Pulmonary hypertension
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"pulmonary hypertension"[MeSH Terms] AND classification
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content. Let me compile the summary.
Pulmonary Hypertension — Overview
Definition
Pulmonary hypertension (PH) is defined as a mean pulmonary artery pressure (mPAP) > 20 mm Hg, measured by right heart catheterization (RHC). This threshold was updated at the 6th World Symposium on Pulmonary Hypertension (WSPH); the previous cutoff of 25 mm Hg was considered arbitrary. Normal mPAP is 14 ± 3.3 mm Hg, so >20 mm Hg represents the 97.5th percentile (>2 SD above normal). Even mildly elevated mPAP (21–24 mm Hg) is associated with increased all-cause mortality (RR 1.5).
— Murray & Nadel's Textbook of Respiratory Medicine
Hemodynamic Classification (6th WSPH)
| Category | mPAP | PCWP | PVR | WHO Groups |
|---|---|---|---|---|
| Normal | 14 ± 3.3 mm Hg | — | — | — |
| Precapillary PH | >20 mm Hg | ≤15 mm Hg | ≥3 WU | 1, 3, 4, 5 |
| Isolated postcapillary PH | >20 mm Hg | >15 mm Hg | <3 WU | 2, 5 |
| Combined pre- + postcapillary PH | >20 mm Hg | >15 mm Hg | ≥3 WU | 2, 5 |
WU = Wood units; PCWP = pulmonary capillary wedge pressure
WHO Clinical Classification (5 Groups)
| Group | Category | Key Examples |
|---|---|---|
| 1 | Pulmonary arterial hypertension (PAH) | Idiopathic (~50%), CTD-associated (~25%), heritable, drug-/toxin-induced, HIV, portal HTN, CHD, schistosomiasis |
| 2 | PH due to left heart disease | HFrEF, HFpEF, valvular disease |
| 3 | PH due to lung disease / hypoxia | COPD, ILD, sleep apnea |
| 4 | PH due to pulmonary artery obstruction | Chronic thromboembolic PH (CTEPH) |
| 5 | PH with unclear/multifactorial mechanisms | Sarcoidosis, histiocytosis, metabolic disorders |
Left heart disease (Group 2) is the most common form of PH in community studies; idiopathic PAH is the rarest.
Pathophysiology
Three core mechanisms drive increased pulmonary vascular resistance (PVR):
1. Vasoconstriction
- Hypoxia triggers intrinsic pulmonary arterial smooth muscle cell (PASMC) contraction — even without endothelium.
- Reduced shear stress → ↓ nitric oxide (NO) production → impaired vasodilation → enhanced vasoconstriction.
- Serotonin and thromboxane from activated platelets amplify vasoconstriction.
2. Vascular Remodeling
- Medial thickening: PASMC proliferation and hypertrophy in small pulmonary arteries and arterioles.
- Intimal proliferation: Fibrosis and concentric laminar thickening, narrowing/obliterating the vessel lumen.
- Plexiform lesions: Aneurysmatic dilations of small arteries filled with proliferating endothelial cells, SMCs, and myofibroblasts — hallmark of severe PAH. Found in IPAH, CHD-associated PAH, HIV, liver cirrhosis, and scleroderma.
- Increased arterial stiffness: Accelerated extracellular matrix turnover (e.g., tenascin-C upregulation) raises PVR independently of smooth muscle tone.
- Growth factors driving remodeling include PDGF, TGF-β, and VEGF from platelets and endothelial cells.
3. In Situ Thrombosis
- Monoclonal endothelial proliferation + platelet activation → local pro-coagulant shift within small vessels.
- Occurs without a remote embolic source, distinguishing it from thromboembolic PH (Group 4).
- Shear stress from elevated pressure further activates endothelium toward a procoagulant phenotype.
Downstream consequence
Rising PVR imposes progressive pressure overload on the right ventricle (RV) → RV hypertrophy → cor pulmonale. Coronary blood flow may fail to meet increased RV metabolic demand, causing right ventricular ischemia — the mechanism of substernal chest pain in PH. Dilation of the pulmonary trunk can also compress the left main coronary artery.
