture/sensitivity results as early as possible (antibiotic stewardship)
- Duration: 7-10 days for most; shorter for good source control; PCT-guided de-escalation suggested (SSC 2021 - weak recommendation)
- Suggest using PCT to support SHORTENING duration of antibiotics (weak recommendation, low QoE) - new in 2021
- Suggest using PCT + clinical evaluation to support STOPPING antibiotics (weak recommendation)
D. Source Control
- Identify and control source of infection within first 6-12 hours (drain abscess, remove infected device, resect necrotic bowel)
- Remove intravascular access devices that may be the source (after establishing alternative access)
SECTION 4: HAEMODYNAMIC MANAGEMENT (VASOPRESSORS)
A. First-Line Vasopressor
- NOREPINEPHRINE (noradrenaline) = FIRST-LINE (strong recommendation)
- Dose: Start 0.01-0.1 mcg/kg/min; titrate to MAP ≥65 mmHg
- α₁ + β₁ agonist; predominantly vasoconstricts; some inotropy
B. Vasopressin
- ADD vasopressin when norepinephrine dose ≥0.25-0.5 mcg/kg/min (strong recommendation) to achieve MAP target OR to lower NE dose
- Dose: 0.03 units/min (fixed, non-titratable; do NOT exceed 0.04 units/min)
- Mechanism: V₁ receptor → vasoconstriction; V₂ → antidiuretic; relatively vasopressin-deficient in vasodilatory shock
- May reduce AKI (VANISH trial)
C. Epinephrine
- Add epinephrine as second-line if MAP target not achieved with NE + vasopressin (weak recommendation)
- Note: Can elevate lactate independently (glycolysis stimulation) → lactate unreliable as resuscitation endpoint with epinephrine
D. Peripheral Vasopressor Administration
- 2021 NEW RECOMMENDATION: Suggest initiating vasopressors PERIPHERALLY (antecubital or above) rather than delaying while awaiting central venous access (weak recommendation, very low QoE)
- Peripheral NE safe for short durations (up to 6 hours) in proximal large veins
- Do NOT delay vasopressors for central access - hypotension causes more harm than short peripheral vasopressor use
E. Dopamine
- Recommend AGAINST using dopamine instead of norepinephrine (strong recommendation)
- Dopamine: No renal protection (low-dose "renal dopamine" myth debunked); higher arrhythmia rate (SOAP II trial: AF 24% vs 12% with NE)
F. Phenylephrine
- Not first-line; pure α₁ agonist; reduces HR (reflex bradycardia); may reduce CO
- Use: Severe tachycardia where NE's β₁ effect undesirable; OR short-term when NE unavailable
G. Dobutamine
- Add dobutamine when evidence of myocardial dysfunction + persistent hypoperfusion despite adequate fluid + vasopressors
- Dose: 2.5-20 mcg/kg/min
- β₁ + β₂ agonist: ↑CO; ↓SVR (may worsen hypotension; use with vasopressor)
H. Corticosteroids
- Vasopressor (NE or equivalent) dose ≥0.25 mcg/kg/min for ≥4 hours to maintain MAP target
- Hydrocortisone 200 mg/day as continuous infusion or 50 mg q6h IV (preferred)
- NOT bolus 100 mg q8h (inferior pharmacokinetics)
- Continue until vasopressors no longer needed; taper and stop
- ADRENAL trial (Gordon 2018): Hydrocortisone → faster shock resolution, shorter MV duration; NO mortality benefit at 90 days
- APROCCHSS trial (Annane 2018): Hydrocortisone + fludrocortisone → reduced 90-day mortality (43% vs 49%)
- Meta-analysis: ↑vasopressor-free days; ↑neuromuscular weakness; no clear mortality benefit
SECTION 5: INVASIVE MONITORING
- Arterial line: Recommended for all patients requiring vasopressors (continuous MAP monitoring, frequent ABGs)
- Central venous catheter: For vasopressors (after initial stabilisation on peripheral), fluid administration, CVP monitoring
- Cardiac output monitoring (PA catheter/echo): Not routinely recommended; use for complex haemodynamics, suspected myocardial dysfunction
- Echocardiography: Suggest early assessment of cardiac function to guide fluid and vasopressor management (new in 2021)
SECTION 6: VENTILATION IN SEPTIC SHOCK
- Sepsis-induced ARDS: Low Vt ventilation (6 mL/kg PBW), Pplat ≤30, prone for PF <150
- Sepsis-induced hypoxaemia (non-ARDS): Trial of HFNC (if breathing spontaneously); low threshold for intubation if worsening
