Types of tympanostomy tubes and their names
Reading File
Searching the Web
types of tympanostomy tubes names designs
Finding Sources
Reading Web Page
types of tympanostomy tubes names short-term long-term
Reading File
Finding Sources
Here is a thorough breakdown of tympanostomy tube types:
Tympanostomy Tubes: Types and Names
Tympanostomy tubes (also called PE tubes, grommets, ventilation tubes, myringotomy tubes, or pressure equalization tubes) fall into two main categories based on how long they stay in the eardrum before extruding.
1. Short-Term Tubes (Grommet / Bobbin Design)
These are the most commonly used. They typically extrude spontaneously within 6-15 months. Most are shaped like a grommet or bobbin.
| Name | Notes |
|---|---|
| Armstrong tube | One of the most widely used designs worldwide; about 80% extrude by 2 years. The Long Armstrong variant is least prone to early extrusion. |
| Shepard tube | Standard short-term grommet; fastest to extrude (~93% gone by 2 years in trials). |
| Paparella type I | Smaller inner flange; shorter retention than Paparella type II. |
| Reuter Bobbin | Cylindrical bobbin shape; 66% extruded by 2 years in one major RCT. |
| Donaldson tube | Double-flanged silicone design; studied against Armstrong in large trials. |
| Sheehy bobbin | Another popular bobbin-style short-term tube. |
2. Long-Term Tubes (T-tube / Flanged Design)
Designed to stay in place for 15 months to several years. These have larger medial flanges or a T-shaped profile that resists extrusion. They are used in children with cleft palate, atrophic TM, or those who have already had multiple sets of short-term tubes.
| Name | Notes |
|---|---|
| Goode T-tube | Classic T-shaped design; only 31% extruded by 2 years in randomized trials - the most retentive in head-to-head studies. Typically stays 3-5 years. |
| Paparella type II | Larger inner flange than type I; behaves as a long-term tube; associated with higher rates of persistent perforation after extrusion. |
| Per-Lee tube | Long-term flanged tube with wide inner flange. |
| Shah grommet | Modification of the grommet with larger inner flange for prolonged retention. |
| Collar button tube | Generic term for any tube shaped like a collar button (wide inner flange, narrow shaft). |
Key Structural Variables That Affect Tube Behavior
- Shape of the medial flange - larger flanges resist extrusion (longer retention).
- Lateral flange presence - absence of a lateral flange speeds extrusion.
- Shaft length and inner diameter - affects patency and drainage.
- Material - most modern tubes are fluoroplastic (PTFE) or silicone, replacing older stainless steel, titanium, and gold tubes. Silicone tubes are associated with the longest time to first infection.
Summary: Short-Term vs. Long-Term at a Glance
| Feature | Short-Term (Grommet) | Long-Term (T-tube) |
|---|---|---|
| Retention | 6-15 months | 15 months to several years |
| Extrusion | Spontaneous | Often needs surgical removal |
| Best for | Most children with OME/rAOM | Cleft palate, atrophic TM, failed prior tubes |
| Examples | Armstrong, Shepard, Reuter Bobbin, Donaldson | Goode T-tube, Per-Lee, Paparella II |
Source: Cummings Otolaryngology Head and Neck Surgery (textbook, "Types of Tympanostomy Tubes and Indications") and Wikipedia on tympanostomy tubes. A 2020 SAGE visual guide specifically lists Armstrong II, Paparella I, Donaldson, Shepard, Sheehy, and Reuter Bobbins as the dominant short-term tubes worldwide.
Physiology of balance and tests of vestibular system
Finding Sources
Searching the Web
physiology of balance vestibular system tests clinical assessment
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Now I have comprehensive textbook material to compose a detailed, well-structured answer.
Physiology of Balance and Tests of the Vestibular System
Part 1: Physiology of Balance
The Three Sensory Inputs
Balance ("postural equilibrium") is maintained by integrating three sensory systems in the brainstem and cerebellum:
- Vestibular system - detects head motion and gravity
- Visual system - provides spatial orientation cues
- Proprioceptive / somatosensory system - joint and muscle position sense from the periphery
Disruption of any one of these can be partially compensated by the other two. When two or more are impaired, significant imbalance results.
Anatomy of the Vestibular End Organ
The vestibular apparatus sits within the bony labyrinth of the temporal bone, adjacent to the cochlea. It consists of a membranous labyrinth filled with endolymph and surrounded by perilymph.
