Hyperkalemia treatment guidelines
Reading File
Searching PubMed
hyperkalemia treatment guidelines management
Finding Sources
Reading Article
PMID: 40685253
Reading Article
PMID: 40542996
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Here is the full, synthesized answer:
Hyperkalemia Treatment Guidelines
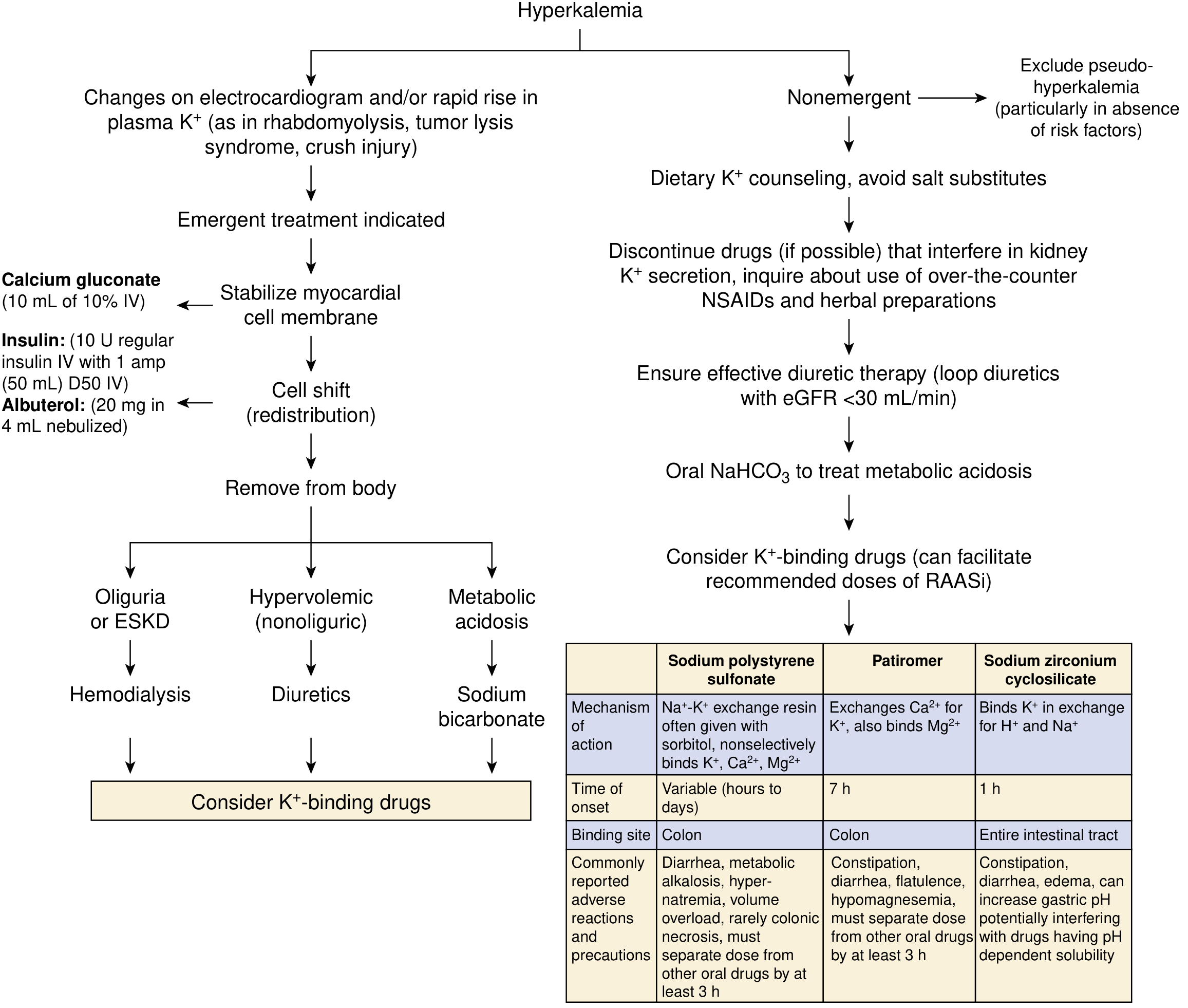
Fig. 10.3 - Approach to treatment of hyperkalemia (Palmer BF, Clegg DJ. Am J Kidney Dis. 2019)
Classification by Severity
| Severity | K+ Level | ECG Findings | Urgency |
|---|---|---|---|
| Mild | 5.5-6.0 mEq/L | None | Hours |
| Moderate | 6.0-6.5 mEq/L | Peaked T waves | Prompt (within 1 hour) |
| Severe | >6.5 mEq/L or any level with ECG changes | Wide QRS, loss of P waves, sine wave | Emergent |
There is no single plasma K+ concentration that defines "severe" hyperkalemia - any ECG change consistent with hyperkalemia renders the level "severe" and requires emergent management, regardless of the absolute value. - NKF Primer on Kidney Diseases, 8e
STEP 1 - Stabilize the Cardiac Membrane (Emergent, ECG changes present)
Calcium salts - do NOT lower plasma K+, but directly antagonize the cardiac membrane effects of hyperkalemia.
