Fever with rash life threatening causes, er approach and management
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"fever AND rash" AND "emergency" AND "life threatening"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
purpura fulminans meningococcemia rash
Reading File
Finding Sources
Searching Images
Rocky Mountain spotted fever petechial rash wrists ankles
Reading File
Reading File
I now have comprehensive material. Let me compose the full clinical answer.
Fever with Rash: Life-Threatening Causes, ER Approach & Management
⚠️ The Critical Principle
Fever + rash in any acutely ill patient must first exclude life-threatening diagnoses. As Goldman-Cecil states: "The presence of an acute fever and rash should prompt exclusion of life-threatening diseases." The rash morphology is the primary diagnostic navigator.
Part 1: Classify by Rash Morphology
| Morphology | Key Life-Threatening Diagnoses |
|---|---|
| Petechial / Purpuric | Meningococcemia, RMSF, DIC/purpura fulminans, endocarditis, TTP |
| Maculopapular | RMSF (early), secondary syphilis, meningococcemia (early), DRESS |
| Diffuse erythroderma | Toxic shock syndrome (staph/strep), SSSS, necrotizing fasciitis |
| Vesiculobullous / Skin sloughing | Stevens-Johnson syndrome / TEN, SSSS, necrotizing fasciitis |
| Retiform / stellate purpura | Purpura fulminans, vasculitis, meningococcemia (advanced) |
Part 2: The Life-Threatening Diagnoses in Detail
1. Meningococcemia / Purpura Fulminans
Organism: Neisseria meningitidis
Rash: Begins as a maculopapular eruption → rapidly becomes petechial then purpuric, non-blanching. Purpura fulminans = rapidly spreading ecchymoses and gangrene of the extremities, the most advanced form, usually with DIC.

Clinical features: High fever, headache, meningismus (may be absent in rapid septicemia), photophobia. Mucosal/GI bleeding, oozing from IV sites. Shock from distributive mechanism + myocarditis + intravascular volume loss. Bilateral adrenal hemorrhage (Waterhouse-Friderichsen syndrome), renal failure, coma.
Poor prognostic signs: WBC <500/mm³, platelets <100,000/mm³, pH <7.30, petechiae within 12 h, absence of meningitis, purpura fulminans, shock.
Management:
- Immediate penicillin G or ceftriaxone 2g IV — do NOT delay for LP if meningitis suspected
- Blood cultures × 2 before antibiotics if possible, but never delay treatment
- Aggressive IV fluid resuscitation; vasopressors (norepinephrine) for refractory shock
- ICU admission; treat DIC (FFP, platelets)
- Dexamethasone 0.15 mg/kg q6h IV for suspected bacterial meningitis (before or with first antibiotic dose)
- Droplet precautions; prophylaxis for close contacts (rifampicin, ciprofloxacin, or ceftriaxone)
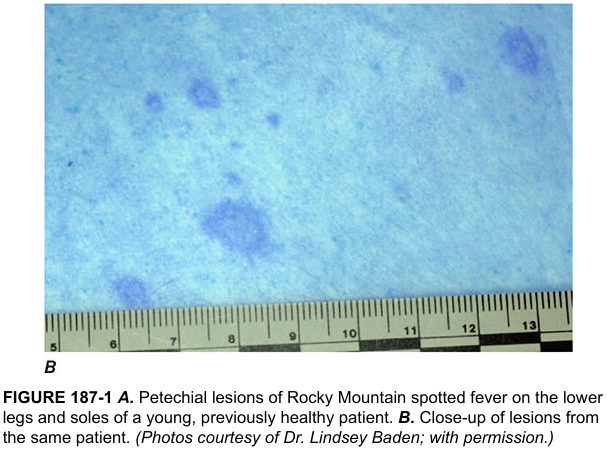
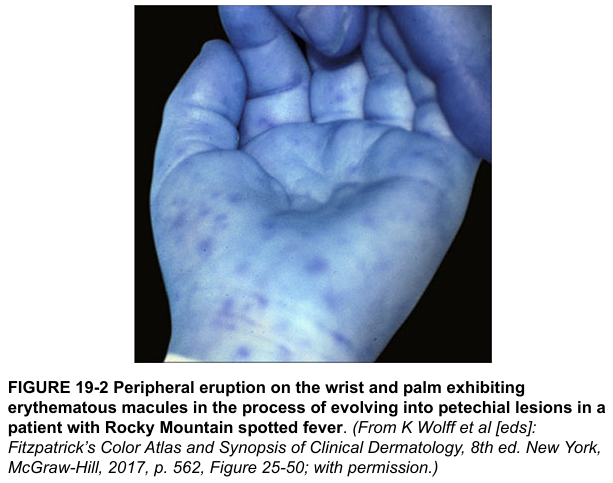
2. Rocky Mountain Spotted Fever (RMSF)
Organism: Rickettsia rickettsii (tick-transmitted)
Rash: Appears day 2–6 of illness. Begins as erythematous blanching macules on the wrists and ankles → spreads centripetally to trunk and face → becomes petechial/hemorrhagic. Involvement of palms and soles is characteristic.