Epidemiology
- Affects all ages and races; women > men (most pronounced in PAH).
- PAH prevalence: ~15–50 per million persons.
- Overall PH prevalence: ~100–127 per 100,000 (Canada data); rising due to increasing HFpEF and sleep apnea.
— Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders
Explore diagnostic tests (echo, RHC, labs) for PH
Finding Sources
Finding Sources
Searching PubMed
"pulmonary hypertension"[MeSH Terms] AND diagnosis[MeSH Terms]
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent data collected. Here is the comprehensive diagnostic overview:
Diagnostic Tests for Pulmonary Hypertension
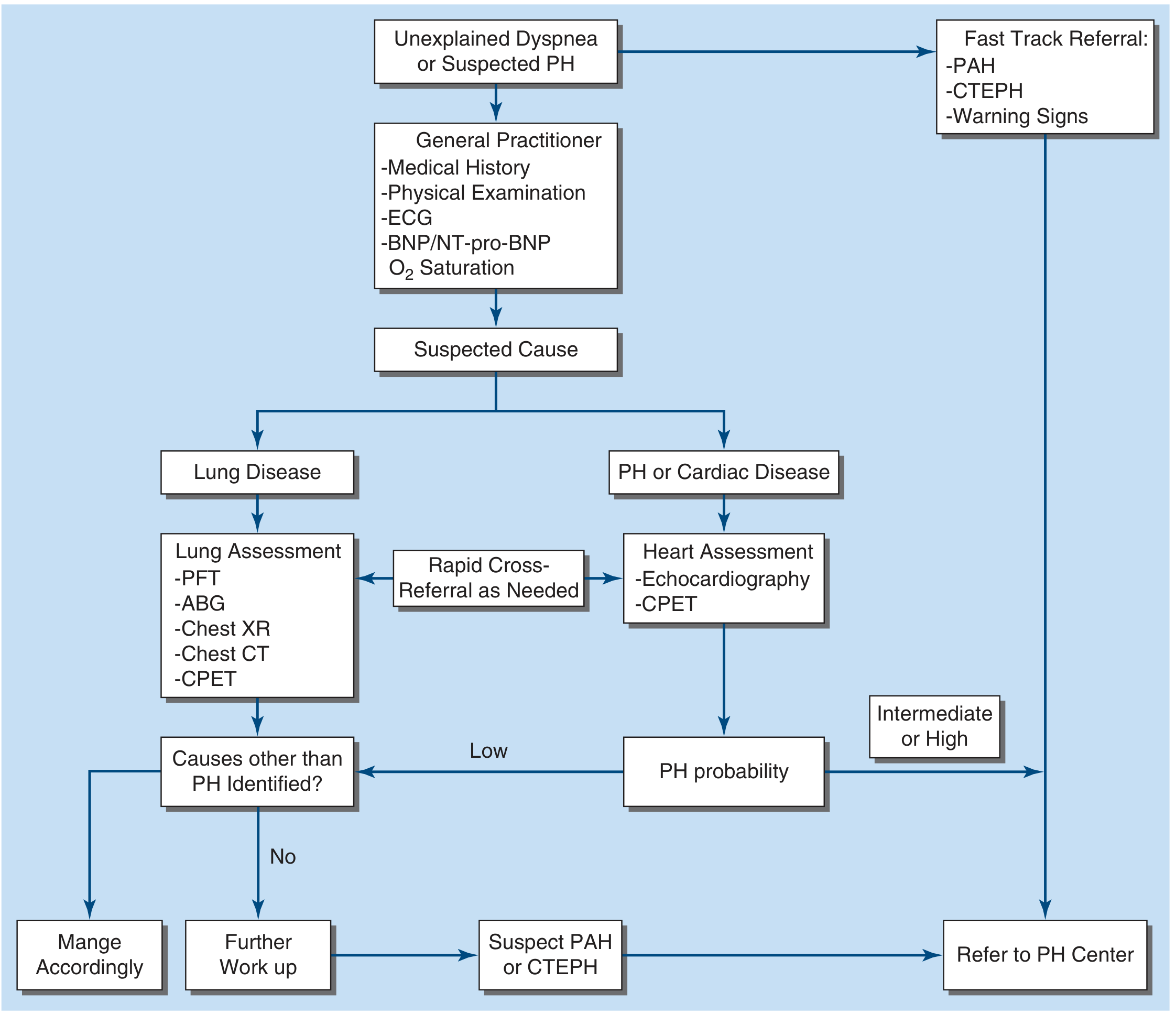
Diagnostic Pathway
Step 1 — Initial screen (GP/first contact): History, physical exam, ECG, BNP/NT-proBNP, O₂ saturation
Step 2 — Non-invasive imaging: Echocardiogram ± chest X-ray, PFTs, CT
Step 3 — Confirmatory: Right heart catheterization (RHC) ± vasoreactivity testing
1. Echocardiography — First-Line Screen
Echocardiography is the best initial noninvasive test for evaluating suspected PH.