- Goal: Avoid intubation if possible; HFNC/NIV trial appropriate in selected patients
SECTION 7: OTHER THERAPIES
- Initiate insulin when 2 consecutive glucose >180 mg/dL (>10 mmol/L) (strong recommendation)
- Target: Blood glucose 144-180 mg/dL (8-10 mmol/L) - NOT tight glycaemic control (NICE-SUGAR: tight control increases hypoglycaemia and mortality)
- LMWH (preferred) or UFH (strong recommendation) unless contraindicated
- Mechanical prophylaxis (compression stockings/IPC) when pharmacological contraindicated
- Initiate RRT when life-threatening fluid/electrolyte/acid-base imbalance persists
- Recommend AGAINST using RRT solely to prevent AKI (STARRT-AKI trial: no benefit early vs delayed RRT)
- CRRT (continuous) preferred in haemodynamically unstable; IHD if stable
- Suggest PPIs in patients with sepsis at high risk of GI bleeding (strong recommendation)
- High-risk features: Mechanical ventilation, coagulopathy, prior GI bleed, high-dose steroids
- Enteral nutrition preferred over parenteral (strong recommendation)
- Early enteral nutrition within 24-48 hours of ICU admission when patient haemodynamically stable
- Do NOT force early full-caloric feeding if patient not tolerating (CALORIES, PERMIT trials)
SECTION 8: LONG-TERM OUTCOMES (NEW IN SSC 2021)
- Suggest ICU follow-up clinics
- Screen for post-intensive care syndrome (PICS): physical, cognitive, psychiatric sequelae
- Suggest rehabilitation interventions
- Family support and psychological counselling
SSC 2021 KEY CHANGES FROM 2016 - SUMMARY
| Domain | SSC 2016 | SSC 2021 | Change |
|---|---|---|---|
| qSOFA | Endorsed as screening | Recommend AGAINST as sole screening tool | Downgraded |
| Fluid type | Balanced OR saline | Balanced crystalloids preferred | Upgraded |
| Fluid dose beyond initial | Liberal approach | Insufficient evidence; suggest dynamic assessment | Downgraded |
| Vasopressor route | Central venous access | Peripheral initiation acceptable (new) | New |
| Dopamine | Avoid if possible | Recommend AGAINST (strong) | Stronger |
| Vasopressin threshold | Add early | Add at NE ≥0.25 mcg/kg/min (specific) | More specific |
| Corticosteroids | Against if responsive to fluids+vasopressors | Suggest when NE ≥0.25 for ≥4 hours (new trigger) | Upgraded/New |
| Antibiotics (shock) | Within 1 hour | Within 1 hour (unchanged) | Maintained |
| Antibiotics (sepsis, no shock) | Within 1 hour | Within 3 hours (with assessment) | Changed |
| PCT-guided de-escalation | Not addressed | Suggest PCT to support shortening (new) | New |
| Capillary refill time | Not mentioned | Suggest as adjunct (new) | New |
| Echocardiography | Not specified | Suggest early cardiac assessment (new) | New |
| Long-term outcomes | Not in guidelines | New section on PICS, follow-up (new) | New |
NEET SS CRITICAL CARE MCQs: SHOCK, SEPSIS, SOFA/qSOFA
- A) Sepsis with temperature >38.5°C and WBC >12,000
- B) Sepsis with SBP <90 mmHg not responding to 2L fluid bolus
- C) Sepsis with vasopressor requirement to maintain MAP ≥65 mmHg AND serum lactate >2 mmol/L despite adequate volume resuscitation
- D) Infection with SIRS + organ failure
- A) Temperature, heart rate, respiratory rate
- B) Altered mental status (GCS <15), systolic BP ≤100 mmHg, respiratory rate ≥22/min
- C) Lactate >2, altered consciousness, MAP <65
- D) WBC >12,000, temperature >38.5°C, HR >90
- A) Dopamine remains acceptable as first-line vasopressor
- B) Peripheral vasopressor initiation is now suggested over delaying for central access
- C) Phenylephrine is now recommended ahead of norepinephrine
- D) Vasopressin should be started before norepinephrine
- A) 4 systems; maximum 16 points
- B) 5 systems; maximum 20 points
- C) 6 systems; maximum 24 points
- D) 7 systems; maximum 28 points
- A) Dextrose 5% in water (D5W)
- B) Hypertonic saline (3%)
- C) Balanced crystalloids (Ringer's Lactate / PlasmaLyte)
- D) Half-normal saline (0.45% NaCl)
- A) MAP <70 mmHg with no vasopressors
- B) Norepinephrine dose ≤0.1 mcg/kg/min OR dopamine 5-15 mcg/kg/min