Clinical features: Abrupt fever, headache, myalgia, nausea/vomiting. CNS involvement, DIC, hepatitis, ARDS, myocarditis, renal failure. Many patients do not report tick exposure.
Critical point: Diagnosis is clinical. Definitive serology is not available acutely in the ED — treat empirically.
Management:
- Doxycycline 100 mg IV/PO q12h — first-line in ALL ages (including children). Delay dramatically increases mortality.
- Chloramphenicol is an alternative only for severe tetracycline allergy (not preferred, especially in children <9 yr anymore — doxycycline is now recommended for all)
- Avoid: sulfa drugs (exacerbate illness); Rickettsia is resistant to penicillins, cephalosporins, aminoglycosides, erythromycin
- Ehrlichiosis is clinically similar and also treated with doxycycline
3. Toxic Shock Syndrome (TSS)
Organisms: Staphylococcus aureus (staphylococcal TSS) or Streptococcus pyogenes (streptococcal TSS) — superantigen-mediated
Rash: Diffuse blanching macular erythroderma (sunburn-like), with nonexudative mucosal inflammation — "strawberry tongue," conjunctivitis, vaginitis. Rash fades within 3 days, followed by full-thickness desquamation of palms and soles 1–2 weeks later.
CDC Case Definition (Staphylococcal TSS):
- Fever ≥38.9°C
- Diffuse macular erythroderma
- Desquamation 1–2 weeks later
- Hypotension (SBP ≤90 mmHg)
- Multisystem involvement (≥3 organ systems): GI, muscular, mucous membranes, renal, hepatic, hematologic (platelets <100,000), CNS
Associations: Menstruation (tampon use), postoperative wounds, burns, postpartum, fasciitis, septic abortion, soft tissue infections.
Management:
- Remove the source (remove tampon, drain abscess, debride wound)
- Aggressive IV fluid resuscitation; vasopressors for shock
- Empirical antibiotics covering MRSA and S. pyogenes:
- Vancomycin + clindamycin (clindamycin reduces toxin production via ribosomal inhibition — a key adjunct)
- Alternatives: linezolid, piperacillin-tazobactam, meropenem
- IVIG 1–2 g/kg single dose in refractory shock (neutralizes superantigens) — considered in severe/refractory cases
- ICU admission, ventilatory support as needed
4. Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)
Trigger: Predominantly drugs (sulfonamides, anticonvulsants, allopurinol, NSAIDs, lamotrigine); also infections (Mycoplasma, HSV)
Rash: Begins as dusky or target-like maculopapular lesions → blistering → epidermal detachment. SJS = <10% BSA; TEN = >30% BSA; overlap = 10–30%.
Clinical features: Fever (often 38–40°C), malaise, painful burning skin, mucosal involvement (oral, genital, ocular) is characteristic and differentiates from other blistering disorders. Positive Nikolsky sign.