- Calcium gluconate: 10 mL of 10% solution IV over 1-3 minutes (preferred for peripheral IV access)
- Calcium chloride: 3-5 mL of 10% solution IV (more elemental calcium per ampule, but causes skin necrosis if it infiltrates - use central line only)
- Effect is rapid and nearly immediate; if no ECG improvement in 3-5 minutes, repeat the dose
- Effect is transient (30-60 min) - must follow with redistribution therapies
- Caution in digoxin toxicity: calcium potentiates digoxin cardiotoxicity
STEP 2 - Shift K+ Into Cells (Redistribution - Temporizing)
A. Insulin + Dextrose (fastest and most reliable)
- Regular insulin 10 units IV + 50 mL of 50% dextrose (D50W) as a bolus
- Follow with D5W infusion at 100 mL/hour to prevent late hypoglycemia
- K+ begins to fall within 15 minutes, peak effect at ~60 minutes
- Key cautions:
- Never give dextrose without insulin - in patients with inadequate endogenous insulin, hyperglycemia can paradoxically raise K+
- If blood glucose >300 mg/dL, insulin can be given without dextrose
- Monitor glucose closely; hypoglycemia is common in renal failure (prolonged insulin half-life)
- Lispro/aspart may cause less hypoglycemia in kidney failure as they are not renally metabolized
B. Nebulized Albuterol (Beta-2 Agonist)
- 20 mg nebulized over 10 minutes (use concentrated 5 mg/mL formulation)
- Onset ~30 minutes; effect is additive to insulin
- The dose needed for K+ lowering is much higher than the bronchodilator dose
- IV albuterol 0.5 mg (available in Europe) is equivalent to 20 mg nebulized
- Low-dose IV epinephrine infusion can also be used in emergencies (e.g., post-massive transfusion) with added inotropic benefit
C. Sodium Bicarbonate
- Lowers K+ by enhancing renal K+ excretion, not by cell shift (useful in patients with residual kidney function)
- Onset within 15 minutes when metabolic acidosis is present
- Indications: metabolic acidosis (especially serum bicarb <10 mmol/L) AND the patient has residual kidney function
- Not indicated as routine emergency monotherapy in patients without residual kidney function (ESKD/dialysis patients)
- Does not enhance the potassium-lowering effects of insulin or albuterol - no additive benefit in combination
STEP 3 - Remove K+ from the Body (Definitive Therapy)
A. Diuretics
- Loop and thiazide diuretics - effective if adequate kidney function exists
- Loop diuretics preferred when eGFR <30 mL/min
- Not useful in oliguric AKI or ESKD
B. Hemodialysis
- Most effective modality for K+ removal
- Indicated for severe hyperkalemia with oliguria, AKI, or ESKD
- Cannot typically be initiated fast enough to replace emergency measures above - stabilize with Steps 1-2 first
C. Potassium Binders (oral/rectal - adjunct and chronic prevention)
| Drug | Mechanism | Binding Site | Onset | Starting Dose | Key Adverse Effects |
|---|---|---|---|---|---|
| Sodium polystyrene sulfonate (SPS/Kayexalate) | Na+-K+ exchange resin | Colon | Hours to days (variable) | 50 g in 30 mL sorbitol PO or enema | Diarrhea, metabolic alkalosis, hypernatremia, rare colonic necrosis (FDA black box warning) |
| Patiromer (Veltassa) | Exchanges Ca2+ for K+ | Colon | ~7 hours | 8.4 g once daily; titrate weekly | Constipation, diarrhea, hypomagnesemia; separate from other drugs by 3 hours |
| Sodium zirconium cyclosilicate (Lokelma) | Binds K+ in exchange for H+ and Na+ | Entire GI tract | ~1 hour | 10 g three times daily x 48 h, then 5-10 g once daily | Constipation, diarrhea, edema; can raise gastric pH |
