
42d6c41f-4158-4b52-8f04-ad00839a24d1.jpeg
Silver
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Answer: 4 - Urethral Diverticulum
Why Urethral Diverticulum?
The classic features of this case all point to urethral diverticulum:
| Feature in Case | Explanation |
|---|---|
| 50-year-old woman | UD is almost exclusively diagnosed in adult females |
| Chronic burning/dysuria | Classic symptom - part of the "3 Ds": Dysuria, Dyspareunia, Dribbling |
| Cystic periurethral mass, ~1 cm | UD is defined as a urine-filled cystic periurethral structure connected to the urethra |
| Mass shifts meatus to the right | The cystic sac exerts mass effect, displacing the urethra/meatus laterally |
According to Smith and Tanagho's General Urology:
"A urethral diverticulum is a urine-filled periurethral cystic structure connected to the urethra through an ostium." "The diagnosis is usually made on feeling a rounded cystic mass in the anterior wall of the vagina... symptoms include irritative voiding symptoms and dysuria."
Why Not the Others?
1. Urethral caruncle - This is a small, fleshy, benign outgrowth at the posterior lip of the urethral meatus. It is typically red/vascular, NOT cystic, and doesn't displace the meatus. Common in postmenopausal women but presents as a visible external exophytic lesion, not a sub-urethral cystic mass.
2. Skene gland abscess (Scan gland abscess) - Skene (paraurethral) gland abscesses are typically acute, tender, and present at the distal urethral opening bilaterally. They are abscesses, not cystic masses, and do not characteristically displace the meatus.
3. Gartner duct cyst - Arises from a remnant of the mesonephric (Wolffian) duct along the anterolateral walls of the vagina. It is a vaginal wall cyst, NOT a periurethral cystic mass, and would not cause dysuria or meatal displacement in this manner.
The key distinguishing clue is the cystic periurethral mass + meatal displacement + dysuria in a middle-aged woman - this is textbook urethral diverticulum. The textbook explicitly lists Gartner duct cysts and Skene gland cysts/abscesses in the differential diagnosis of UD, confirming the exam question is testing this discrimination.
- Smith and Tanagho's General Urology, 19th Ed.
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have everything needed to give a comprehensive answer. The flowchart from Campbell Walsh Wein Urology and the surrounding text make the answer very clear.
Answer: d) A 6-year-old girl with right kidney parenchymal laceration of 2.5 cm due to gunshot trauma
Here is the kidney trauma algorithm from Campbell Walsh Wein Urology that explains the reasoning:
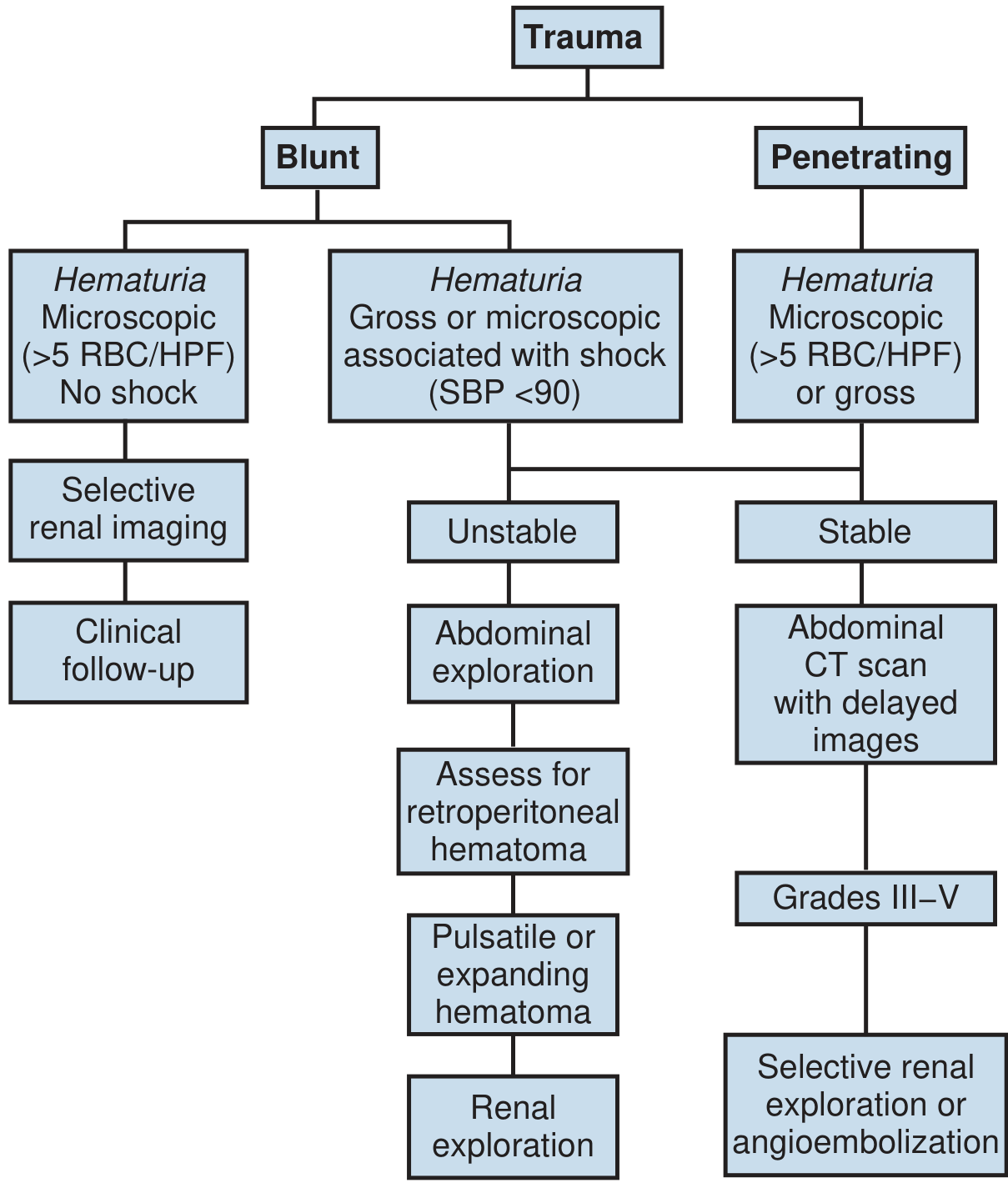
Why is option (d) correct?