Management:
- Stop the causative drug immediately — this is the single most important intervention
- Transfer to burn unit or ICU
- Wound care (non-adherent dressings), fluid/electrolyte replacement
- Ophthalmology consult (prevent ocular sequelae)
- Do NOT use systemic corticosteroids (controversial; may increase mortality)
- Cyclosporine, IVIG, or anti-TNF agents (etanercept, infliximab) used in severe cases
- SCORTEN score guides prognosis and ICU triage
5. Necrotizing Fasciitis
Often overlooked — rash may appear deceptively benign initially (erythema, swelling) on one extremity.
Clinical features: Rapidly spreading erythema, severe disproportionate pain, skin appears normal early → progresses to bullae, skin necrosis, crepitus, violaceous discoloration, systemic sepsis. Often associated with Group A Strep or polymicrobial.
Management:
- Emergent surgical consultation for immediate wide debridement — this is the key intervention
- Broad-spectrum IV antibiotics: piperacillin-tazobactam + clindamycin + vancomycin
- ICU admission, resuscitation
6. Disseminated Gonococcemia / Endocarditis with Septic Emboli
Gonococcal: triad of polyarthralgia, tenosynovitis, and dermatitis — pustular or vesiculopustular lesions on the distal extremities, may be hemorrhagic. Treat with ceftriaxone.
Endocarditis: septic emboli appear as purpuric or necrotic lesions (gunmetal-gray), Osler nodes, Janeway lesions. Requires blood cultures × 3 before empiric vancomycin + gentamicin.
Part 3: ER Approach Algorithm
FEVER + RASH → Acutely ill? → YES → TREAT AS EMERGENCY
Step 1: RAPID ASSESSMENT (< 5 min)
├─ Airway, breathing, circulation, mental status
├─ IV access × 2 + monitoring + O₂
└─ Is patient in SHOCK? → Start resuscitation simultaneously
Step 2: RASH CHARACTERIZATION (Bedside)
├─ Petechial/purpuric/non-blanching?
│ → Meningococcemia, RMSF, DIC, endocarditis
│ → Draw blood cultures, give ceftriaxone NOW
├─ Diffuse erythroderma + mucous membrane involvement?
│ → TSS: remove source, vancomycin + clindamycin
├─ Blistering / skin detachment + mucosal lesions?
│ → SJS/TEN: stop offending drug, dermatology/burns
└─ Unilateral extremity pain, erythema, crepitus?
→ Necrotizing fasciitis: surgical consult STAT
Step 3: TARGETED HISTORY
└─ Tick exposure? (RMSF/Ehrlichiosis)
└─ Recent drugs? (SJS/TEN/DRESS)
└─ Tampon/wound/postoperative? (TSS)
└─ Sexual contacts? (Gonococcemia)
└─ Travel? Immunosuppression? Animal exposures?
Step 4: INVESTIGATIONS (DO NOT DELAY TREATMENT)
├─ CBC, BMP, LFTs, coagulation (PT/PTT/fibrinogen/D-dimer)
├─ Blood cultures × 2–3
├─ Wound/mucosal cultures, throat swab
├─ LP if meningococcemia suspected (after CT if focal neuro signs)
└─ Skin biopsy (if stable — Rickettsia immunofluorescence, SJS)
Step 5: EMPIRICAL TREATMENT (while awaiting results)
└─ See table below
Part 4: Empirical Treatment Summary Table
| Diagnosis | First-Line Treatment | Key Adjuncts |
|---|---|---|
| Meningococcemia | Ceftriaxone 2g IV q12h | Dexamethasone; ICU; close-contact prophylaxis |
| RMSF / Ehrlichiosis | Doxycycline 100mg IV/PO q12h | Do NOT wait for serology |
| Staph TSS | Vancomycin + Clindamycin IV | Remove source; IVIG in refractory cases |
| Strep TSS | Penicillin G + Clindamycin IV | IVIG; surgical debridement if NF |
| SJS / TEN | Stop drug; supportive care | Burns unit; ophthalmology; cyclosporine/IVIG |
| Necrotizing Fasciitis | Pip-tazo + Clindamycin + Vancomycin | EMERGENCY debridement |
| Gonococcemia | Ceftriaxone 1g IV daily | Treat partners; rule out endocarditis |
| Bacterial Endocarditis | Vancomycin + Gentamicin | Echo; blood cultures × 3 before antibiotics |
The Non-Negotiable Rules in the ER
- Petechial rash + fever = meningococcemia until proven otherwise — antibiotics before LP, before CT, before almost everything
- RMSF: treat empirically with doxycycline — waiting for serology kills patients; "failure to administer antibiotics in a timely fashion dramatically increases morbidity and mortality" — Rosen's Emergency Medicine
- SJS/TEN: stop the drug immediately — the most critical single action
- TSS: source control first — antibiotic alone is insufficient without removing the infected focus
- Necrotizing fasciitis: operate, not just observe — no amount of antibiotics replaces surgical debridement
Sources: Rosen's Emergency Medicine (10th ed.), Harrison's Principles of Internal Medicine (22nd ed., 2025), Goldman-Cecil Medicine, Fitzpatrick's Dermatology.
