Asthma topic from fishman Murray and nadal and gina guidelines explain and make notes simple words
Reading File
Finding Sources
Searching the Web
GINA guidelines 2025 asthma definition pathophysiology diagnosis treatment summary
Reading File
Reading File
Reading Web Page
https://ginasthma.org/wp-content/uploads/2025/11/GINA-2025-U…
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the key content. Let me compile the comprehensive, simple-language notes.
🫁 ASTHMA - Complete Notes
Sources: Murray & Nadel's Textbook of Respiratory Medicine + GINA 2025 Guidelines
PART 1: DEFINITION
"Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness, and cough that vary over time and in intensity, together with variable expiratory airflow limitation." — GINA 2025 / Murray & Nadel (Chapter 62)
In simple words: Asthma is a lung disease where the airways get inflamed, narrow, and produce excess mucus - making it hard to breathe. The good news is this narrowing is usually REVERSIBLE (airways open up again, either on their own or with treatment).
Key features:
- Chronic inflammation - ongoing swelling inside airways
- Variable obstruction - airflow blockage that comes and goes
- Bronchial hyperresponsiveness (BHR) - airways react to things that don't bother normal people (cold air, exercise, dust)
- Heterogeneous - different patients have different types/triggers
PART 2: PATHOPHYSIOLOGY (How it happens)
2.1 Normal vs Asthmatic Airway
| Feature | Normal | Asthma |
|---|---|---|
| Airway wall | Thin | Thickened, inflamed |
| Mucus | Normal | Excess, sticky |
| Smooth muscle | Relaxed | Hypertrophied, twitchy |
| Lumen (space) | Wide open | Narrowed |
2.2 The Inflammatory Cascade (T2-High / Allergic Asthma)
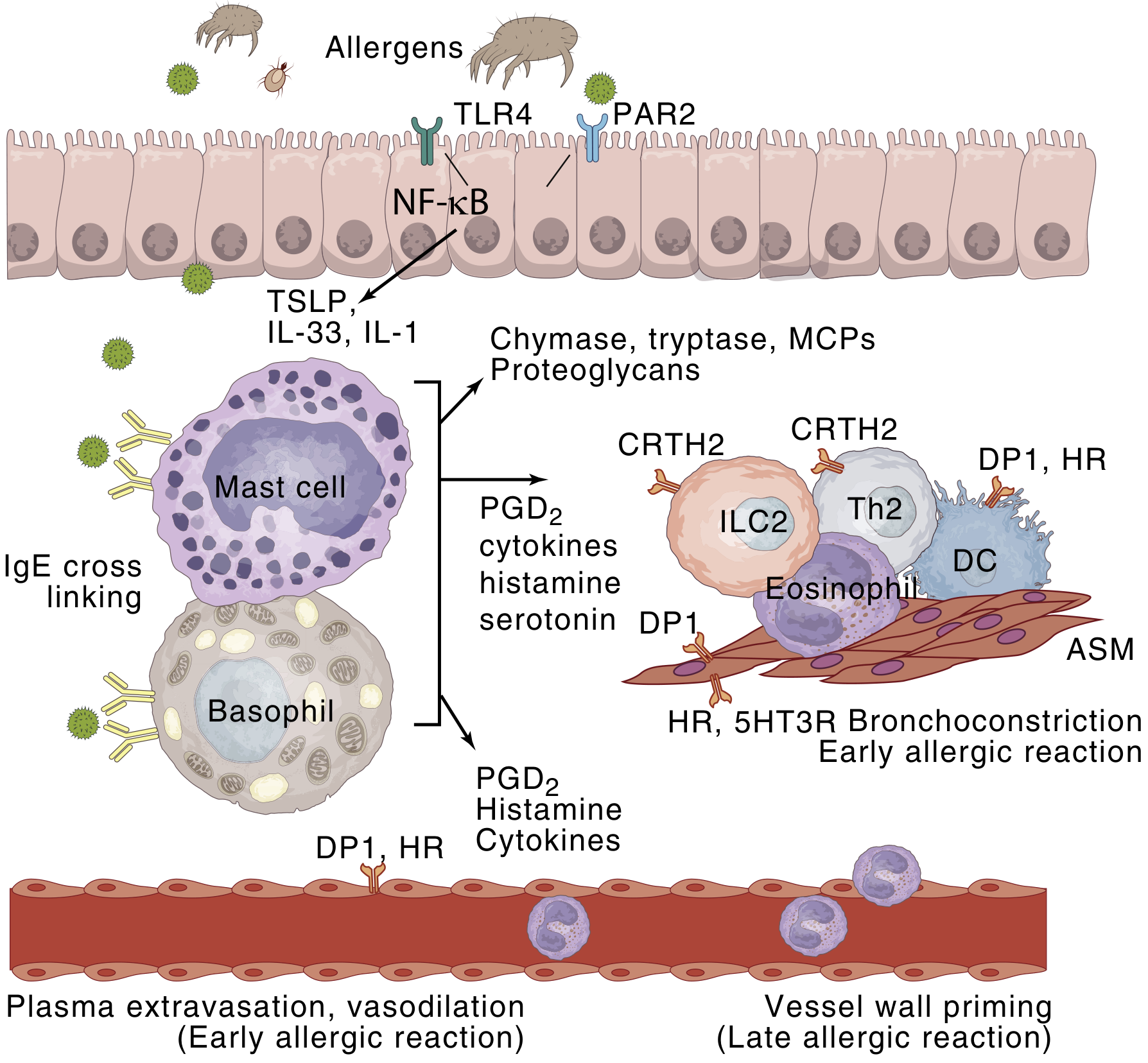
Step-by-step (simple):
- Allergen enters the airway (dust mite, pollen, animal dander)
- Airway epithelial cells release alarm signals: TSLP, IL-33, IL-1
- Mast cells & basophils get activated (IgE cross-linking)
- They release: histamine, PGD2, leukotrienes → BRONCHOCONSTRICTION (early allergic reaction, within minutes)
- Eosinophils are recruited (via IL-5 from Th2 cells and ILC2s) → LATE PHASE REACTION (hours later)
- Repeated episodes → airway remodeling (permanent structural changes)
2.3 Key Cells in Asthma
| Cell | What it does |
|---|---|
| Mast cell | First responder - releases histamine, causes immediate bronchoconstriction |
| Eosinophil | Major effector - releases toxic granules, damages airway lining |
| Th2 lymphocyte | Produces IL-4, IL-5, IL-13 - drives allergic inflammation |
| ILC2 | Innate version of Th2 cells - important in non-allergic asthma |
| Airway smooth muscle | Contracts abnormally, also becomes hypertrophied |
| Dendritic cell | Presents allergen to T cells |
2.4 Key Mediators
- Histamine → bronchoconstriction, mucus, itch
- Leukotrienes (LTC4, LTD4) → powerful bronchoconstriction + mucus
- IL-5 → eosinophil growth + survival
- IL-13 → mucus hypersecretion + airway hyperresponsiveness
- IL-4 → IgE production (switches B cells to make IgE)
- IgE → sits on mast cells, triggers degranulation when allergen binds
2.5 Airway Remodeling (Chronic Changes)
- Subepithelial fibrosis (thickening below the lining)