- C) Dobutamine is the only vasopressor being used
- D) Systolic BP <90 mmHg on any vasopressor
- A) Any patient with septic shock regardless of vasopressor dose
- B) Vasopressor requirement of norepinephrine ≥0.25 mcg/kg/min for at least 4 hours to maintain MAP target
- C) Serum cortisol <18 mcg/dL on ACTH stimulation test
- D) Failure of all antibiotics after 72 hours
- A) ↓CO, ↑SVR, ↑PCWP - "cold and wet"
- B) ↓CO, ↑SVR, ↓PCWP - "cold and dry"
- C) ↑CO (or normal), ↓SVR, ↓MAP - "warm shock"
- D) Normal CO, ↑SVR, ↑PCWP - "warm and wet"
- A) Norepinephrine
- B) Vasopressin
- C) Dopamine
- D) Hydrocortisone
- A) Only after all cultures are collected and sensitivities returned
- B) Immediately within 1 hour of recognition
- C) Within 3 hours of presentation (same as sepsis without shock)
- D) Within 6 hours
- A) CVP-guided resuscitation vs. ScvO₂-guided resuscitation
- B) Capillary refill time-guided resuscitation vs. serum lactate-guided resuscitation
- C) Mean arterial pressure target 65 vs. 80 mmHg
- D) Balanced crystalloid vs. saline resuscitation
- A) Any SOFA score ≥2 regardless of baseline
- B) SOFA increase ≥2 from baseline associated with suspected or confirmed infection
- C) Total SOFA score ≥8
- D) SOFA increase ≥4 from baseline
- A) Add dopamine to norepinephrine
- B) Add vasopressin 0.03-0.04 units/min to norepinephrine (strong recommendation); then consider epinephrine as second-line
- C) Replace norepinephrine with epinephrine entirely
- D) Add phenylephrine as the second vasopressor
- A) Withholding is always preferred; once started, treatment cannot be stopped
- B) There is NO ethical difference - both are morally equivalent when treatment is futile or disproportionately burdensome
- C) Withdrawing is always considered euthanasia in sepsis
- D) Withdrawing requires a court order in all cases
RAPID REVISION TABLE: SEPSIS/SEPTIC SHOCK
| Concept | Key Value |
|---|---|
| Sepsis-3 definition | Organ dysfunction (SOFA ≥2) + dysregulated host response to infection |
| Septic shock definition | Sepsis + vasopressor for MAP ≥65 + lactate >2 despite adequate resuscitation |
| Septic shock mortality | >40% |
| qSOFA criteria | AMS + SBP ≤100 + RR ≥22; ≥2 = high risk |
| SSC 2021 on qSOFA | AGAINST using as sole screening tool |
| Initial fluid | 30 mL/kg crystalloid within 3 hours |
| Preferred crystalloid | Balanced (Ringer's Lactate/PlasmaLyte) over normal saline (2021 change) |
| MAP target | ≥65 mmHg |
| First vasopressor | Norepinephrine |
| Second vasopressor | Vasopressin (fixed 0.03-0.04 units/min) at NE ≥0.25 mcg/kg/min |
| Dopamine | Strongly recommended AGAINST |
| Peripheral vasopressors | NOW acceptable (new SSC 2021) |
| Antibiotics (shock) | Within 1 hour |
| Antibiotics (sepsis, no shock) | Within 3 hours (new SSC 2021) |
| Corticosteroids threshold | NE ≥0.25 mcg/kg/min for ≥4 hours (new SSC 2021) |
| Steroid regimen | Hydrocortisone 200 mg/day continuous infusion |
| Blood glucose target | 144-180 mg/dL (NOT tight control) |
| SOFA components | Respiratory, Coagulation, Liver, Cardiovascular, CNS, Renal (6 systems, 0-24) |
| SOFA ≥2 | Sepsis |
| Septic shock SOFA cardiovascular | Vasopressor requirement (score 2-4) |
- Sabiston Textbook of Surgery, 11e (shock classification, SOFA, sepsis definitions, vasopressors, ADRENAL)
- Barash's Clinical Anesthesia, 9e (types of shock, haemodynamic profiles)
- Harrison's Principles of Internal Medicine, 22e (shock classification table)
- Evans L et al. SSC 2021 Guidelines - Crit Care Med 2021; PMID 34605781
- Singer M et al. Sepsis-3 Definitions - JAMA 2016 (SOFA, qSOFA)
- SOAP II Trial (dopamine vs norepinephrine)
- SEPSISPAM Trial (MAP 65 vs 80)
- SMART/SALT-ED Trials (balanced vs saline)
- ANDROMEDA-SHOCK Trial (capillary refill time)
- ADRENAL + APROCCHSS Trials (corticosteroids)
- Ranzani OT et al. SOFA-2 Score - JAMA 2025; PMID 41159833
Write a short note on high flow nasal cannula for md anaesthesia exa, . Also with possible neet ss critical carequestions .