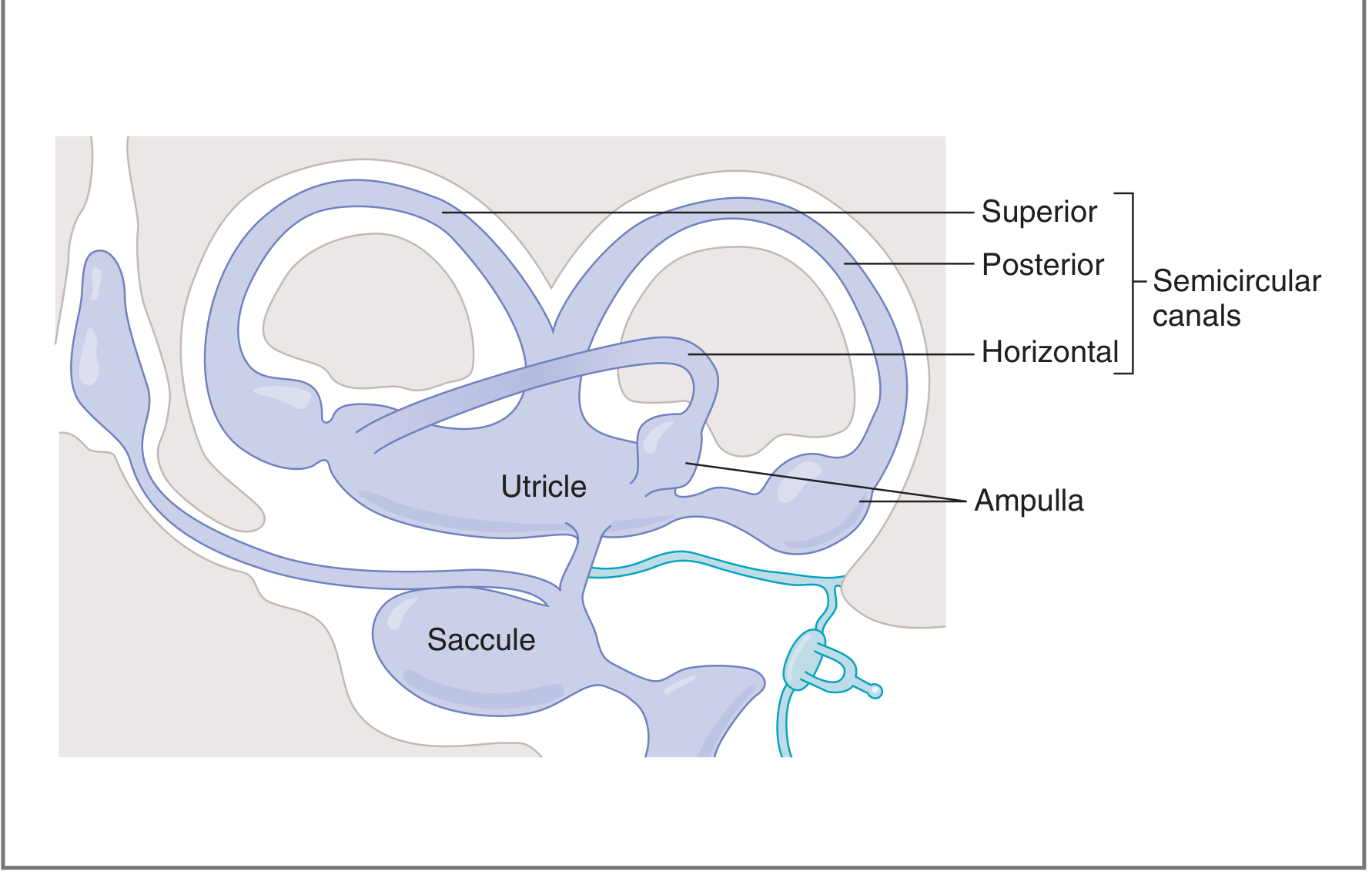
Fig. Structures of the vestibular organ - Costanzo Physiology 7th Ed.
It has five end organs in each ear:
| Structure | Number | Detects |
|---|---|---|
| Semicircular canals (SCCs) | 3 (horizontal, superior, posterior) | Angular / rotational acceleration |
| Utricle | 1 | Linear acceleration (horizontal plane) |
| Saccule | 1 | Linear acceleration (vertical plane, gravity) |
Semicircular Canals - How They Work
The three SCCs are arranged perpendicular to one another, covering all three axes of head rotation. Each canal has an ampulla at one end containing vestibular hair cells embedded in a gelatinous mass called the cupula. The cupula spans the entire cross-section of the ampulla and has the same specific gravity as endolymph.