- Smooth muscle hypertrophy (muscle gets bigger)
- Angiogenesis (new blood vessels form)
- Goblet cell hyperplasia (more mucus-producing cells)
- These changes may make obstruction partially irreversible over time
PART 3: PHENOTYPES (Types of Asthma)
Murray & Nadel emphasizes asthma is heterogeneous - not one disease:
| Phenotype | Features | Who gets it |
|---|---|---|
| Allergic (T2-high) | Elevated IgE, eosinophils, responds to steroids | Children, atopic adults |
| Non-allergic | Eosinophilic but no allergy, often adult-onset | Adults |
| Late-onset eosinophilic | Adult onset, severe, nasal polyps, aspirin sensitivity | Adults |
| Obesity-associated | Hard to control, minimal eosinophils | Obese patients |
| Exercise-induced | Triggered only by exercise | Athletes, children |
| Occupational | Triggered by workplace exposure | Industrial workers |
| Aspirin-exacerbated | Samter's triad: asthma + nasal polyps + aspirin sensitivity | Adults |
PART 4: DIAGNOSIS
4.1 Diagnostic Algorithm (Murray & Nadel, Fig. 62.1)
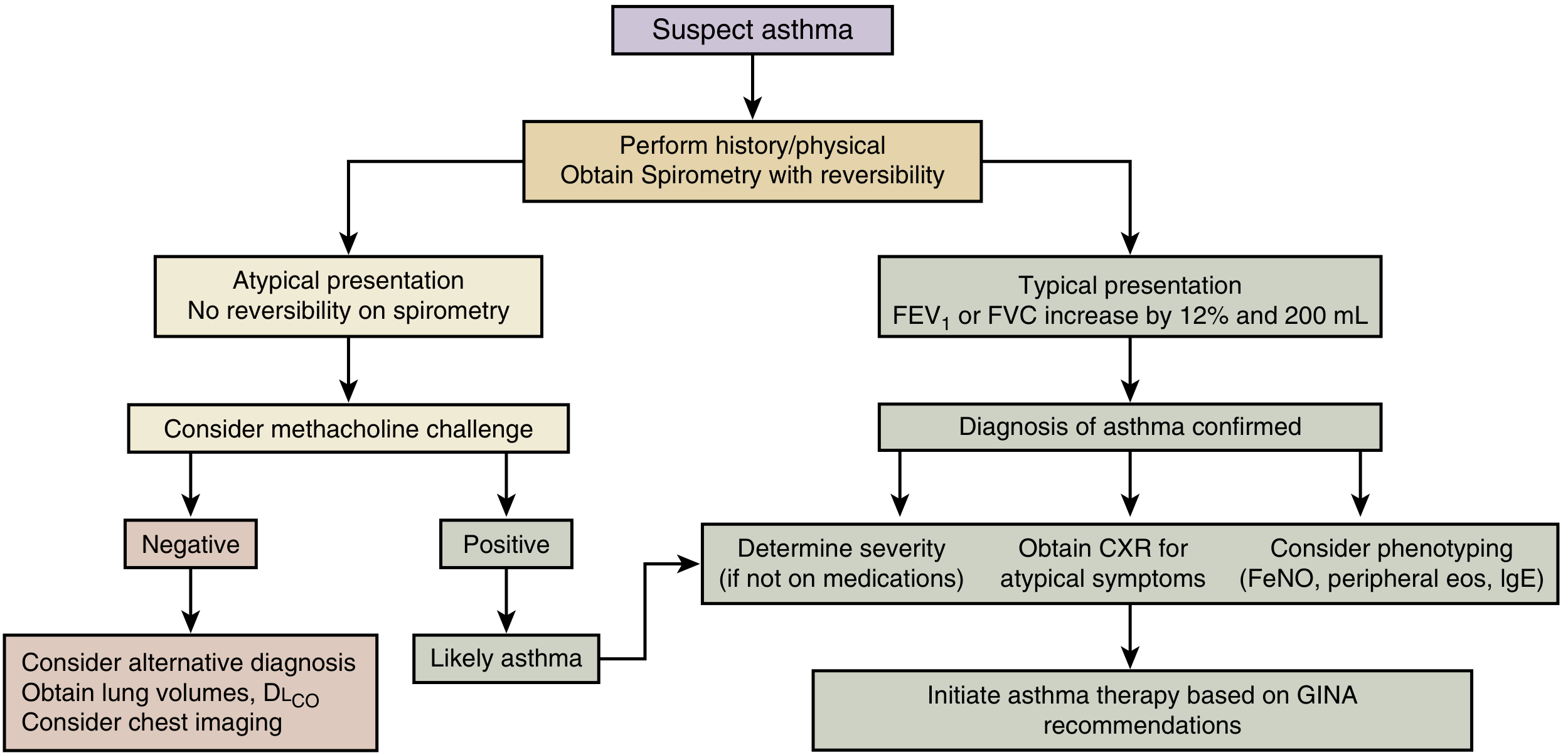
Simple flow:
- Suspect asthma (symptoms: wheeze, SOB, chest tightness, cough)
- Take history + physical + spirometry with bronchodilator test
- POSITIVE (FEV1 or FVC increases by ≥12% AND ≥200 mL after bronchodilator) → Asthma confirmed
- NEGATIVE/Atypical → Methacholine challenge test
- Positive methacholine → Likely asthma
- Negative methacholine → Consider alternative diagnosis
4.2 GINA 2025 - 4 Cardinal Symptoms
The classic symptom cluster:
- Wheezing
- Shortness of breath
- Chest tightness
- Cough (often worse at night or early morning)
Clues that it IS asthma:
- Symptoms vary (better and worse at different times)
- Symptoms triggered by exercise, cold air, smoke, allergens
- Symptoms worse at night or early morning
- Personal/family history of atopy (eczema, hay fever)
- Symptoms respond to bronchodilators
4.3 Spirometry Findings in Asthma
| Test | Asthma pattern |
|---|---|
| FEV1/FVC ratio | Reduced (obstructive) |
| FEV1 | Reduced |
| After bronchodilator | FEV1 or FVC increases ≥12% AND ≥200 mL ✓ |
| PEF variability | >10% (GINA); >20% more suggestive |
| FEV1 when well | May be completely NORMAL |
4.4 Other Tests (GINA 2025)
| Test | Useful for |
|---|---|
| Methacholine challenge | When spirometry is normal but asthma suspected |
| FeNO (exhaled NO) | Detects T2 (eosinophilic) inflammation; >25 ppb supports T2 asthma |
| Blood eosinophils | Elevated (>300/μL) supports T2 asthma phenotype |
| Total IgE / skin prick tests | Confirms allergic phenotype |
| CXR | Usually normal in asthma; useful to exclude other diagnoses |
| Sputum eosinophils | Can guide steroid therapy (not widely available) |
4.5 Differential Diagnosis (What else looks like asthma?)
- COPD (fixed obstruction, smoking history, older patients)
- Vocal cord dysfunction (stridor, paradoxical vocal cord movement)
- Heart failure ("cardiac asthma" - orthopnea, elevated BNP)
- Bronchiectasis (daily productive cough, recurrent infections)
- Cystic fibrosis (young patients, pancreatic involvement)
- GERD-related cough
- Sarcoidosis
PART 5: ASSESSMENT AND CLASSIFICATION
5.1 GINA Asthma Symptom Control (past 4 weeks)
Ask these 4 questions:
- Daytime symptoms more than twice per week?