high flow nasal cannula HFNC mechanism advantages indications contraindications post-extubation FLORALI trial 2024
high flow nasal cannula HFNC acute hypoxemic respiratory failure intubation mortality
https://pmc.ncbi.nlm.nih.gov/articles/PMC11375959
HFNC high flow nasal cannula ROX index failure prediction intubation FLORALI post-extubation
ROX index HFNC failure prediction formula SpO2/FiO2 respiratory rate 2.85 threshold intubation cutoff
HFNC FLORALI trial results high risk extubation post-extubation NIV vs HFNC reintubation Hernandez 2016 comparison
HIGH FLOW NASAL CANNULA (HFNC) OXYGEN THERAPY
Short Note for MD Anaesthesia Examination | NEET SS Critical Care
INTRODUCTION
COMPARISON: CONVENTIONAL OXYGEN vs HFNC
| Parameter | Conventional Low-Flow O₂ | HFNC |
|---|---|---|
| Flow rate | 1-15 L/min | 20-60 L/min |
| FiO₂ accuracy | Variable (dilution with room air) | Fixed, accurate 0.21-1.0 |
| Humidification | None/minimal | Active heated humidification (37°C, 100% RH) |
| PEEP effect | None | Generates 2-7 cmH₂O (flow-dependent) |
| Dead space washout | Nil | Significant |
| Patient comfort | Low-medium | High (warm, humidified, no tight seal) |
| CO₂ clearance | No | Modest improvement |
EQUIPMENT / COMPONENTS OF HFNC SYSTEM
- Blender - mixes air and oxygen to achieve precise FiO₂ (0.21-1.0)
- High-flow flowmeter - drives gas at up to 60 L/min
- Active heated humidifier (Fisher & Paykel Optiflow/Airvo) - heats gas to 37°C with 100% relative humidity
- Heated breathing circuit/tubing - prevents condensation
- Wide-bore nasal prongs (soft, large-bore; fit both nares snugly but NOT airtight)
MECHANISMS OF ACTION (PHYSIOLOGICAL EFFECTS)
1. Accurate and High FiO₂ Delivery
- Conventional NC/mask: patient's peak inspiratory flow (15-30 L/min) exceeds device flow → room air entrained → FiO₂ diluted and unpredictable
- HFNC at 40-60 L/min: exceeds or matches peak inspiratory flow → minimal room air entrainment → stable, accurate FiO₂ as set
- FiO₂ set on blender = FiO₂ delivered to alveoli (reliable)
- Higher flow = higher FiO₂ accuracy
2. Dead Space Washout (Nasopharyngeal CO₂ Clearance)
- High continuous gas flow washes out the anatomical dead space in nasopharynx and proximal tracheobronchial tree (~150 mL)
- Reduces CO₂ rebreathing at onset of inspiration (fresh oxygen fills dead space between breaths)
- Improves alveolar ventilation efficiency without increasing minute ventilation
- Net effect: Reduces PaCO₂ modestly; reduces work of breathing
3. Positive End-Expiratory Pressure (PEEP) Effect
- High flow through nasal prongs against the upper airway resistance generates positive nasopharyngeal pressure
- This transmits as a modest PEEP of 2-7 cmH₂O (flow-dependent; ~1 cmH₂O per 10 L/min with mouth closed)
- PEEP effect increases with: higher flow rate + closed mouth
- Effects of PEEP: prevents alveolar collapse, recruits microatelectasis, increases functional residual capacity (FRC by ~25%)
4. Reduction in Work of Breathing (WOB)
- High-flow delivery reduces patient's inspiratory effort (less effort needed to generate tidal flow)
- Heated humidification reduces mucosal irritation and bronchospasm from cold/dry gas
- Reduces accessory muscle activation and tachypnoea
- Reduces respiratory drive by improving gas exchange
5. Heated Humidification
- Gas delivered at 37°C, 100% relative humidity (isothermal saturation boundary)
- Prevents drying of mucosa → better mucociliary clearance → easier secretion expectoration
- Reduces bronchospasm from cold/dry gas
- Critical difference from conventional O₂ therapy (comfort and compliance)