Mechanism of transduction:
When the head rotates, the bony canal and attached ampulla move, but the endolymph initially lags due to inertia. This relative movement deflects the cupula, bending the stereocilia on hair cells.
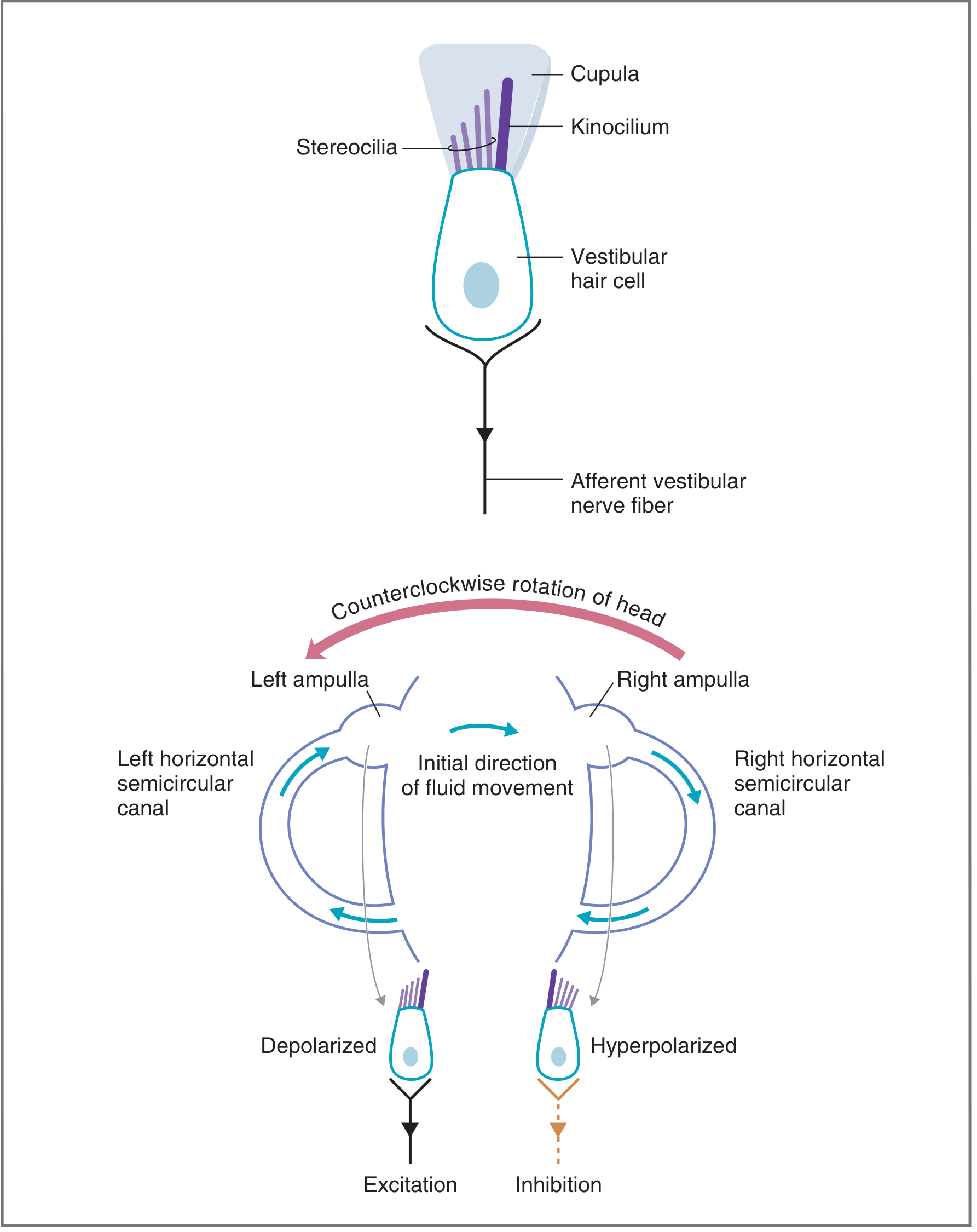
Fig. Vestibular hair cell transduction - Costanzo Physiology 7th Ed.
- Stereocilia bent toward the kinocilium → hair cell depolarizes → increased afferent firing
- Stereocilia bent away from kinocilium → hair cell hyperpolarizes → decreased afferent firing
Push-pull pairing: The lateral SCCs are paired with each other; the left superior SCC pairs with the right posterior SCC, and vice versa. When the head moves, one canal in a pair is excited while the opposite is inhibited. The CNS reads the differential firing rate as the signal for head movement.