TSS pathophysiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
superantigen mechanism MHC class II T cell receptor Vbeta toxic shock syndrome diagram
Loading Image
Loading Image
I have all the essential material. Here is a comprehensive, mechanistically thorough answer.
Toxic Shock Syndrome — Pathophysiology
The Core Concept: Superantigen-Driven Immune Catastrophe
TSS is not caused by direct bacterial invasion of tissue. It is a toxin-mediated systemic inflammatory response driven by proteins called superantigens — exotoxins that hijack the adaptive immune system to trigger a massive, dysregulated cytokine storm.
Step 1: Normal Antigen Presentation vs. Superantigen Action
Normal T-cell activation requires a peptide antigen to be processed intracellularly by an APC, loaded into the groove of an MHC class II molecule, and then recognized by the precise CDR3 region of the TCR αβ heterodimer. This activates only the ~0.01–0.1% of T cells that are antigen-specific.
Superantigens bypass this entirely.
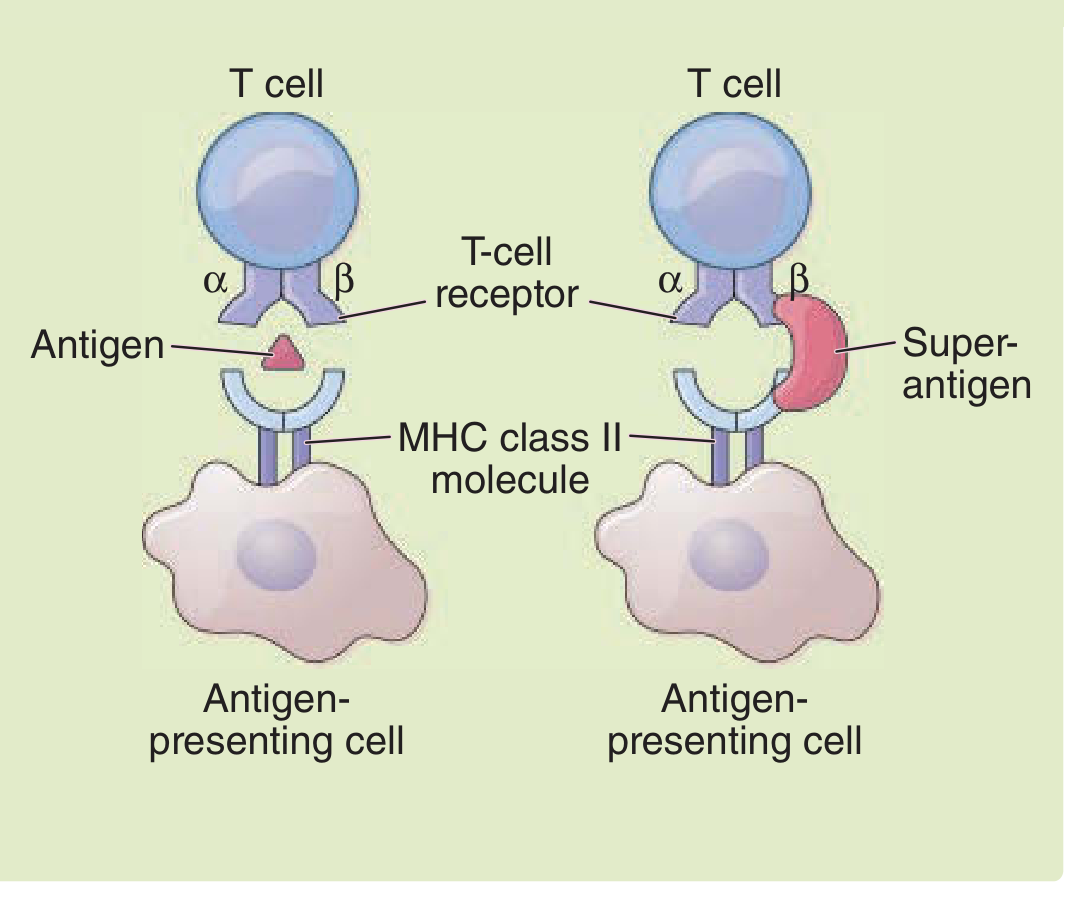
A superantigen:
- Does not require processing by the APC
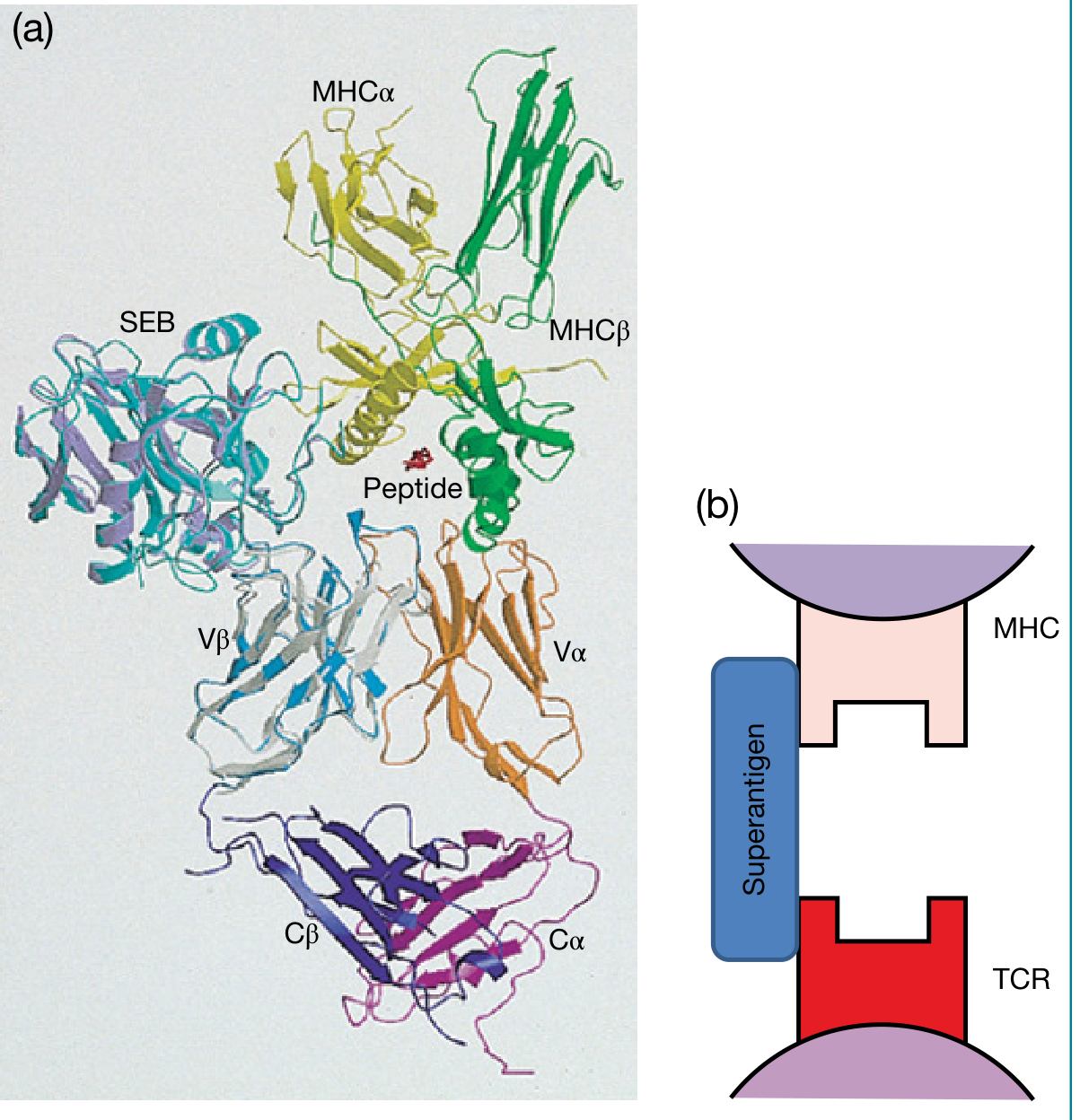
- Binds outside the peptide-binding groove of MHC class II (to the α or β chain of MHC on the outer wall)
- Simultaneously binds the Vβ region of the TCR β chain — a region shared by entire T-cell families, not the antigen-specific CDR3
Because many different T-cell clones share the same Vβ family structure, a single superantigen can activate 5–20% of the entire circulating T-cell pool simultaneously — compared to 0.01–0.1% in a normal immune response. This is the basis of the "cytokine storm."
Step 2: The Causative Toxins
Staphylococcal TSS
| Toxin | Characteristics |
|---|---|
| TSST-1 (Toxic Shock Syndrome Toxin-1) | Predominant toxin in menstrual TSS; unique ability to cross mucosal surfaces |
| Staphylococcal Enterotoxin B (SEB) | Most potent T-cell mitogen known — active at 10⁻¹³–10⁻¹⁶ M |
| Staphylococcal Enterotoxin C (SEC) | SEB + SEC account for ~50% of non-menstrual TSS |
TSST-1 is produced by S. aureus strains growing on mucous membranes (e.g., vagina during menstruation, postoperative wounds). Blood and protein from the tampon neutralize the normally bactericidal acidic vaginal pH, creating an ideal environment for TSST-1 production.
Host susceptibility factor: Patients who lack pre-existing neutralizing antibodies against TSST-1 are at markedly increased risk. Most adults develop protective antibody titers by adulthood — explaining why TSS is more common in young women encountering their first exposure.
Streptococcal TSS
| Toxin | Role |
|---|---|
| SPEA (Streptococcal Pyrogenic Exotoxin A) | Majority of strep TSS cases |
| SPEB | Cysteine protease; cleaves pre-IL-1β → active IL-1β; contributes to necrotizing fasciitis |
| SPEC, SSA, mitogenic factor | Additional superantigenic contributors |
Streptococcal pyrogenic exotoxins act as superantigens binding Vβ elements of the TCR without classic antigen processing, causing massive clonal proliferation of T lymphocytes and macrophage stimulation.