6. Reduced Inspiratory Resistance / Improved Comfort
- No tight-fitting mask → no claustrophobia → better tolerance
- Patient can speak, eat, and expectorate
- Better compliance vs NIV masks (particularly in agitated or anxious patients)
SETTINGS AND HOW TO INITIATE HFNC
| Parameter | Starting | Titration | Range |
|---|---|---|---|
| Flow rate | 30-40 L/min | Increase to 60 L/min if tolerated | 20-60 L/min |
| FiO₂ | 0.5-0.6 (start) or 1.0 in emergency | Titrate down to SpO₂ target | 0.21-1.0 |
| Temperature | 37°C (31-37°C range) | Most tolerate 37°C | 31-37°C |
| SpO₂ target | 92-96% | 88-92% in COPD/hypercapnic | 88-96% |
INDICATIONS FOR HFNC
A. Established / Strong Indications
| Indication | Evidence |
|---|---|
| Acute hypoxaemic respiratory failure (AHRF) | FLORALI trial; strong recommendation; reduces intubation by 30-50% vs conventional O₂ in mild-moderate AHRF |
| Post-extubation support - LOW risk | Hernandez 1 (JAMA 2016) - HFNC superior to conventional O₂ in LOW-risk extubation |
| Post-extubation support - HIGH risk (non-hypercapnic) | Hernandez 2 (JAMA 2016) - HFNC non-inferior to NIV; NIV preferred if hypercapnia present |
| Peri-intubation/Pre-oxygenation | HFNC during intubation extends apnoeic safe time (THRIVE principle) |
| Apnoeic oxygenation during intubation | Continues O₂ delivery during laryngoscopy; extends apnoea tolerance |
| Post-operative respiratory failure | Particularly after cardiac/thoracic surgery; non-inferior to NIV |
| Immunocompromised patients with AHRF | HIGH trial; comfort and less mask complications |
| COVID-19 hypoxaemia | Widely used; reduces NIV/intubation need |
B. Other Indications
- Do-not-intubate (DNI) patients: Comfort and palliation while providing oxygen support
- Bronchoscopy/Procedures: Maintains oxygenation during diagnostic/therapeutic bronchoscopy
- Mild COPD exacerbation: May be used when NIV not tolerated (see hypercapnia caveat below)
- Obstructive sleep apnoea: Some benefit between CPAP sessions
- Paediatric respiratory failure: Bronchiolitis (PARIS trial, 2018 - HFNC vs standard O₂)
CONTRAINDICATIONS
Absolute:
- Apnoea or respiratory arrest (needs immediate intubation)
- Severe facial deformity/trauma preventing prong fitting
- Absent airway reflexes / impaired consciousness (risk of aspiration)
Relative:
- Severe hypercapnia (PaCO₂ >60 mmHg, pH <7.25) - HFNC does not provide the ventilatory support of NIV; use NIV preferentially
- Severe haemodynamic instability requiring intubation
- Active epistaxis or nasal obstruction
- Gastric aspiration risk in vomiting, ileus
- Pneumothorax not drained
KEY CLINICAL TRIALS
1. FLORALI Trial (Frat et al., NEJM 2015) - MOST IMPORTANT
| Outcome | HFNC | Standard O₂ | NIV |
|---|---|---|---|
| Intubation (overall, day 28) | 38% | 47% | 50% (not significant) |
| Intubation (PF ≤200 subgroup) | 35% | 53% | 58% (p=0.009) |
| Ventilator-free days | 24 | 22 | 19 (p=0.02) |
| ICU mortality | 11% | 19% | 25% |
| 90-day mortality | 12% | 23% (HR 2.01, p=0.046) | 28% (HR 2.50, p=0.006) |
- Primary endpoint not significant overall
- In moderate-severe AHRF (PF ≤200): HFNC significantly reduced intubation
- HFNC significantly improved 90-day survival vs both standard O₂ AND NIV
- HFNC superior to NIV for non-hypercapnic AHRF
2. Hernandez 1 Trial (Hernandez et al., JAMA 2016) - Post-Extubation, LOW Risk
3. Hernandez 2 Trial (Hernandez et al., JAMA 2016) - Post-Extubation, HIGH Risk
4. THRIVE (Transnasal Humidified Rapid Insufflation Ventilatory Exchange - Patout 2015/Gustafsson 2017)