"Hair cells within the SCCs fire at a baseline rate when at rest. When the head is moved rotationally, one of the pair of canals will increase its firing rate while the other will decrease. This differential signals a head movement in the plane of that canal." - K.J. Lee's Essential Otolaryngology
Otolith Organs - Utricle and Saccule
These detect linear acceleration (including gravity). Within them, the macula contains hair cells covered by an otolith mass - a gelatinous membrane embedded with calcium carbonate crystals (otoconia).
- When the head tilts, gravity pulls the heavy otolith mass across the hair cells, bending stereocilia
- Utricle: macula oriented horizontally when upright; detects lateral tilt and forward/backward linear motion
- Saccule: macula oriented vertically when upright; detects up/down motion (pitch and roll)
Because of the bilateral arrangement, every possible head orientation produces a unique pattern of excitation/inhibition across the four otolith organs (2 utricles + 2 saccules).
Central Vestibular Pathways
Afferent fibers from hair cells travel in the vestibular division of CN VIII to four vestibular nuclei in the medulla:
| Nucleus | Main Input | Main Output |
|---|---|---|
| Superior | SCCs | Extraocular muscles via MLF (mediates VOR) |
| Medial | SCCs | Extraocular muscles via MLF |
| Lateral (Deiters) | Utricle | Spinal cord via lateral vestibulospinal tract (postural reflexes) |
| Inferior | SCCs + otoliths | Brainstem + cerebellum via MLF |
The cerebellum modulates and fine-tunes all vestibular signals.
Vestibulo-Ocular Reflex (VOR)
The VOR maintains stable gaze during head movement. It generates eye movements equal and opposite to head rotation, preventing "retinal slip." The fovea covers a small visual field and cannot be kept on target by voluntary pursuit alone - the VOR fills this role during rapid head movements.
- Normal VOR: head turns right → eyes move left at equal velocity → gaze remains stable
- Impaired VOR (e.g., unilateral vestibular loss): head turns toward the affected side → eyes fail to compensate → a catch-up saccade is seen (the basis of the head impulse test)
Nystagmus - the hallmark of vestibular activity - consists of:
- Slow phase: the compensatory eye drift driven by vestibular input
- Fast phase (saccade): the rapid "reset" movement; nystagmus is named by the direction of the fast phase
Part 2: Tests of the Vestibular System
A. Bedside / Clinical Tests
| Test | What It Tests | How Done | Interpretation |
|---|---|---|---|
| Dix-Hallpike maneuver | Posterior SCC (BPPV) | Patient moved rapidly from sitting to head-hanging position, head turned 45°; Frenzel lenses improve sensitivity | Torsional upbeat nystagmus with latency, fatigability = BPPV; persistent/non-fatiguing = central |
| Head Impulse Test (HIT) | High-frequency VOR (horizontal SCC) | Examiner grasps head, makes a small rapid unpredictable head thrust; patient fixes on examiner's nose | Corrective saccade after the thrust = ipsilateral canal paresis (peripheral); normal VOR + nystagmus + skew deviation = HINTS criteria for central lesion |
| Romberg test | Postural control + proprioception | Stand feet together, arms crossed, eyes closed | Falling/excessive sway = peripheral vestibular, cerebellar, or severe neuropathy; does not localize on its own |
| Fukuda Stepping Test | Peripheral labyrinthine function | March in place 50 steps, eyes closed, arms outstretched | Rotation >45° = peripheral vestibular weakness; most sensitive for severe unilateral dysfunction |
| Unterberger test | Similar to Fukuda | Arms horizontal, eyes closed, march 50 steps | Rotation toward side of lesion |
| Skew deviation | Otolith-ocular pathway integrity | Cover-uncover test; look for vertical correction of each eye alternately | Skew (vertical misalignment) = brainstem/cerebellar lesion |
B. Laboratory / Instrumental Tests
1. Electronystagmography / Videonystagmography (ENG/VNG)
The most widely used formal vestibular test battery.
- ENG: records eye movements indirectly via electrodes measuring the corneoretinal potential (dipole). Electrodes placed at lateral canthi and around one eye.
- VNG: records directly with infrared video cameras in real time.
Test subsets:
Vestibular subsets:
- Spontaneous nystagmus
- Gaze nystagmus
- Positional nystagmus
- Positioning (Dix-Hallpike) nystagmus
- Fistula test
- Bithermal caloric tests
Oculomotor subsets:
- Smooth pursuit
- Saccadic system
- Optokinetic system
- Fixation suppression
2. Bithermal Caloric Test
The most important component of ENG/VNG - it tests the lateral SCC of each ear independently.
