Polyphonic vs monophonic wheeze
Polyphonic vs Monophonic Wheeze
Background: What is a Wheeze?
- Murray & Nadel's Textbook of Respiratory Medicine, p. 898
Monophonic Wheeze
| Feature | Detail |
|---|---|
| Definition | A single-pitch wheeze - only one frequency/note heard at a time |
| Mechanism | One airway is narrowed or obstructed at a single site |
| Timing | Often heard throughout both inspiration and expiration |
| Cause | Focal/localized obstruction |
| Classic causes | Endobronchial tumor, aspirated foreign body, congenital bronchial anomaly, focal bronchial stenosis, carcinoid |
| Clinical significance | Localizing - points to a specific anatomical site; warrants bronchoscopic evaluation to exclude a structural lesion |
Polyphonic Wheeze
| Feature | Detail |
|---|---|
| Definition | Multiple simultaneous pitches heard together, like a chord |
| Mechanism | Many airways of different calibers narrowed simultaneously, each vibrating at its own frequency |
| Timing | Predominantly expiratory, though can be inspiratory too |
| Cause | Diffuse airway disease affecting multiple airways |
| Classic causes | Asthma, COPD, pulmonary edema ("cardiac asthma"), aspiration, bronchiolitis, cystic fibrosis, lymphangitic carcinomatosis |
| Clinical significance | Indicates generalized airflow obstruction; not localizing |
- Murray & Nadel's Textbook of Respiratory Medicine, p. 898
Head-to-Head Summary
| Feature | Monophonic | Polyphonic |
|---|---|---|
| Number of pitches | Single | Multiple simultaneous |
| Airways involved | One | Many |
| Distribution | Localized | Diffuse/scattered |
| Timing | Inspiratory and/or expiratory | Predominantly expiratory |
| Key implication | Focal structural lesion | Generalized obstructive disease |
| Typical diagnoses | Foreign body, tumor, stenosis | Asthma, COPD, pulmonary edema |
| Next step | Bronchoscopy to rule out lesion | Spirometry, bronchodilator response |
Special Notes
- Localized wheeze (which is usually monophonic) that persists despite treatment for presumed asthma should always raise suspicion for an endobronchial lesion.
- A "squawk" or "squeak" is a short late-inspiratory wheeze associated with pulmonary fibrosis, hypersensitivity pneumonitis, and bronchiolitis obliterans - distinct from typical polyphonic wheeze.
- Wheezing during forced exhalation can occur in normal individuals and is neither sensitive nor specific for asthma on its own - it is spontaneous/resting polyphonic wheeze that carries more diagnostic weight.
- A rhonchus is considered a wheeze variant with a lower pitch (similar to snoring), often related to secretions and tends to clear with coughing.