- Any night waking due to asthma?
- Reliever used more than twice per week?
- Any activity limitation due to asthma?
| # of "YES" answers | Control level |
|---|---|
| 0 | Well controlled ✅ |
| 1-2 | Partly controlled ⚠️ |
| 3-4 | Uncontrolled ❌ |
(Murray & Nadel, Table 62.1 - GINA Classification of Asthma Control)
5.2 GINA Severity Classification (retrospective - based on treatment needed)
| Severity | Definition |
|---|---|
| Mild | Well controlled on Step 1 or Step 2 |
| Moderate | Well controlled on Step 3 |
| Severe | Requires Step 4 or Step 5 (or remains uncontrolled despite it) |
Important: Severity is assessed AFTER treatment is started, not at diagnosis!
5.3 Risk Factors for Exacerbations (GINA 2025)
- Uncontrolled symptoms
- Frequent SABA use (>2x/week)
- Not on ICS
- Poor inhaler technique or adherence
- Smoking, allergen exposure
- Obesity, chronic rhinosinusitis, GERD
- Low FEV1 (<60% predicted)
- Previous severe exacerbation or ICU admission
PART 6: TREATMENT (GINA Stepwise Approach)
6.1 Big Picture Concept
GINA 2025 key change: There is NO "reliever-only" Step 1. Even mild asthma needs anti-inflammatory treatment because SABA-only therapy is unsafe. Use ICS-formoterol as the preferred reliever at all steps.
6.2 The 5-Step Treatment Ladder
(Murray & Nadel, Fig. 62.3 / Table 62.2)
| Step | Preferred Controller | Preferred Reliever |
|---|---|---|
| Step 1 (Mildest) | As-needed low-dose ICS-formoterol | As-needed low-dose ICS-formoterol |
| Step 2 | Low-dose ICS (daily) OR as-needed ICS-formoterol | As-needed SABA or ICS-formoterol |
| Step 3 | Low-dose ICS-LABA (daily) | As-needed SABA or ICS-formoterol |
| Step 4 | Medium-dose ICS-LABA | As-needed SABA or ICS-formoterol |
| Step 5 (Severe) | High-dose ICS-LABA + refer for phenotyping/add-on therapy | As-needed SABA or ICS-formoterol |
Step up if not controlled. Step down once controlled for 3 months.
6.3 Drug Classes Explained Simply
A. Inhaled Corticosteroids (ICS) - BACKBONE of treatment
- Examples: Budesonide, Fluticasone, Beclomethasone
- Work by: Reducing airway inflammation
- Use: Daily controller therapy
- Key point: Most important single drug in asthma management
B. Long-Acting Beta-2 Agonists (LABA) - always with ICS
- Examples: Formoterol, Salmeterol, Vilanterol
- Work by: Relaxing airway smooth muscle (bronchodilation)
- Use: Combined with ICS for moderate-severe asthma
- Warning: NEVER use LABA alone without ICS in asthma
C. Short-Acting Beta-2 Agonists (SABA) - rescue use
- Examples: Salbutamol (albuterol), Terbutaline
- Work by: Quick bronchodilation (within minutes)
- Use: Reliever for acute symptoms
- Warning: Overuse (>2x/week) = poor control = increase therapy
D. Leukotriene Receptor Antagonists (LTRA) - add-on
- Examples: Montelukast
- Work by: Blocking leukotriene receptors
- Use: Add-on at Step 2-3; good for aspirin-sensitive asthma, exercise-induced asthma, allergic rhinitis with asthma
E. Theophylline - older add-on
- Low-dose has anti-inflammatory effect
- Narrow therapeutic window, multiple interactions
- Less preferred today
F. Short-Acting Muscarinic Antagonist (SAMA)
- Examples: Ipratropium
- Used in acute severe asthma (added to SABA in ER)
G. Long-Acting Muscarinic Antagonist (LAMA) - Step 4-5 add-on
- Examples: Tiotropium
- Added to ICS-LABA in uncontrolled severe asthma
6.4 Biologics (Step 5 - Severe Asthma Only)
These are targeted therapies for specific asthma phenotypes:
| Drug | Target | Phenotype | Dosing |
|---|---|---|---|
| Omalizumab | Anti-IgE | Allergic (T2-high) | SC every 2-4 weeks |
| Mepolizumab | Anti-IL-5 | Severe eosinophilic | SC monthly |
| Reslizumab | Anti-IL-5 | Severe eosinophilic (eos ≥400/μL) | IV every 4 weeks |
| Benralizumab | Anti-IL-5Rα | Severe eosinophilic (eos ≥300/μL) | SC monthly x3, then every 8 weeks |
| Dupilumab | Anti-IL-4Rα (blocks IL-4 + IL-13) | Eosinophilic OR oral steroid-dependent | SC every 2 weeks |
| Tezepelumab | Anti-TSLP | Broad (T2 and non-T2) | SC monthly |
(Murray & Nadel, Chapter 62, biologic section)
PART 7: ACUTE EXACERBATIONS (Asthma Attack)
7.1 Severity Assessment
| Feature | Mild-Moderate | Severe | Life-threatening |
|---|---|---|---|
| Speech | Full sentences | Short phrases | Unable to speak |
| Accessory muscles | No | Yes | Yes + paradoxical |
| RR | <25 | >25 | Variable |
| HR | <110 | >110 | Bradycardia (bad sign) |
| SpO2 | >95% | 90-95% | <90% |
| PEFR | >50% predicted | 33-50% | <33% |
| PaCO2 | Normal/low | Low | Rising (DANGER!) |
Rising CO2 in an acute attack = patient is tiring out → consider ICU/intubation
7.2 Acute Management (GINA Primary Care)
- Bronchodilator: Inhaled SABA (salbutamol) 4-10 puffs via spacer every 20 min x 3 in first hour
- Severe: Add ipratropium (SAMA)
- Oxygen: Titrate to SpO2 93-95%
- Systemic corticosteroids: Oral prednisolone 40-50 mg/day (or IV hydrocortisone) for 5-7 days
- Reassess after 1 hour:
- Good response → discharge with action plan
- Poor response → admit or escalate
- Magnesium sulfate (IV): For severe exacerbations not responding to bronchodilators
- Heliox, NIV, intubation: For life-threatening exacerbations
7.3 Discharge Checklist
- ✅ Prescribe or adjust controller treatment (ICS or ICS-LABA)
- ✅ Ensure SABA reliever provided
- ✅ Ensure good inhaler technique demonstrated
- ✅ Give written asthma action plan
- ✅ Follow up within 1 week
- ✅ Address risk factors
PART 8: SPECIAL SITUATIONS
8.1 Asthma in Pregnancy
- Affects 3.7-8.4% of pregnancies
- Uncontrolled asthma is MORE dangerous than the medications
- 1/3 worsen, 1/3 improve, 1/3 unchanged
- Safe drugs in pregnancy: ICS (budesonide preferred), SABA, LABA (with ICS)
- Avoid: High-dose oral steroids if possible (risk of growth restriction, cleft palate)
- Principle: Treat to keep asthma controlled - same stepwise approach
8.2 Asthma + Obesity
- More difficult to control
- Less eosinophilic
- Poor response to ICS
- Weight loss significantly improves asthma control
- OSA is common comorbidity - treat with CPAP
8.3 Asthma + OSA (Sleep Apnea)
- OSA worsens asthma control
- Mechanisms: OSA causes oxidative stress → bronchoconstriction; upper airway closure → vagal reflex bronchoconstriction
- Treat OSA with CPAP → improves asthma quality of life, reduces exacerbations
8.4 Occupational Asthma
- New-onset or worsening asthma due to workplace exposure
- Common causes: isocyanates, flour, latex, animal proteins
- Key: Remove from exposure - treatment is secondary
8.5 Exercise-Induced Bronchoconstriction (EIB)
- Peaks 5-15 min after exercise, resolves within 30-60 min
- Diagnosis: >10% fall in FEV1 after exercise challenge
- Prevention: Pre-exercise inhaled SABA OR ICS-formoterol
PART 9: MONITORING AND FOLLOW-UP
9.1 Validated Tools to Assess Control
- Asthma Control Test (ACT) - 5 questions, score 5-25 (≥20 = well controlled)
- Asthma Control Questionnaire (ACQ) - 7 items
- GINA symptom control - the 4 YES/NO questions (above)
9.2 What to Check at Every Visit
- Symptom control (GINA 4 questions)
- Exacerbation frequency
- SABA use
- Inhaler technique (check every time!)