Important caveats for binders:
- SPS: not approved for chronic management; evidence base is weak (mostly small, low-quality studies); colonic necrosis risk is real especially with sorbitol
- Patiromer and SZC: FDA-approved for chronic management of hyperkalemia; multiple RCTs show ~1 mEq/L sustained reduction in K+; particularly useful to allow continuation/up-titration of RAASi in CKD and heart failure
- None of the binders should be used as monotherapy for acute or emergency hyperkalemia - use only as adjuncts to Steps 1-2
Non-Emergent Management (No ECG Changes)
- Stop exogenous K+ (IV fluids, dietary sources, salt substitutes)
- Dietary K+ counseling - avoid high-K+ foods, salt substitutes containing KCl
- Discontinue or dose-reduce causative drugs where possible: NSAIDs, ACE inhibitors, ARBs, potassium-sparing diuretics, trimethoprim, heparin
- Treat underlying cause (e.g., fludrocortisone for hypoaldosteronism)
- Ensure effective diuretic therapy - loop diuretics especially when eGFR <30 mL/min
- Oral NaHCO3 to treat metabolic acidosis
- Consider K+ binders - particularly to enable guideline-directed RAASi use in CKD/HF patients
Special Clinical Situations
Hyperkalemia in CKD/Heart Failure on RAASi
A 2025 systematic review and network meta-analysis (PMID: 40542996) found that novel potassium binders (patiromer and SZC) improved RAASi optimization by 38% compared to placebo, decreased hyperkalemia incidence by 28%, and reduced K+ by 0.71 mEq/L. The 2025 GUARDIAN-HK European consensus (PMID: 40685253) explicitly states that RAASi should no longer be considered a reversible cause of hyperkalemia - instead, K+ binders should be used to maintain patients on guideline-directed target doses.
Perioperative/Anesthetic Considerations
- Elective surgery should be deferred until hyperkalemia is corrected
- Succinylcholine is contraindicated - depolarizing blockade causes additional K+ release
- Avoid potassium-containing IV solutions (e.g., lactated Ringer's)
- Avoid metabolic or respiratory acidosis - use controlled ventilation
- Monitor neuromuscular function closely - hyperkalemia accentuates NMB effects
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Digoxin-Toxic Patients
- Calcium is relatively contraindicated - calcium potentiates digoxin cardiotoxicity ("stone heart" syndrome)
- Consider Digibind (digoxin-specific antibody fragments) instead
Summary Algorithm
Hyperkalemia
|
├── ECG changes or K+ >6.5 mEq/L → EMERGENT
│ 1. Calcium gluconate 10 mL 10% IV (stabilize membrane)
│ 2. Insulin 10U + D50W IV (shift)
│ + Albuterol 20 mg nebulized (shift, additive)
│ 3. Remove: Diuretics / Dialysis / Binders (adjunct)
│
└── No ECG changes, K+ 5.5-6.5 mEq/L → NON-EMERGENT
- Stop K+ sources, dietary counseling
- Remove causative drugs
- Loop diuretics (if renal function intact)
- Oral NaHCO3 (if metabolic acidosis)
- Chronic K+ binders (patiromer or SZC) to enable RAASi
Sources:
- NKF Primer on Kidney Diseases, 8e (p. 128-129)
- Morgan and Mikhail's Clinical Anesthesiology, 7e (p. 2180-2181)
- Sabiston Textbook of Surgery, 11e (Box 33.5, p. 602)
- GUARDIAN-HK European Steering Committee, 2025 [PMID: 40685253]
- Huang et al., Drugs, 2025 - Novel Potassium Binders Meta-analysis [PMID: 40542996]
This is a shared conversation. Sign in to Orris to start your own chat.