Strep TSS is actually more common than staph TSS: 2–4 cases vs 0.3–0.5 cases per 100,000 population respectively. Blood cultures are positive in >50% of strep TSS, versus only ~10% of staph TSS. — Fitzpatrick's Dermatology
Step 3: The Cytokine Storm
Once superantigens bridge MHC class II on APCs to TCR Vβ on T cells:
Superantigen + MHC class II (APC) + TCR Vβ (T cell)
↓
Massive polyclonal T-cell activation (5–20% of T-cell pool)
↓
Explosive release of:
• IL-2 (T cells) → fever, T-cell proliferation
• IFN-γ (T cells) → macrophage activation
• TNF-α (macrophages) → fever, hypotension, shock
• TNF-β / Lymphotoxin (T cells) → tissue damage
• IL-1 (macrophages) → fever, endothelial damage
• IL-6 (macrophages) → acute phase response, fever
Additionally:
- Mast cells release leukotrienes (vasoactive)
- Strep exotoxins potentiate endotoxin-induced shock and may suppress antibody synthesis
Step 4: From Cytokine Storm → Clinical Manifestations
CYTOKINE STORM (TNF-α, IL-1, IL-6, IFN-γ)
│
├──→ ENDOTHELIAL INJURY
│ ↓
│ Capillary leak syndrome
│ ↓ ↓
│ Tissue edema Intravascular volume depletion
│ ↓
│ HYPOTENSION / SHOCK
│
├──→ FEVER (IL-1, IL-6, TNF acting on hypothalamus)
│
├──→ RASH (diffuse macular erythroderma)
│ CLA+ T cells (skin-homing) traffic to skin → erythroderma
│ Later: full-thickness desquamation (palms & soles, 1–2 wk)
│
├──→ MULTIORGAN DYSFUNCTION
│ • Renal: ischemia from hypoperfusion + direct cytokine injury
│ • Hepatic: TNF-mediated hepatocyte injury
│ • Hematologic: thrombocytopenia, DIC
│ • CNS: altered consciousness (toxin + hypoperfusion)
│ • Muscular: myositis (creatine kinase elevation)
│
└──→ MUCOUS MEMBRANE INFLAMMATION
Strawberry tongue, conjunctivitis, vaginitis
(direct cytokine effect + toxin crossing mucosal barriers)
Why skin homing?
Superantigen-stimulated T cells generate increased numbers of CLA-positive (Cutaneous Lymphocyte Antigen) T cells — the subset that traffics preferentially to skin. This explains the disproportionately high cutaneous manifestations of TSS compared to other forms of sepsis. — Fitzpatrick's Dermatology
Step 5: Staphylococcal vs. Streptococcal TSS — Key Pathophysiological Differences
| Feature | Staph TSS | Strep TSS |
|---|---|---|
| Primary toxins | TSST-1, SEB, SEC | SPEA, SPEB, SPEC |
| Bacteremia | Rare (~10%) | Common (>50%) |
| Entry site | Mucous membranes, wounds | Any invasive GAS infection |
| Association with NF | Not typical | Frequently complicated by necrotizing fasciitis/myositis |
| SPEB special role | — | Cleaves pre-IL-1β → active IL-1β; direct tissue destruction via cysteine protease activity |
| Age group | Young women (menstrual); any age (non-menstrual) | Otherwise healthy adults; young, elderly, immunocompromised |
| Rash | Classic diffuse erythroderma ± desquamation | May be less prominent; local infection signs dominate |
Step 6: Why Clindamycin is Used (Mechanistic Basis)
Standard beta-lactams kill bacteria but do not reduce ongoing toxin production. Clindamycin inhibits the 50S ribosomal subunit → directly suppresses toxin (TSST-1, SPE) synthesis by the bacterial ribosome. This is why clindamycin is always added to primary antibiotic coverage in TSS, regardless of susceptibility — its value is in toxin suppression, not bacterial killing.
Similarly, IVIG works by providing pre-formed neutralizing antibodies against the superantigens (TSST-1, SPEs), directly blocking their ability to crosslink MHC-II and TCR Vβ, thereby dampening the cytokine storm.
Summary Diagram
S. aureus / GAS
(at mucosal surface, wound, soft tissue)
↓
Toxin production (TSST-1 / SPEA / SPEB)
↓
Superantigen bridges:
MHC class II (APC) ←→ TCR Vβ (T cell)
[BYPASSES normal antigen processing]
↓
5–20% of T cells activated simultaneously
↓
Cytokine storm: IL-2, TNF-α, TNF-β, IFN-γ, IL-1, IL-6
↓
┌──────────────────────────────────────────┐
│ Capillary leak → hypovolemia → shock │
│ Endothelial damage → multiorgan failure │
│ CLA+ T cells to skin → erythroderma │
│ Hypothalamic prostaglandins → fever │
│ Mucous membrane inflammation │
│ Desquamation at 1–2 weeks │
└──────────────────────────────────────────┘
Sources: Fitzpatrick's Dermatology (Vol. 1–2); Roitt's Essential Immunology; Goldman-Cecil Medicine; Medical Microbiology (Murray, 9th ed.); Rosen's Emergency Medicine (10th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.