- Adherence to controller medication
- Lung function (spirometry at least annually)
- Trigger avoidance
9.3 When to Step Down Treatment
- Good control for at least 3 months
- Low risk of exacerbation
- Step down slowly, one step at a time
- Don't step down ICS completely in most patients
PART 10: GINA 2025 KEY UPDATES (New This Year)
- New asthma definition - updated wording to reflect heterogeneity
- New diagnostic flowchart - clearer pathway using spirometry + biomarkers
- T2 biomarkers emphasized - Blood eosinophils + FeNO to assess Type 2 inflammation before starting/adjusting treatment
- Population vs patient level treatment - New figure distinguishing population-level recommendations from individualized decisions
- No SABA-only at Step 1 - ICS-formoterol as preferred reliever at ALL steps
- Children <5 years: New explicit 3-criteria diagnosis:
- Recurrent wheezing episodes
- No other likely cause
- Clinical response to asthma medications
- Severe exacerbations in <5y: New SpO2 threshold + nebulized magnesium added
- Climate change acknowledged as risk factor for exacerbations
- Biomarkers appendix - sputum eos, blood eos, FeNO, IgE, periostin - how to use in clinical context
QUICK MEMORY AID
ASTHMA =
A - Airway inflammation (chronic)
S - Symptoms: wheeze, SOB, chest tightness, cough
T - Triggers: allergens, exercise, cold, smoke, infections
H - Hyperresponsiveness (airways overreact)
M - Mostly reversible obstruction
A - Anti-inflammatory therapy (ICS) is the cornerstone
GINA CONTROL = 4 questions in 4 weeks
0 YES = Well controlled
1-2 YES = Partly controlled
3-4 YES = Uncontrolled
STEPS 1-5:
Step 1 = As-needed ICS-formoterol
Step 2 = Low-dose ICS daily
Step 3 = Low-dose ICS-LABA
Step 4 = Medium-dose ICS-LABA
Step 5 = High-dose ICS-LABA + Biologic
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine (Chapter 62 - Diagnosis and Treatment of Asthma; Chapter 60 - Molecular Immunology of Asthma)
- GINA 2025 Global Strategy Report - Updated November 2025
- GINA 2025 Key Updates Summary
Asthma topic from fishman textbook and gina 2026
Finding Sources
Searching the Web
GINA 2026 asthma guidelines key updates new recommendations
Finding Sources
Reading Web Page
https://www.hmpgloballearningnetwork.com/site/allergy/videos…
Reading File
Reading File
Searching the Web
GINA 2026 stepwise treatment steps ICS-formoterol depemokimab new biologic anti-TSLP tezepelumab
Finding Sources
Reading Web Page
https://www.pulmonologyadvisor.com/features/asthma-gina-2026…
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading Web Page
https://ginasthma.org/wp-content/uploads/2026/05/GINA-2026-S…
I now have all the material needed. Let me compile the comprehensive notes.
🫁 ASTHMA - Complete Notes
Sources: Fishman's Pulmonary Diseases & Disorders + GINA 2026 (Published May 5, 2026)
PART 1: DEFINITION & OVERVIEW
Fishman's Definition:
"Asthma is a chronic inflammatory disease of the airways characterized by persistent variable symptoms that include shortness of breath, cough, and wheezing. It is the most common chronic lung disease and one of the most prevalent diseases in the United States, affecting more than 20 million adults and 7 million children."
- Fishman's Pulmonary Diseases & Disorders, Chapter 43
GINA 2026 Definition:
"Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness, and cough that vary over time and in intensity, together with variable expiratory airflow limitation."