- Demonstrated apnoeic oxygenation with HFNC during general anaesthesia
- HFNC at 70 L/min during laryngoscopy: extended safe apnoea time to >14 minutes without desaturation
- Mechanism: Apnoeic oxygenation + bulk gas flow removes CO₂ from dead space
- Widely adopted for peri-intubation preoxygenation and difficult airway management
ROX INDEX - PREDICTING HFNC FAILURE (KEY EXAM TOPIC)
| ROX Index | Time Point | Meaning |
|---|---|---|
| ≥4.88 at 2, 6, and 12 hours | All timepoints | Associated with LOWER risk of intubation (HFNC likely to succeed) |
| <2.85 at 2 hours | 2h | High risk of HFNC failure |
| <3.47 at 6 hours | 6h | High risk of failure |
| <3.85 at 12 hours | 12h | 100% predictive of failure → urgent ICU consultation |
| 3.85-4.88 at 12h | 12h | Indeterminate zone → clinical judgement |
- Measure ROX index at 2, 6, and 12 hours after HFNC initiation
- Trending is more important than a single value
- Falling ROX = deteriorating; rising ROX = improving
- AUC at 12 hours = 0.759 (reasonable discrimination)
- Original study in community-acquired pneumonia; not fully validated for all AHRF causes
- Does not replace clinical assessment (work of breathing, mental status, haemodynamics)
- Never delay intubation when clinical signs indicate impending decompensation, regardless of ROX score
SIGNS OF HFNC FAILURE - WHEN TO ESCALATE
| Sign | Threshold |
|---|---|
| Respiratory rate | >35/min persisting |
| SpO₂ | <90% despite FiO₂ 1.0 and flow 60 L/min |
| Worsening dyspnoea/distress | Clinical judgement |
| Accessory muscle use | Paradoxical breathing |
| Altered mental status | Agitation, confusion |
| Haemodynamic instability | Deteriorating |
| Rising PaCO₂ | pH <7.25 |
| ROX index <3.85 at 12 hours | Tool-based trigger |
ADVANTAGES OF HFNC OVER NIV
| Advantage | HFNC | NIV |
|---|---|---|
| Comfort/Tolerance | Excellent (no mask) | Poor (claustrophobia, pressure sores) |
| Patient communication | Possible (talk, eat, drink) | Limited |
| Secretion clearance | Better (humidification, can cough freely) | Impaired by mask |
| Gastric insufflation risk | Lower | Higher (especially when poorly fitting) |
| Complexity of setup | Simpler | Complex (mask fitting, leak management) |
| Skin pressure injury | None | Facial pressure ulcers common |
| In immunocompromised patients | Preferred (avoids mask-associated infections) | Higher infection risk from mask secretions |
| Hypercapnia management | Modest CO₂ clearance | Superior (active ventilation) |
ADVANTAGES OF HFNC OVER CONVENTIONAL OXYGEN THERAPY
- Higher and more reliable FiO₂ delivery (no dilution)
- Active PEEP generation (2-7 cmH₂O) prevents atelectasis
- Dead space washout → better CO₂ clearance
- Heated humidification → mucosal comfort, secretion clearance
- Reduces work of breathing
- Better tolerance and compliance
- Possible mortality benefit in moderate-severe AHRF (FLORALI)
SPECIAL USES IN ANAESTHESIA
1. Peri-Intubation Oxygenation (Apnoeic Oxygenation)
- Apply HFNC at 15-70 L/min during laryngoscopy/intubation
- Continues oxygen delivery via nasal route while jaw is held open
- Mechanism: Bulk flow of O₂ down pressure gradient from nasopharynx to alveoli even without diaphragmatic effort (apnoeic oxygenation)
- THRIVE study: apnoea time extended significantly
- DAS guidelines / DIFFICULT AIRWAY management: HFNC during RSI/difficult airway management is now standard
2. Pre-Oxygenation Before Induction
- HFNC at 60 L/min FiO₂ 1.0 for 3-5 minutes before induction
- Better pre-oxygenation (higher ETO₂) than face mask in obese patients