Quantitative estimation of PAP
- Tricuspid regurgitant (TR) jet velocity measured by Doppler
- Modified Bernoulli equation: RVSP = 4v² + RAP (v = TR jet velocity in m/s)
- RVSP is assumed equal to PASP when the pulmonic valve is normal
- Normal RVSP: 28 ± 5 mm Hg; screening echo suggests PH when PASP > 40 mm Hg (Goldman-Cecil) or peak TRv > 2.8 m/s (echocardiography textbook)
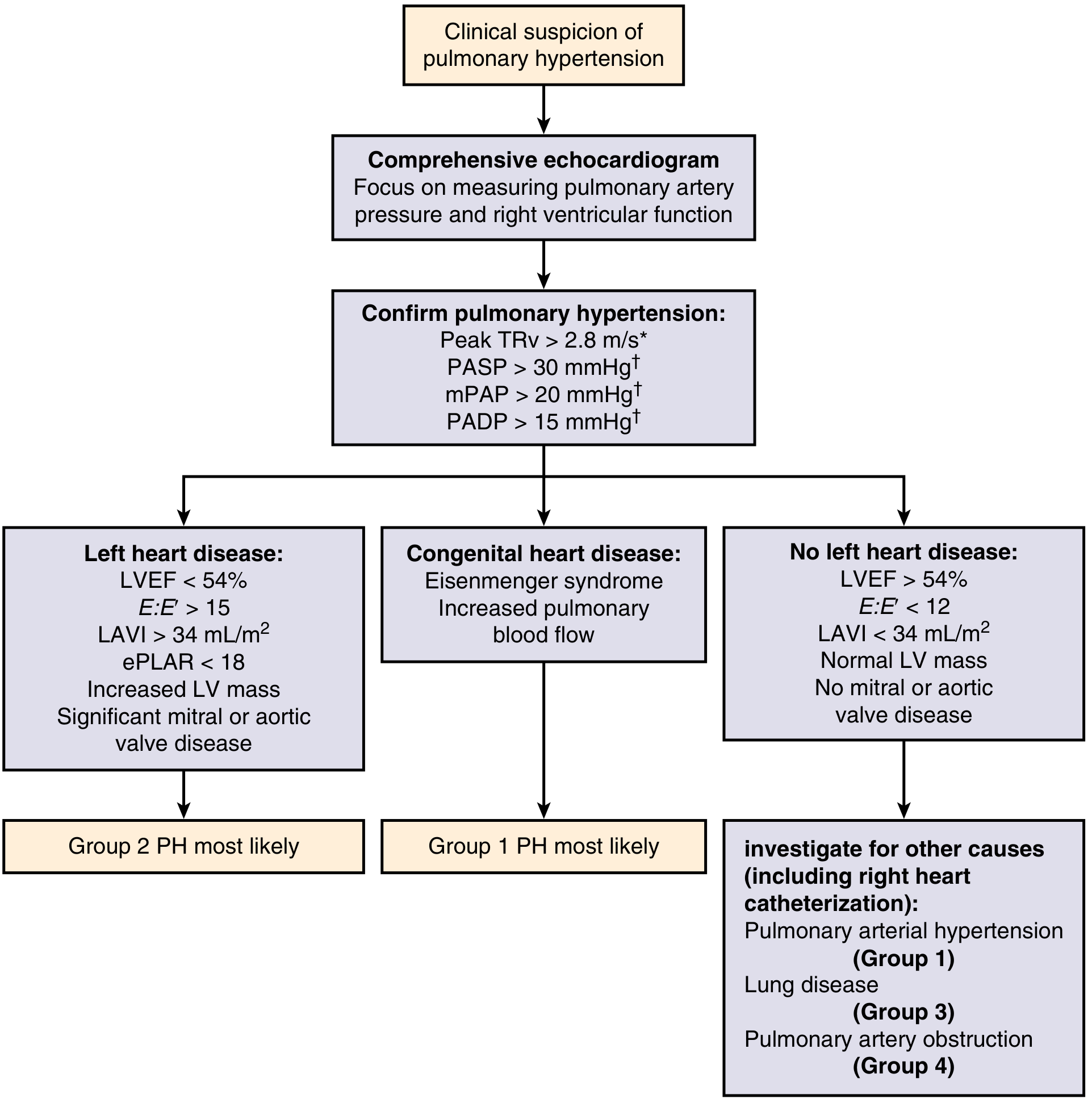
Echocardiographic PH thresholds (6th WSPH–aligned):
| Parameter | Threshold suggesting PH |
|---|---|
| Peak TR velocity | > 2.8 m/s |
| PASP | > 30 mm Hg |
| mPAP | > 20 mm Hg |
| PADP | > 15 mm Hg |
Qualitative 2D features of elevated PAP
- Right atrial (RA) enlargement
- Right ventricular (RV) enlargement
- Flattening of the interventricular septum ("D-sign")
- Underfilled left ventricle
- Pericardial effusion (marker of high risk; RA area >26 cm² = high-risk)
Etiological clues on echo
Echo differentiates WHO groups by showing:
| Finding | Likely Group |
|---|---|
| LVEF <54%, E:E' >15, LAVI >34 mL/m², mitral/aortic valve disease | Group 2 (LHD) |
| Eisenmenger syndrome, intracardiac shunt | Group 1 (CHD-associated PAH) |
| Normal LV, LVEF >54%, E:E' <12 | Groups 1, 3, 4 — needs RHC |
| Thrombus in RA/RV/PA, tricuspid vegetation | Group 4 (CTEPH) |
Limitation: Echo is unreliable in parenchymal lung disease/hyperinflation; correlation with RHC is imperfect. In ~25% of patients with severe PAH, a patent foramen ovale can shunt right→left, worsening hypoxia.