3 Core Features (Fishman's):
- Bronchoconstriction + variable airflow obstruction - airways narrow and open up
- Airway hyperresponsiveness (AHR) - airways overreact to triggers
- Chronic airway inflammation - ongoing immune cell activity in the airways
PART 2: PATHOPHYSIOLOGY (Fishman's - The Deep Dive)
2.1 The Inflammatory Pathways
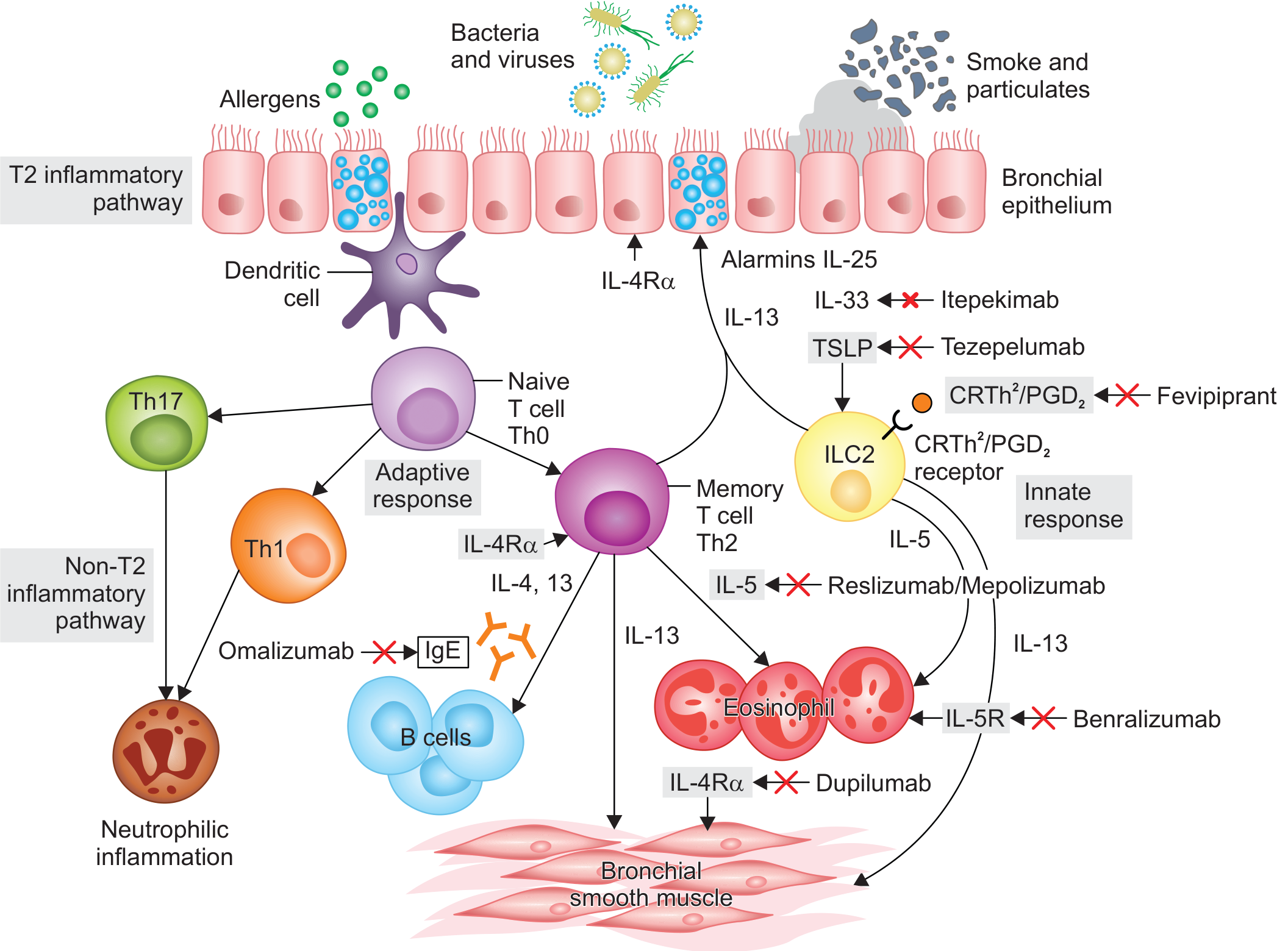
Fishman's describes two main inflammatory pathways:
| Pathway | Driven By | Leads To | Typical Patient |
|---|---|---|---|
| T2 (Type 2) | Th2 cells + ILC2 + IL-4, IL-5, IL-13 | Eosinophilic inflammation | 65-80% of asthmatics, allergic |
| Non-T2 | Th1 + Th17 cells | Neutrophilic inflammation | Obese, severe, steroid-resistant |
2.2 How the Allergic Response Starts
Step-by-step (simple version):
- Allergen hits bronchial epithelium
- Epithelial cells release alarmins: TSLP, IL-25, IL-33
- Alarmins activate dendritic cells → present allergen → naive T cell becomes Th2 cell
- ILC2 (innate lymphoid cells) also activated by alarmins → release IL-5
- Th2 cells produce: IL-4, IL-5, IL-13
- B cells get IL-4 → produce IgE
- IgE binds to mast cells → on re-exposure to allergen → mast cell degranulation
- Release of histamine, tryptase, PGD2 → EARLY PHASE reaction (within minutes)
- Eosinophils recruited (via IL-5) → LATE PHASE reaction (hours later)
2.3 Key Cells in Fishman's
Mast Cells
- First responders in allergic asthma
- Release histamine (bronchoconstriction, edema, mucus), tryptase (activates other cells), PGD2
- BAL histamine peaks at 12 minutes after allergen challenge
- Tryptase normalizes at 48h; histamine stays elevated (other cells take over)
Eosinophils
- Major effectors in T2 asthma
- Release toxic granule proteins: MBP (major basic protein), ECP, EDN, EPX
- MBP → bronchial hyperreactivity by interfering with muscarinic receptors
- Cause airway remodeling, mucus plugs
- Key insight (Fishman's): Eosinophilia plays variable roles in different patients - explains why anti-IL-5 worked in some but not all
Neutrophils
- Recruited by IL-8, IL-17, G-CSF
- Key in non-T2 / severe asthma
- Found in sputum during severe exacerbations and fatal asthma (autopsy)
- Patients with neutrophilic asthma: more often female, obese, steroid-resistant
- Neutrophils release elastase → mucus production
T Lymphocytes (Th2 cells)
- Produce IL-4, IL-5, IL-13
- Critical mediators of allergic (T2) inflammation
- Th17 cells → IL-17 → neutrophil recruitment (non-T2 pathway)
ILC2 (Innate Lymphoid Cells type 2)
- Innate counterpart of Th2 cells
- Activated by alarmins (TSLP, IL-33, IL-25) without needing allergen sensitization
- Important in non-allergic eosinophilic asthma and severe asthma with nasal polyps
- More steroid-resistant than Th2 cells
Airway Epithelial Cells
- Act as barrier AND as initiators of inflammation
- In asthma: defective tight junctions → allergens penetrate more easily
- Decreased type I interferon production → increased viral susceptibility → exacerbations
- Reduced antioxidant defense → more oxidative damage
- Release alarmins (TSLP, IL-25, IL-33) → link epithelium to T2 and non-T2 inflammation
2.4 Molecular Mediators (Fishman's)
Cytokines
| Cytokine | Source | Function in asthma |
|---|---|---|
| IL-4 | Th2, ILC2 | IgE class switching in B cells |
| IL-5 | Th2, ILC2 | Eosinophil development, survival, recruitment |
| IL-13 | Th2, ILC2 | Mucus hypersecretion, AHR, IL-4Rα signaling |
| IL-8 (CXCL8) | Epithelium, macrophages | Neutrophil recruitment |
| IL-17 | Th17 | Neutrophilic inflammation |
| TSLP | Epithelium | Master alarm signal - activates DC, ILC2 |
| IL-33 | Epithelium | Activates ILC2, mast cells |
| IL-25 | Epithelium | Amplifies T2 responses |
Leukotrienes (Fishman's - arachidonic acid metabolites)
- Produced via 5-lipoxygenase pathway (FLAP is the activating protein)
- LTC4, LTD4, LTE4 → potent bronchoconstriction (much more potent than histamine)
- Also increase mucus secretion and vascular permeability
- Targeted by: LTRA (montelukast)
Prostanoids (from COX pathway)
- PGD2, PGF2a, TXA2 → bronchoconstrictors
- PGE2 → bronchodilatory (protective)
- PGD2 is the predominant prostanoid in asthma
- Acts via CRTH2 receptor on Th2 cells and ILC2 (target of fevipiprant)
Nitric Oxide (FeNO)
- Low levels: bronchodilator, protective
- High levels in asthma (iNOS upregulated by TSLP, IL-13)
- FeNO reflects eosinophilic airway inflammation → used as biomarker for T2 asthma
- Higher FeNO = more eosinophils in airway wall
Granule Proteins
| Protein | Cell | Function |
|---|---|---|
| MBP (major basic protein) | Eosinophil | BHR, epithelial damage |
| ECP (eosinophil cationic protein) | Eosinophil | Epithelial damage |
| EDN | Eosinophil | Neurotoxic |
| EPX | Eosinophil | Oxidative damage |
| Tryptase | Mast cell | Activates eosinophils, epithelium |
| Histamine | Mast cell/basophil | Bronchoconstriction, edema, itch |
2.5 Airway Remodeling (Fishman's - Chronic Changes)
"Irreversible structural changes occur in the airway in asthma that are collectively called 'airway remodeling.' This involves the chronic cycle of 'injury-repair.'" - Fishman's Ch. 43
Components:
- Epithelial changes - shedding, metaplasia, defective repair
- Subepithelial fibrosis - from TGF-β, fibroblast/myofibroblast activity
- Smooth muscle hypertrophy + hyperplasia - larger, more muscle → more bronchoconstriction
- Increased angiogenesis - new blood vessels
- Goblet cell hyperplasia - more mucus cells
Result: Persistent airflow obstruction that does not fully reverse even with maximum treatment