Create a diagnostic algorithm for evaluating new-onset wheeze
A clean, professional medical diagnostic algorithm flowchart for evaluating new-onset wheeze in adults. The flowchart should be vertical, on a white background with clear boxes, arrows, and color-coding. Structure: TOP BOX (dark blue header): "NEW-ONSET WHEEZE IN ADULTS" Step 1 (light blue box): "IMMEDIATE ASSESSMENT — Is this an emergency?" Branch YES (red arrow right): "Acute severe bronchospasm / Anaphylaxis / Stridor / Silent chest / Respiratory failure" → Red box: "EMERGENCY MANAGEMENT: Bronchodilators, Epinephrine (if anaphylaxis), O2, ICU" Branch NO (green arrow down): Continue algorithm Step 2 (light blue box): "CHARACTERIZE THE WHEEZE" Two sub-boxes side by side: - Left (yellow): "MONOPHONIC — Single pitch, Localized, Fixed → Suspect focal lesion" - Right (orange): "POLYPHONIC — Multiple pitches, Diffuse, Both phases → Suspect generalized disease" Step 3 (light blue box): "HISTORY & PHYSICAL" Sub-items: "Onset & triggers | Smoking history | Atopy/allergy | Medications (ACEi, beta-blockers, NSAIDs) | Occupational exposure | Positional change | Associated symptoms (cough, dyspnea, stridor)" Step 4 (light blue box): "INITIAL INVESTIGATIONS" Sub-items: "CXR | Spirometry with bronchodilator reversibility | Peak flow | Full blood count, BNP" Step 5: Large diamond decision box (light yellow): "REVERSIBLE AIRFLOW OBSTRUCTION on spirometry? (FEV1/FVC < 0.7, ≥12% + 200mL improvement post-BD)" - YES (green arrow): Green box "OBSTRUCTIVE PATTERN → Assess for Asthma vs COPD: Age, atopy, smoking, eosinophils, FeNO, methacholine challenge" - Sub-branch: "Asthma confirmed → Step-up therapy per GINA" | "COPD confirmed → GOLD strategy" - NO (blue arrow): Blue box "NON-OBSTRUCTIVE → Consider alternative diagnoses" Step 6 (blue box under NO branch): "FURTHER EVALUATION FOR WHEEZE MIMICS" Sub-items listed: "• Cardiac: BNP, Echo → Heart failure" "• Endobronchial lesion: CT chest, Bronchoscopy → Tumor, Foreign body, Carcinoid" "• Upper airway: Laryngoscopy → VCD, Angioedema, Tracheal stenosis" "• Vascular: CT angio → Pulmonary embolism, Vascular malformation" "• GI: pH monitoring → GERD" "• Other: ILD, Bronchiolitis obliterans, Aspiration" BOTTOM BOX (dark teal): "If no diagnosis after full workup → Multidisciplinary review / Specialist referral" Use color-coded boxes: dark blue for header, light blue for process steps, yellow/orange for wheeze types, green for positive findings, red for emergencies, teal for conclusion. Include directional arrows with labels YES/NO. Make it clean, readable, clinic-ready.