Gunshot wounds = penetrating trauma. Following the algorithm's right-side branch (Penetrating):
- Any hematuria (microscopic or gross) in penetrating trauma triggers CT imaging
- If stable - CT is done with delayed images
- Grades III-V penetrating injuries → "Selective renal exploration or angioembolization"
A 2.5 cm parenchymal laceration from a gunshot = AAST Grade III (laceration >1 cm depth) or higher. Per the textbook:
"High grade penetrating injuries (AAST grade III or IV) are typically managed surgically because of the high rate of delayed bleed (24%) and the necessity to explore for associated intra-abdominal injuries."
The gunshot mechanism is key - it is a high-energy penetrating injury that violates the retroperitoneum and risks injuring adjacent structures. Even when the kidney injury alone might look manageable, the trajectory demands surgical exploration.
Why the others are WRONG?
| Option | Why NOT emergency OR exploration |
|---|---|
| (a) 45-yr man, bilateral Grade 3, motorcycle (blunt) | Grade 3 blunt - hemodynamically stable - nonoperative management is standard for blunt Grades I-IV |
| (b) 30-yr woman, BP 110/80, "shattered" kidney (blunt) | BP 110/80 = hemodynamically stable - even shattered (Grade V) blunt kidneys can be managed non-operatively if stable. Surgery is triggered by hemodynamic instability (SBP <90), not grade alone in blunt trauma |
| (c) 18-yr man, urinary extravasation, stab wound | Urinary extravasation per the key points: "Kidney injuries with urinary extravasation can often be managed conservatively and resolve spontaneously." Stab wounds have strong evidence for conservative management in stable patients |
The fundamental principle:
-
Blunt + stable = almost always nonoperative (even high grade)
-
Penetrating (gunshot) + Grade III+ = requires exploration due to trajectory, associated injuries, and high delayed-bleed risk
-
Campbell Walsh Wein Urology, Fig. 90.7 and Nonoperative Management section
-
Sabiston Textbook of Surgery, 39th Ed - Management of Renal Trauma

c2715dc6-15ad-47f7-b26d-bcbe3f685362.jpeg
Options are ESWL RIRS PCNL FOLLOWUP
Finding Sources
Finding Sources
Reading File
Reading File
The table is definitive. Here is the complete answer:
Answer: PCNL (Percutaneous Nephrolithotomy)
The Key Table (AUA/Endourological Society Guidelines)
| Stone Characteristic | First-Line Treatment |
|---|---|
| Non-lower pole stone <20 mm | ESWL or URS |
| Non-lower pole stone >20 mm | PCNL |
| Lower pole stone <10 mm | ESWL or URS |
| Lower pole stone >10 mm | PCNL or URS |
This patient has an 18 mm stone in the lower calyx - which places her squarely in the "lower pole stone >10 mm" category → PCNL is first-line.
Why PCNL specifically over URS (RIRS)?
The question uses the phrasing "the reference book," which typically refers to Campbell Walsh Wein or Smith & Tanagho. The guideline-recommended first-choice for lower pole stones >10 mm is PCNL, with the strongest evidence. The textbook explicitly states:
"An RCT has shown that for lower pole stones greater than 10 mm, PCNL has much better clearance rates than ESWL (92% vs. 23%)."
RIRS (retrograde intrarenal surgery / flexible URS) is an alternative but not the first-line preferred choice for an 18 mm lower calyx stone per standard guidelines.
Why Not the Other Options?
| Option | Reason to Reject |
|---|---|
| ESWL | Poor clearance from lower pole - fragments don't drain well due to gravity; RCT shows only 23% stone-free rate vs 92% for PCNL in lower pole stones >10 mm |
| RIRS | Acceptable alternative, but PCNL is the preferred first-line for lower pole >10 mm; stone-free rates with flexible URS are similar to ESWL for lower pole stones |
| Follow-up | An 18 mm stone is too large for expectant management - it will not pass spontaneously and carries risks of obstruction, infection, and renal damage |
- Comprehensive Clinical Nephrology, 7th Ed., Table 63.3 (AUA/Endourological Society Guideline)
This is a shared conversation. Sign in to Orris to start your own chat.