Key mechanism: EMTU (Epithelial-Mesenchymal Trophic Unit) - reactivation of fetal lung morphogenesis process in chronic asthma → TGF-β release → fibrosis
PART 3: ASTHMA PHENOTYPES (Fishman's)
Fishman's Chapter 43 describes at least 4 phenotypic clusters:
| Phenotype | Features |
|---|---|
| Eosinophilic-allergic | Atopic sensitization + eosinophilic inflammation (classic T2) |
| Eosinophilic-non-allergic | Eosinophilic but no atopy; often adult-onset |
| Highly symptomatic, minimal eosinophilia | Lots of symptoms, little inflammation; difficult to treat |
| Neutrophilic (non-T2) | Obese, female, steroid-resistant, severe |
Fishman's key quote: "The study of these factors has led to a greater understanding that different phenotypes of asthma exist, and treatment of asthma based on a patient's predominant phenotype may soon be possible."
PART 4: DIAGNOSIS
4.1 Symptoms (GINA 2026)
The classic quartet:
- Wheeze (musical, expiratory sound)
- Shortness of breath
- Chest tightness
- Cough (often worse at night / early morning)
Clues that strengthen diagnosis:
- Symptoms vary day to day, season to season
- Triggered by exercise, cold air, smoke, allergens, viral infections
- Respond to bronchodilators
- Personal/family history of atopy
4.2 Spirometry (GINA 2026)
| Finding | Significance |
|---|---|
| FEV1/FVC < 0.7 (or below LLN) | Obstructive defect |
| Post-BD FEV1 or FVC increase ≥12% AND ≥200 mL | Significant reversibility → supports asthma |
| Normal spirometry | Does NOT rule out asthma |
| PEF variability >10% | Supports asthma |
| PEF increase >20% after bronchodilator | Supports asthma |
4.3 Biomarkers (GINA 2026 - updated emphasis)
| Biomarker | What it means | Threshold |
|---|---|---|
| FeNO | T2 eosinophilic airway inflammation | >25 ppb supports T2 asthma |
| Blood eosinophils | T2 phenotype; predicts biologic response | >300/μL significant |
| Total IgE | Allergic phenotype | Elevated in allergic asthma |
| Periostin | IL-13 driven T2 inflammation | Emerging biomarker |
| Sputum eosinophils | Gold standard for eosinophil phenotyping | >3% abnormal |
4.4 Bronchial Provocation Testing
- When spirometry is normal but asthma suspected
- Methacholine challenge: Positive if PC20 ≤16 mg/mL (or ≤8 for some labs)
- Exercise challenge: >10% FEV1 fall
- Very sensitive (negative = asthma unlikely); less specific
4.5 Diagnosis in Children <5 years (GINA 2026 - all 3 required)
- Recurrent acute wheezing episodes
- No other likely cause for respiratory symptoms
- Timely clinical response to asthma medications
4.6 Differential Diagnosis
- COPD (fixed obstruction, older, smoker)
- Vocal cord dysfunction (inspiratory stridor, normal spirometry between episodes)
- Heart failure (cardiac asthma - elevated BNP, bilateral crackles)
- Bronchiectasis (daily productive cough)
- Cystic fibrosis (young, pancreatic, clubbing)
- GERD-related cough
- Hyperventilation syndrome
PART 5: ASSESSMENT
5.1 GINA 2026 - Symptom Control (ask about past 4 weeks)
| Question | Yes | No |
|---|---|---|
| Daytime symptoms >2x/week? | ||
| Any night waking due to asthma? | ||
| Reliever used >2x/week? | ||
| Any activity limitation? |
| Total "Yes" | Control Level |
|---|---|
| 0 | ✅ Well controlled |
| 1-2 | ⚠️ Partly controlled |
| 3-4 | ❌ Uncontrolled |
5.2 GINA 2026 - Severity (retrospective, after treatment)
| Severity | Treatment needed to stay controlled |
|---|---|
| Mild | Steps 1-2 |
| Moderate | Step 3 |
| Severe | Step 4-5, or remains uncontrolled despite it |
5.3 New GINA 2026 Assessment Tools
- CAAT (Chronic Airways Assessment Test) - NEW addition to GINA 2026
- Peds-AIRQ (Pediatric Asthma Impairment and Risk Questionnaire) - NEW for children
- PRAM (Pediatric Respiratory Assessment Measure) - for acute exacerbations in children
- Also: ACQ (Asthma Control Questionnaire), ACT (Asthma Control Test) - existing tools
5.4 Risk Factors for Exacerbations (GINA 2026)
- Uncontrolled symptoms
- Frequent SABA use
- Not on ICS
- Poor inhaler technique or adherence
- Smoking or allergen exposure
- Obesity, rhinosinusitis, GERD, pregnancy
- Low FEV1 (<60% predicted)
- Previous severe exacerbation or near-fatal asthma
5.5 Red Flags for Fatal/Near-Fatal Asthma (NEW - GINA 2026)
GINA 2026 added a dedicated list of red flags for fatal risk:
- Previous near-fatal asthma requiring intubation
- Hospital or ER visit for asthma in the past year
- Not currently using ICS
- Currently using or recently stopped OCS
- Over-reliance on SABA (using >1 canister/month)
- Psychiatric illness or psychosocial problems
- Poor adherence or no written action plan
- Food allergy + asthma
PART 6: TREATMENT - GINA 2026 STEPWISE APPROACH
6.1 The Two Tracks (BIG NEW CONCEPT - GINA 2026)
GINA 2026 formally organizes treatment into 2 tracks:
| Track 1 (PREFERRED) | Track 2 (Alternative) | |
|---|---|---|
| Reliever | As-needed low-dose ICS-formoterol | As-needed ICS-SABA (preferred) or SABA alone |
| Why preferred | ICS-formoterol reduces severe exacerbations by ~2/3 vs SABA alone; simplifies regimen (one inhaler) | Use if Track 1 not available/affordable/acceptable |
| MART | Yes (Steps 3-5: same ICS-formoterol used for maintenance AND relief) | No |
| Evidence | Budesonide-formoterol; beclometasone-formoterol | Lower evidence for some steps |
Key GINA 2026 message: ICS-formoterol as anti-inflammatory reliever (AIR) reduces severe exacerbations and hospitalizations by ~2/3 compared with SABA-alone treatment, even in patients considered "mild."