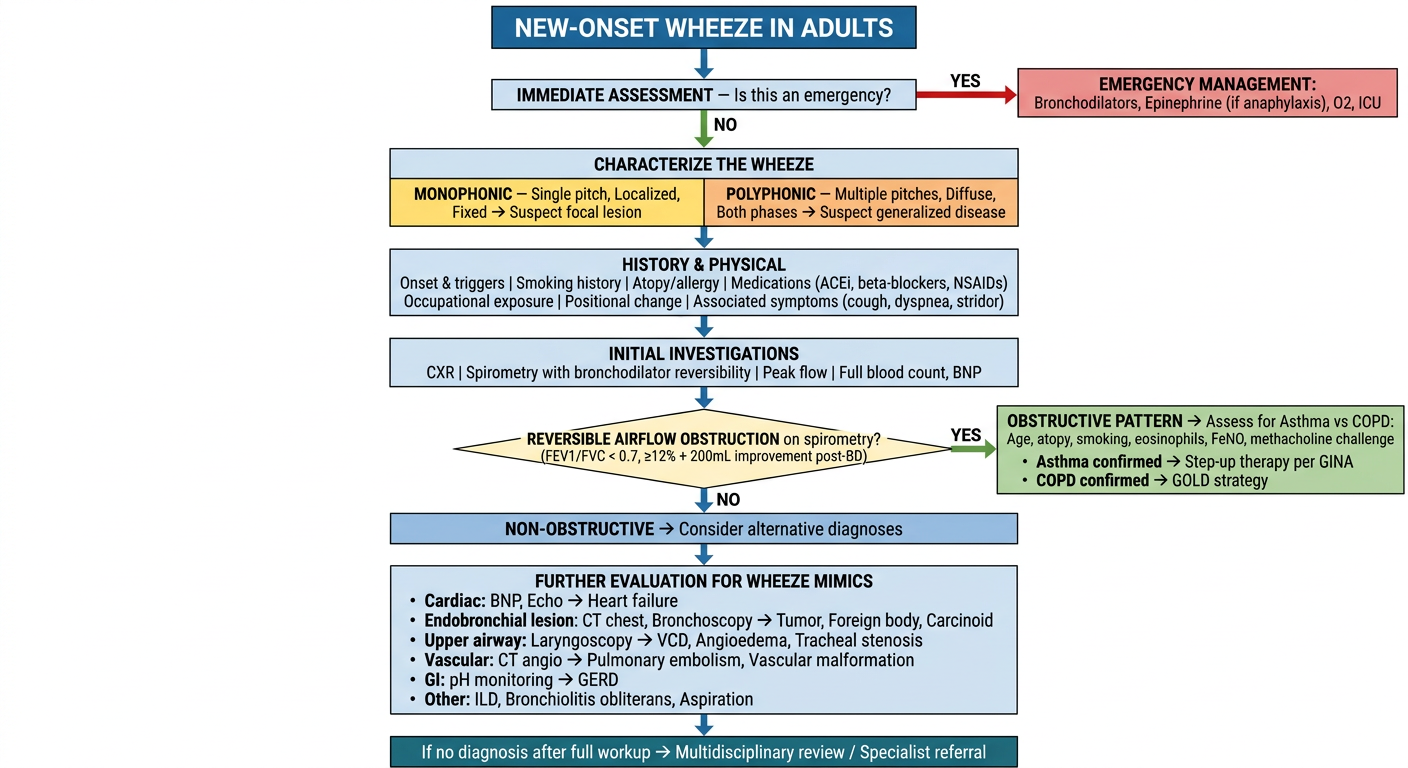
Step 1 - Emergency Triage (Do This First)
Step 2 - Characterize the Wheeze
- Monophonic + fixed + localized = single structural obstruction. Bronchoscopy is likely needed.
- Polyphonic + diffuse + expiratory-dominant = generalized airflow limitation. Think obstructive lung disease or pulmonary edema.
Step 3 - Targeted History
- Triggers: allergens, exercise, cold air, occupational agents → asthma
- Smoking history: COPD
- Medications: ACE inhibitors (cough, can mimic), beta-blockers (bronchoconstriction), NSAIDs/aspirin (aspirin-exacerbated respiratory disease)
- Position: orthopnea + wheeze → cardiac asthma
- Onset: acute = foreign body, anaphylaxis; subacute/chronic = asthma, COPD, tumor
Step 4 - First-Line Investigations
- CXR: hyperinflation (COPD/asthma), cardiomegaly + pulmonary edema, mass, foreign body
- Spirometry with bronchodilator reversibility: the single most important test
- BNP/NT-proBNP: if cardiac cause suspected
- FBC: eosinophilia supports atopic asthma
Step 5 - Spirometry Decision
- FEV1/FVC < 0.70 with ≥12% + ≥200 mL post-BD improvement = asthma
- FEV1/FVC < 0.70, minimal reversibility + smoking history = COPD
- Normal spirometry = does NOT exclude asthma (may need methacholine challenge, FeNO, or serial peak flows) and should prompt investigation of mimics
Step 6 - Wheeze Mimics (When Spirometry is Non-Diagnostic)
| Mimic | Key Test | Clue |
|---|---|---|
| Heart failure | BNP, Echo | Bibasilar crackles, orthopnea, elevated JVP |
| Endobronchial tumor / carcinoid | CT chest + bronchoscopy | Monophonic wheeze, hemoptysis, no response to BD |
| Foreign body aspiration | CT + bronchoscopy | Sudden onset, history of aspiration event |
| Vocal cord dysfunction (VCD) | Laryngoscopy during symptoms | Inspiratory stridor, paradoxical cord motion |
| Tracheal stenosis | Flow-volume loop (plateau), CT | Variable or fixed extrathoracic/intrathoracic pattern |
| Pulmonary embolism | CTPA | Acute onset, pleuritic pain, risk factors |
| GERD-related | pH-impedance monitoring | Worse post-meals, nocturnal |
| Vascular compression | CT angiography | Right-sided aortic arch, aberrant vessel |
| Bronchiolitis obliterans | HRCT (air-trapping), biopsy | Post-infection, post-transplant, collagen vascular disease |
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 898-902
A Key Pitfall to Remember
"Wheezes may be absent in severe airway obstruction due to absolute reduction in airflow; reappearance usually indicates improvement in the underlying obstruction."
- Murray & Nadel's, p. 898