2. Right Heart Catheterization — Gold Standard
RHC is virtually always required to:
- Confirm the diagnosis of PH (mPAP >20 mm Hg)
- Classify hemodynamic subtype (pre- vs. postcapillary)
- Assess severity (PVR, cardiac index, RAP, SvO₂)
- Guide therapy
Key hemodynamic parameters measured at RHC
| Parameter | Normal | Significance |
|---|---|---|
| mPAP | 14 ± 3.3 mm Hg | >20 mm Hg = PH |
| PCWP | 8 ± 2.9 mm Hg | >15 mm Hg = postcapillary |
| PVR | 0.93 ± 0.38 WU | ≥3 WU = precapillary (PAH) |
| Cardiac index (CI) | ≥2.5 L/min/m² | <2.0 = high-risk |
| RAP | <8 mm Hg | >14 = high-risk |
| Mixed venous O₂ saturation (SvO₂) | >65% | <60% = high-risk |
Acute Vasoreactivity Testing (during RHC)
- Who: Indicated at initial RHC for idiopathic, hereditable, or drug-induced PAH only
- Agents: Inhaled nitric oxide, IV adenosine, or IV epoprostenol (short-acting)
- Positive response: ↓mPAP by ≥10 mm Hg to an absolute mPAP ≤40 mm Hg, with stable or improved cardiac output
- Significance: ~10% of IPAH patients are acute responders; ~50% of these sustain long-term benefit with oral calcium channel blockers (CCBs) — with 5-year survival ~94%
- ⚠️ CCBs must NOT be given without documented vasoreactivity — can cause hypotension, ↓ CO, arrhythmia, and death in non-responders
3. Laboratory Tests
Biomarkers
| Test | Interpretation |
|---|---|
| NT-proBNP / BNP | Frequently elevated in PH; reflects RV pressure overload. Normal does NOT exclude PH. Used for risk stratification: BNP <50 ng/L = low risk; BNP >300 ng/L = high risk |
| Uric acid | Elevated in severe PH — reflects tissue hypoxia |
Connective tissue disease / etiology workup
| Test | Target condition |
|---|---|
| ANA, anti-Scl-70, anti-centromere | Systemic sclerosis (most common CTD-PAH) |
| Anti-dsDNA, anti-Smith | SLE |
| RF, anti-CCP | RA |
| HIV serology | HIV-associated PAH |
| Liver function tests, hepatitis serology | Portal hypertension (portopulmonary HTN) |
| CBC, peripheral smear | Hemolytic anemia (Group 5), polycythemia |
| Thyroid function | Thyroid disease (Group 5) |
| Coagulation screen, antiphospholipid antibodies | CTEPH (Group 4) |
4. Additional Non-Invasive Tests
ECG
- Right axis deviation
- RV hypertrophy (R > S in V1)
- Right atrial enlargement ("P pulmonale" — peaked P in lead II)
- ST/T changes in anterior precordium (RV strain pattern)
- ⚠️ Normal ECG does NOT exclude PH
Chest X-ray
- Enlarged proximal pulmonary arteries
- Peripheral vascular "pruning" (reduced peripheral vasculature)
- Right ventricular enlargement (reduced retrosternal air space on lateral view)
- ⚠️ Normal CXR does NOT exclude PH
V/Q Scan
- Study of choice to exclude CTEPH (Group 4)
- Shows mismatched perfusion defects (perfusion deficit without corresponding ventilation deficit)
- CT-PA may miss chronic thromboembolic disease — V/Q is preferred for CTEPH screening
Pulmonary Function Tests (PFTs)
- PAH: mild restrictive pattern or mild ↓ DLCO
- Group 3 PH: obstructive (COPD) or restrictive (ILD) pattern
- Helps differentiate lung disease–related PH
CT Chest / HRCT
- Identifies parenchymal lung disease (Group 3)
- Can show dilated central PAs, RV enlargement
- CT-PA: useful for acute PE but less sensitive for chronic CTEPH than V/Q
Cardiopulmonary Exercise Testing (CPET)
- ↓ Peak VO₂ and elevated VE/VCO₂ slope reflect impaired RV reserve
- Used in risk stratification: PeakVO₂ <11 mL/min/kg = high risk
Risk Stratification Summary (ESC/ERS, at RHC)
| Parameter | Low Risk (<5% 1-yr mortality) | Intermediate (5–10%) | High Risk (>10%) |
|---|---|---|---|
| WHO Functional Class | I–II | III | IV |
| 6-min walk distance | >440 m | 165–440 m | <165 m |
| NT-proBNP | <300 ng/L | 300–1400 ng/L | >1400 ng/L |
| RA area (echo) | <18 cm² | 18–26 cm² | >26 cm² |
| Pericardial effusion | None | None/minimal | Present |
| Cardiac index | >2.5 | 2.0–2.4 | <2.0 |
| RAP | <8 mm Hg | 8–14 mm Hg | >14 mm Hg |
| SvO₂ | >65% | 60–65% | <60% |
— Fishman's Pulmonary Diseases and Disorders; Goldman-Cecil Medicine; Murray & Nadel's Respiratory Medicine; Harrison's Principles 22e
This is a shared conversation. Sign in to Orris to start your own chat.