6.2 GINA 2026 - Treatment Steps (Track 1 - Preferred)
| Step | Maintenance Controller | Reliever |
|---|---|---|
| Step 1 | None (as-needed only) | As-needed low-dose ICS-formoterol |
| Step 2 | None OR low-dose ICS-formoterol (if more symptomatic) | As-needed low-dose ICS-formoterol |
| Step 3 | Low-dose ICS-formoterol daily (MART) | As-needed low-dose ICS-formoterol |
| Step 4 | Medium-dose ICS-formoterol daily (MART) | As-needed low-dose ICS-formoterol |
| Step 5 | High-dose ICS-formoterol ± add-on therapy + biologic if eligible | As-needed ICS-formoterol |
MART = Maintenance And Reliever Therapy - patient uses same inhaler for both daily maintenance AND as reliever when needed (only ICS-formoterol can be used this way).
6.3 GINA 2026 - Treatment Steps (Track 2 - Alternative)
| Step | Controller | Reliever |
|---|---|---|
| Step 1 | None | ICS-SABA (combination) or low-dose ICS whenever SABA taken |
| Step 2 | Low-dose ICS daily | As-needed ICS-SABA or SABA |
| Step 3 | Low-dose ICS-LABA daily | As-needed SABA or ICS-formoterol |
| Step 4 | Medium-high dose ICS-LABA | As-needed SABA; add LAMA |
| Step 5 | Add-on LAMA, phenotype-guided biologics | As-needed SABA |
6.4 Drug Classes - Simple Explanation
ICS (Inhaled Corticosteroids) - Most Important Drug
- Examples: Budesonide, Fluticasone (propionate + furoate), Beclometasone, Ciclesonide, Mometasone
- Action: Anti-inflammatory, reduce airway swelling, improve AHR
- Effect: Reduce symptoms, improve FEV1, reduce exacerbations and hospitalizations
- Key point from GINA 2026 Severe Asthma Guide: ICS are "the most effective anti-inflammatory medications for asthma"
LABA (Long-Acting Beta-2 Agonists)
- Examples: Formoterol (fast-onset), Salmeterol (slow-onset), Vilanterol
- Always combined with ICS - never alone in asthma
- Formoterol is special: fast-acting like SABA → can be used as reliever (basis of MART)
SABA (Short-Acting Beta-2 Agonists)
- Examples: Salbutamol (albuterol), Terbutaline
- Quick relief within minutes
- GINA 2026: Not recommended as sole reliever; overuse = poor control = danger
LAMA (Long-Acting Muscarinic Antagonists)
- Example: Tiotropium
- Add-on at Steps 4-5
- GINA 2026: Triple therapy (ICS-LABA-LAMA) reduces severe exacerbations less than biologic therapy but may benefit Step 5 patients who do not qualify for biologics
LTRA (Leukotriene Receptor Antagonists)
- Example: Montelukast
- Add-on at Steps 2-3
- Good for: aspirin-sensitive asthma, exercise-induced asthma, allergic rhinitis coexisting with asthma
OCS (Oral Corticosteroids) - Minimize!
- GINA 2026 new emphasis: Strongly recommends minimizing OCS use due to cumulative side effects
- Strategies: Treat modifiable risk factors, use ICS-formoterol as reliever, education, biologics first
- Short courses (5-7 days) acceptable for acute exacerbations
PART 7: BIOLOGICS (Step 5 - Severe Asthma)
7.1 Overview (GINA 2026 updates)
GINA 2026 emphasizes phenotype-based biologic selection using T2 biomarkers (blood eosinophils, FeNO, IgE) to guide choice.
7.2 Biologic Table (UPDATED GINA 2026)
| Drug | Target | Class | Key Indication | Dosing | NEW in 2026? |
|---|---|---|---|---|---|
| Omalizumab | Anti-IgE | Anti-IgE | Allergic asthma (elevated IgE + sensitization) | SC every 2-4 weeks | Biosimilar (omalizumab-igec) added |
| Mepolizumab | Anti-IL-5 | Anti-IL-5 | Severe eosinophilic (eos ≥150-300/μL) | SC monthly | - |
| Reslizumab | Anti-IL-5 | Anti-IL-5 | Severe eosinophilic (eos ≥400/μL) | IV every 4 weeks | - |
| Benralizumab | Anti-IL-5Rα | Anti-IL-5R | Severe eosinophilic (eos ≥300/μL) | SC monthly x3, then q8 weeks | - |
| Depemokimab | Anti-IL-5 | Anti-IL-5 | Severe eosinophilic (≥12y) + CRSwNP (≥18y) | SC twice yearly | ✅ NEW in GINA 2026 |
| Dupilumab | Anti-IL-4Rα | Anti-IL-4/13 | Eosinophilic OR OCS-dependent (any eos count) | SC every 2 weeks | - |
| Tezepelumab | Anti-TSLP | Anti-alarmin | Broad - T2 AND non-T2 (no biomarker cutoff) | SC monthly | - |
7.3 DEPEMOKIMAB - New Addition in GINA 2026 ⭐
- Ultra-long-acting anti-IL-5 monoclonal antibody
- Dosing: Subcutaneous injection TWICE YEARLY (every 6 months!) - major convenience advantage
- Approved for severe eosinophilic asthma (≥12 years)
- Also approved for CRSwNP (≥18 years)
- Added to GINA 2026
7.4 Non-Asthma Indications (NEW TABLE - GINA 2026)
GINA 2026 added a new table summarizing non-asthma indications for biologic classes:
| Biologic Class | Non-Asthma Indications |
|---|---|
| Anti-IgE | Chronic urticaria, food allergy |
| Anti-IL-5 / IL-5R | CRSwNP, eosinophilic granulomatosis with polyangiitis (EGPA), hypereosinophilic syndrome |
| Anti-IL-4Rα | Atopic dermatitis, CRSwNP |
| Anti-TSLP | CRSwNP |
7.5 Biologic Decision Tree (GINA 2026 Update)
GINA 2026 updated the decision tree for choosing a biologic:
- Check for Type 2 inflammation (blood eos, FeNO)
- Consider comorbidities (nasal polyps, atopic dermatitis, urticaria, EGPA)
- Consider practical issues: cost, administration route, dosing frequency, patient preference
- Consider predictors of response (higher eos/FeNO = better response to anti-IL-5/anti-IL-4)
PART 8: ACUTE EXACERBATIONS
8.1 Severity Assessment
| Feature | Mild-Moderate | Severe | Life-threatening |
|---|---|---|---|
| Talks in | Sentences | Phrases | Can't speak |
| Accessory muscles | No | Yes | Yes + paradoxical |
| RR | <25/min | >25/min | Variable |
| SpO2 (air) | >95% | 90-95% | <92% (GINA 2026 threshold) |