- In patients with AHRF: allows adequate denitrogenation without worsening distress
3. Intra-Procedural Sedation (Procedural Oxygenation)
- Used during bronchoscopy, GI endoscopy, cardioversion under sedation
- Maintains oxygenation throughout the procedure
- Reduces risk of desaturation during bolus sedation/airway obstruction
4. Post-Operative Respiratory Support
- After cardiac/thoracic/abdominal surgery
- Particularly useful in obese patients (high risk of atelectasis)
- Reduces post-operative pulmonary complications (atelectasis, pneumonia)
- OPERA trial: HFNC vs conventional O₂ post-extubation cardiac surgery - reduced post-extubation respiratory failure at 30 min
WEANING FROM HFNC
- Reduce FiO₂ first (towards 0.21) while maintaining flow
- Then reduce flow rate (from 60 → 40 → 30 → 20 L/min)
- When flow ≤20 L/min and FiO₂ ≤0.3: trial on conventional nasal cannula
- Assess at each step-down: SpO₂, RR, WOB, patient comfort
- Do not rush weaning - premature step-down leads to re-escalation
HFNC IN HYPERCAPNIC RESPIRATORY FAILURE (COPD) - CURRENT POSITION
- HFNC has modest CO₂-clearance through dead space washout
- Not equivalent to NIV for hypercapnic failure
- Tan et al. RCT (Crit Care 2024): HFNC non-inferior to NIV for acute-moderate hypercapnia in COPD (pH 7.25-7.35, PaCO₂ <65) - may be acceptable alternative when NIV intolerated
- Strong hypercapnia (pH <7.25 or PaCO₂ >65): NIV preferred; HFNC insufficient
- Meta-analysis (Ovtcharenko et al., Crit Care 2022; Fahey et al., 2023): HFNC similar to NIV for treatment failure, intubation in hypercapnic AHRF; caution needed in severe cases
ADVERSE EFFECTS AND LIMITATIONS
| Adverse Effect | Details |
|---|---|
| Delayed intubation | Most dangerous - false reassurance from SpO₂ maintenance with HFNC masking worsening failure |
| Hypercapnia | If hypercapnic patient worsens on HFNC - CO₂ clearance insufficient |
| Gastric insufflation | Less than NIV but can occur with very high flows |
| Nasal dryness/discomfort | Reduce temperature or flow |
| Noise | High-flow hiss; patient complaint |
| P-SILI risk | Patient Self-Inflicted Lung Injury if strong respiratory drive + HFNC "masks" worsening failure |
| Aerosol generation | COVID-19 concern - isolate patient; surgical mask over HFNC prongs reduces aerosol spread |
| Cost | Higher than conventional O₂ |
HFNC vs NIV vs INTUBATION - DECISION FRAMEWORK
ACUTE HYPOXAEMIC RESPIRATORY FAILURE
↓
ASSESS SEVERITY
↓
PF >300: Conventional O₂
↓
PF 150-300 (Mild-Moderate):
HFNC first choice
(FLORALI, better tolerated than NIV)
↓
PF <150 (Moderate-Severe):
HFNC (if not hypercapnic)
NIV if hypercapnic/CHF/COPD dominant
↓
MONITOR ROX INDEX at 2, 6, 12 hours
↓
ROX <3.85 at 12h OR clinical deterioration
→ Prepare for intubation
↓
PF <80 after all measures → ECMO referral
NEET SS CRITICAL CARE MCQs: HFNC
- A) FiO₂ accuracy
- B) Dead space washout
- C) PEEP effect (nasopharyngeal positive pressure increases significantly with mouth closed)
- D) Mucosal humidification
- A) PaO₂/FiO₂ ratio
- B) (SpO₂/FiO₂) ÷ Respiratory Rate
- C) (PaO₂/FiO₂) × PEEP
- D) Respiratory Rate ÷ FiO₂
- A) Primary endpoint of intubation by day 28 was significantly lower in HFNC than NIV
- B) In patients with PaO₂/FiO₂ ≤200, intubation rate was significantly lower with HFNC (35%) vs standard O₂ (53%) vs NIV (58%)
- C) HFNC had no mortality benefit over NIV
- D) HFNC was inferior to NIV for all patients with AHRF
- A) 62-year-old with COPD exacerbation, pH 7.22, PaCO₂ 72 mmHg
- B) 45-year-old with community-acquired pneumonia, PF ratio 170, SpO₂ 87% on Venturi mask 60%, haemodynamically stable, alert