Setup: Head tilted back 60° (so horizontal canals are vertical). Each ear irrigated separately with:
- Water: 44°C (warm) and 30°C (cool) for 30 seconds each
- Air: 58°C and 24°C for 60 seconds (used when TM is perforated)
Mechanism: Temperature creates a convection current in endolymph - either ampullopetal (toward ampulla) or ampullofugal (away) flow - mimicking head rotation.
Mnemonic: COWS (Cold Opposite, Warm Same)
- Cold water → endolymph drops → ampullofugal flow → inhibition → nystagmus to the Opposite side
- Warm water → endolymph rises → ampullopetal flow → excitation → nystagmus to the Same side
Calculations:
- Unilateral weakness (UW) = [(RW + RC) - (LW + LC)] / (RW + RC + LW + LC) × 100%
-
15-30% = abnormal (peripheral lesion on the weaker side)
-
- Directional preponderance (DP) = comparison of right-beating vs. left-beating responses
-
30% may suggest central lesion
-
- Bilateral weakness: total slow-phase velocity for each side <12°/s
Contraindication: water irrigation with TM perforation (use air instead)
Central vs. Peripheral ENG findings:
| Peripheral Signs | Central Signs |
|---|---|
| Unilateral caloric weakness | Spontaneous nystagmus with normal calorics |
| Bilateral weakness with known ototoxicity | Direction-changing nystagmus |
| Fatiguing positional nystagmus | Failure of fixation suppression |
| Direction-fixed nystagmus | Abnormal saccades with normal calorics |
| Intact fixation suppression | Hyperactive caloric responses |
3. Rotary Chair Test (Rotational Chair / Sinusoidal Harmonic Acceleration)
- Patient sits in a motorized chair rotating in darkness at various frequencies
- Tests the VOR across a range of stimulus frequencies
- Tests both labyrinths simultaneously - useful when calorics are inconclusive
- Key parameters: VOR gain, phase, and symmetry
- Phase leads at low frequencies indicate loss of velocity storage (sign of peripheral lesion)
4. Vestibular Evoked Myogenic Potentials (VEMPs)
- cVEMP (cervical VEMP): loud sound stimulus → saccule → inferior vestibular nerve → ipsilateral sternocleidomastoid inhibition. Tests saccule and inferior vestibular nerve.
- oVEMP (ocular VEMP): same stimulus → utricle → superior vestibular nerve → contralateral inferior oblique activation. Tests utricle and superior vestibular nerve.
- Useful for diagnosing superior semicircular canal dehiscence, vestibular neuritis, and Meniere's disease.
5. Video Head Impulse Test (vHIT)
- Modern, objective version of the bedside HIT
- High-speed infrared camera tracks eye movements during rapid head thrusts in all six SCC planes
- Quantifies VOR gain for each individual SCC
- Detects covert saccades invisible to the naked eye
6. Computerized Dynamic Posturography (CDP)
- Measures postural stability on a moving platform while visual and/or proprioceptive cues are manipulated
- The sensory organization test (SOT) isolates each sensory input systematically
- Useful for functional assessment, rehab planning, and disability evaluation
7. Bárány (Rotation) Test - Historical/Bedside
Rotating the patient ~10 revolutions in a special chair then stopping abruptly:
- Normal: post-rotatory nystagmus toward the opposite side; patient falls toward the side of original rotation
- Tests both labyrinths simultaneously
Summary Table: Tests at a Glance
| Test | Structure Tested | Key Feature |
|---|---|---|
| Dix-Hallpike | Posterior SCC (BPPV) | Latency + fatigability = peripheral |
| Head Impulse (HIT/vHIT) | Horizontal SCC, high-frequency VOR | Catch-up saccade = ipsilateral paresis |
| Romberg | Postural control, proprioception | Non-localizing |
| Fukuda stepping | Peripheral labyrinth | >45° turn = peripheral deficit |
| ENG/VNG + Calorics | Each lateral SCC independently | COWS mnemonic; best for side-of-lesion |
| Rotary chair | Both labyrinths, VOR gain/phase | Best for bilateral loss assessment |
| cVEMP | Saccule + inferior vestibular nerve | Ipsilateral SCM inhibition |
| oVEMP | Utricle + superior vestibular nerve | Contralateral inferior oblique activation |
| CDP/Posturography | All three balance inputs | Functional disability, rehab |
Sources: Costanzo Physiology 7th Ed. (pp. 102-104); K.J. Lee's Essential Otolaryngology (pp. 345-352); Cummings Otolaryngology Head and Neck Surgery (p. 2638); Scott-Brown's Otorhinolaryngology Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.