| PEFR | >50% | 33-50% | <33% |
| PaCO2 | Normal/low | Low | Rising = DANGER |
GINA 2026 Update: SpO2 threshold for urgent management = <92% (previously debated)
8.2 Acute Management (GINA 2026)
If SpO2 <92% on room air = urgent management:
- Bronchodilator: Repeated rapid-acting inhaled SABA (or ICS-formoterol as alternative to SABA in mild exacerbations per GINA 2026)
- +Ipratropium (SAMA): Add for severe exacerbations
- Oxygen: Controlled flow; target SpO2 93-95%
- Systemic corticosteroids: Oral prednisolone 40-50 mg/day OR IV hydrocortisone; 5-7 days
- Magnesium sulfate IV: For severe exacerbations not responding; improves FEV1 and reduces hospitalization
8.3 NEW GINA 2026 Exacerbation Flowcharts
- New primary care flowcharts for managing exacerbations
- ICS-formoterol as alternative to SABA for mild exacerbations - can reduce need for OCS
8.4 Discharge Checklist (GINA 2026)
- ✅ Start/adjust ICS-containing controller
- ✅ Verify/step up to ICS-formoterol reliever
- ✅ Check inhaler technique (new GINA 2026 guidance on single-breath + tidal breathing techniques)
- ✅ Address triggers/modifiable risk factors
- ✅ Written asthma action plan
- ✅ Follow-up within 1 week
PART 9: SPECIAL SITUATIONS
9.1 Vaccines (GINA 2026 Updated Evidence)
- Influenza vaccine: Recommended annually for all asthmatics
- RSV vaccine: Updated evidence incorporated in GINA 2026
- COVID-19 vaccine: Updated evidence incorporated in GINA 2026
- Vaccines reduce exacerbation risk in patients susceptible to viral triggers
9.2 GLP-1 Agonists (GINA 2026 - New Observation)
- Observational data (not yet definitive) suggesting GLP-1 agonists (like semaglutide) may improve asthma outcomes
- Likely mechanism: weight loss reduces obesity-related asthma
- GINA 2026 notes "potential future role" - watch this space
9.3 Asthma in Pregnancy
- Uncontrolled asthma > drug risk to fetus
- Continue ICS - budesonide is most-studied and preferred
- Step approach same as non-pregnant adults
9.4 Aspirin/NSAID-Exacerbated Asthma (AERD)
- Samter's Triad: Asthma + nasal polyps + aspirin sensitivity
- Add LTRA (montelukast) - blocks LTE4 pathway triggered by aspirin
- Consider aspirin desensitization
- Biologics effective (dupilumab, mepolizumab, tezepelumab also cover CRSwNP)
9.5 Allergic Bronchopulmonary Aspergillosis (ABPA)
- Fungal sensitization in asthma → extremely difficult to control
- GINA 2026: OCS ± antifungal agent
- Consider biologics for underlying eosinophilic asthma
PART 10: INHALER TECHNIQUE (NEW GUIDANCE - GINA 2026)
GINA 2026 added specific guidance on two MDI techniques:
| Technique | How | When |
|---|---|---|
| Single-breath technique | Slow, deep inhalation over ~3-5 seconds after actuating MDI; hold for 10 seconds | Standard MDI use |
| Tidal breathing technique | Normal breathing through spacer after actuating; for those who can't coordinate single breath | Children, elderly, poor coordination |
- Spacer recommended with pMDI for all patients
- Check technique at EVERY clinic visit
PART 11: GINA 2026 KEY UPDATES SUMMARY
| Update | What Changed |
|---|---|
| Anti-inflammatory reliever | ICS-formoterol or ICS-SABA recommended at ALL steps; SABA-only no longer acceptable |
| SpO2 threshold | <92% = urgent management trigger (updated) |
| SABA dose | Updated recommended doses for SABA therapy |
| Depemokimab | NEW biologic added (anti-IL-5, twice yearly) |
| Omalizumab biosimilar | Generic anti-IgE (omalizumab-igec) listed |
| Biologic decision tree | Updated with new drugs and comorbidity guidance |
| Non-asthma indications table | NEW table for 4 biologic classes |
| New assessment tools | CAAT, Peds-AIRQ, PRAM added |
| Inhaler technique | Single-breath + tidal breathing MDI details added |
| New exacerbation flowcharts | Primary care & ER management flowcharts |
| OCS minimization | Strong emphasis on avoiding cumulative OCS |
| Fatality red flags | New dedicated list of fatal asthma risk factors |
| Vaccines | Updated influenza, RSV, COVID-19 evidence |
| GLP-1 agonists | Observational data on potential benefit noted |
| Triple therapy | Less effective than biologics at Step 5 but useful when biologics not accessible |
| Pediatric exacerbations | Validated severity score strongly recommended |
QUICK MEMORY AIDS
FISHMAN'S ASTHMA CORE = 3 Bs
B - Bronchoconstriction (variable, reversible airflow obstruction)
B - Bronchial Hyperresponsiveness (airway overreacts to triggers)
B - Bronchial inflammation (Chronic, T2 or non-T2)
INFLAMMATORY CELLS = MELT BEN
M - Mast cells (early phase)
E - Eosinophils (late phase, T2)
L - Lymphocytes (Th2 = IL-4/5/13; Th17 = neutrophils)
T - Th2 cells
B - Basophils
E - Epithelial cells (alarmins)
N - Neutrophils (severe/non-T2)
GINA 2026 CONTROL (past 4 weeks, 4 questions):
0 YES = Well controlled ✅
1-2 YES = Partly controlled ⚠️
3-4 YES = Uncontrolled ❌
GINA 2026 TRACKS:
Track 1 (PREFERRED) = ICS-formoterol as reliever at ALL steps
Track 2 (Alternative) = ICS-SABA or SABA as reliever
NEW BIOLOGIC 2026 = DEPEMOKIMAB
- Anti-IL-5
- Twice yearly (6-monthly) dosing
- ≥12 years for severe eosinophilic asthma
Sources:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (ISBN 9781260473940) - Chapter 43: Pathophysiology of Asthma
- GINA 2026 Global Strategy Report - Published May 5, 2026
- GINA 2026 Severe Asthma Guide v7.0 - May 2026
- GINA 2026 Key Updates Summary - Pulmonology Advisor
This is a shared conversation. Sign in to Orris to start your own chat.