- C) A patient with respiratory arrest requiring immediate intubation
- D) 78-year-old with severe heart failure, PF ratio 90, pH 7.30, PaCO₂ 55 mmHg
- A) Positive pressure generation forcing CO₂ out of alveoli
- B) High FiO₂ increasing oxygen to replace CO₂ in alveoli
- C) Continuous high-flow washout of anatomical dead space (nasopharynx and proximal airways), reducing CO₂ rebreathing and improving alveolar ventilation efficiency
- D) Diaphragmatic stimulation increasing ventilatory drive
- A) The positive pressure pushes oxygenated gas into alveoli during apnoea
- B) Bulk flow of oxygen down the pressure gradient from the nasopharynx to alveoli via apnoeic oxygenation, combined with CO₂ washout from dead space
- C) HFNC activates the Hering-Breuer reflex, preventing apnoea
- D) Warming prevents oxygen desaturation by improving haemoglobin-oxygen affinity
- A) HFNC is always superior to NIV in all high-risk post-extubation patients
- B) HFNC is non-inferior to NIV in general high-risk patients; but NIV may be superior in VERY high-risk patients, especially with hypercapnia, COPD, or CHF
- C) Standard oxygen therapy is preferred over HFNC for post-extubation in high-risk patients
- D) HFNC should not be used post-extubation in any patient with COPD
- A) 0-1 cmH₂O
- B) 10-15 cmH₂O
- C) 4-7 cmH₂O
- D) 15-20 cmH₂O
- A) Lower patient comfort
- B) Greater risk of facial pressure sores
- C) Inability to provide active inspiratory pressure support to unload the respiratory muscles as effectively as NIV
- D) Higher risk of gastric insufflation
- A) It prevents bronchospasm by delivering heated gas
- B) It maintains reliable oxygenation throughout the procedure despite partial airway obstruction by the bronchoscope, without requiring intubation
- C) It provides general anaesthesia equivalent to propofol
- D) It prevents bleeding from mucosal biopsies
RAPID REVISION TABLE
| Feature | Key Value |
|---|---|
| HFNC max flow rate | 60 L/min |
| HFNC FiO₂ range | 0.21-1.0 (accurate, fixed) |
| HFNC temperature | 37°C, 100% relative humidity |
| PEEP generated | ~1 cmH₂O per 10 L/min (mouth closed) |
| PEEP at 60 L/min | 4-7 cmH₂O |
| Dead space washout | ~150 mL nasopharyngeal dead space cleared |
| ROX formula | (SpO₂/FiO₂) ÷ RR |
| ROX success threshold | ≥4.88 at 2, 6, 12 hours |
| ROX failure at 12h | <3.85 (100% predictive failure) |
| FLORALI trial | HFNC superior in PF ≤200; improved 90-day mortality |
| THRIVE technique | Apnoeic oxygenation at 70 L/min; >14 min safe apnoea |
| Starting flow | 30-40 L/min, titrate to 60 |
| SpO₂ target | 92-96% (88-92% in COPD) |
| HFNC vs NIV | Non-inferior post-extubation (general high-risk); NIV superior if hypercapnia |
| Post-extubation very high-risk | NIV preferred over HFNC (2022 RCT: 23.3% vs 38.8% reintubation) |
| Weaning: first step | Reduce FiO₂ first, then reduce flow |
| Contraindications | Apnoea, severe hypercapnia (pH<7.25), impaired consciousness |
| Main risk | Delayed intubation (false security from maintained SpO₂) |
- Barash's Clinical Anesthesia, 9e (THRIVE reference)
- Frat JP et al. FLORALI Trial - NEJM 2015 (HFNC vs NIV vs standard O₂ in AHRF)
- Hernandez G et al. - JAMA 2016 (Post-extubation high-risk: HFNC vs NIV)
- Roca O et al. ROX Index - Am J Respir Crit Care Med 2019
- Gustafsson IM et al. THRIVE - Br J Anaesth 2017 (apnoeic oxygenation)
- Comprehensive Review on HFNC - PMC 2024
- Tan D et al. HFNC vs NIV in COPD hypercapnia - Crit Care 2024; PMID 39026242
- Ovtcharenko N et al. HFNC vs NIV meta-analysis - Crit Care 2022; PMID 36352457