MRI knee anatomy pdf to reach students with diagrams and images
Reading File
search_medical_text
MRI knee anatomy structures ligaments menisci cartilage
search_medical_text
knee MRI sequences planes imaging protocol education
search_medical_image
MRI knee anatomy labeled structures sagittal coronal axial
GradeResponse
GradeResponse
GradeResponse
search_medical_image
knee MRI anatomy
search_medical_text
knee anatomy cruciate ligaments meniscus patella tibia femur
GradeResponse
GradeResponse
search_medical_text
ACL PCL MCL LCL meniscus tear MRI appearance diagnosis
search_medical_image
knee ligament meniscus MRI sagittal coronal
GradeResponse
GradeResponse
Now I have enough to build a comprehensive, well-structured educational guide. Here is your MRI Knee Anatomy — Student Teaching Guide, formatted as a complete PDF-ready document:
🦴 MRI Knee Anatomy
A Student Teaching Guide — Structures, Sequences & Pathology
1. Introduction to Knee MRI
MRI is the gold standard for evaluating knee soft tissues. It images fascia, vessels, nerves, muscle, cartilage, ligaments, tendons, synovial effusions, and bone marrow with superior soft-tissue resolution compared to arthrography or CT (Harrison's Principles of Internal Medicine, 21st Ed., p. 10396).
Why MRI for the Knee?
| Feature | MRI Advantage |
|---|---|
| Ligaments (ACL, PCL, MCL, LCL) | Direct visualization, tear grading |
| Menisci | Detects tears of all configurations |
| Cartilage | Assesses thickness, fissuring, loss |
| Bone marrow | Osteonecrosis, stress reactions |
| Soft tissue | Bursae, cysts, tendon pathology |
2. The Three Compartments of the Knee
The knee is a synovial hinged joint with three compartments (Bailey & Love's Surgery, 28th Ed., p. 511):
┌─────────────────────────────────┐
│ 1. Medial compartment │
│ 2. Lateral compartment │
│ 3. Patellofemoral compartment │
└─────────────────────────────────┘
Bones involved: Distal femur · Proximal tibia · Patella · Fibula (head)
3. MRI Planes — What Each Shows
| Plane | Structures Best Seen |
|---|---|
| Sagittal | ACL, PCL, menisci (anterior/posterior horns), quadriceps/patellar tendons |
| Coronal | MCL, LCL, meniscal body, articular cartilage width |
| Axial | Patellofemoral joint, trochlear groove, popliteal structures, iliotibial band |
Standard MRI Sequences
| Sequence | Tissue Contrast | Best For |
|---|---|---|
| T1-weighted | Fat = bright; fluid = dark | Anatomy, bone marrow fat |
| T2-weighted | Fat = bright; fluid = bright | Cartilage, cysts, edema |
| PD Fat-Sat | Fluid = bright; fat suppressed | Ligament/meniscal tears |
| STIR | Fluid/edema = very bright | Bone marrow edema, stress fractures |
| Gradient Echo | Cartilage = bright | Articular cartilage detail |
4. Key Anatomical Structures on MRI
4A. Cruciate Ligaments
| Ligament | Plane | Normal MRI Appearance | Function |
|---|---|---|---|
| ACL | Sagittal | Oblique low-signal band, parallel to roof of intercondylar notch | Prevents anterior tibial displacement |
| PCL | Sagittal | Curved low-signal band (hockey stick shape) | Prevents posterior tibial displacement |
ACL arises from posterior lateral femoral condyle → anterior tibial plateau (oblique course) PCL is shorter, stronger; arises from posterior tibial plateau → medial femoral condyle
4B. Collateral Ligaments
| Ligament | Plane | Function |
|---|---|---|
| MCL (Medial Collateral) | Coronal | Resists valgus stress; two layers (superficial & deep) |
| LCL (Lateral Collateral) | Coronal | Resists varus stress |
4C. Menisci
The menisci are C-shaped fibrocartilaginous structures visible in sagittal and coronal planes.
| Feature | Medial Meniscus | Lateral Meniscus |
|---|---|---|
| Shape | C-shaped (larger, open) | O-shaped (smaller, closed) |
| Mobility | Less mobile (attached to MCL) | More mobile |
| Tear rate | More commonly injured | Less commonly injured |
| MRI signal (normal) | Uniformly low signal (dark) on PD/T2 | Same |
Meniscal Tear Patterns (Bailey & Love's, p. 585):
- Circumferential (bucket-handle) — most common; causes locking
- Radial — extends inward from free edge
- Horizontal — splits meniscus into upper/lower leaves
- Flap — unstable fragment
- Degenerative — irregular, diffuse; seen in older patients
MRI tip: Abnormal signal reaching the articular surface = tear. Signal confined to meniscal substance = intrasubstance degeneration (Grade 1–2, not a true tear).
4D. Articular Cartilage
- Best sequences: PD fat-sat, 3D GRE, dGEMRIC
- Normal cartilage: smooth, uniform intermediate signal
- Femoral condyles, tibial plateaus, patella undersurface, trochlea all covered
Cartilage Grading (Modified Outerbridge):
| Grade | MRI Finding |
|---|---|
| 0 | Normal |
| I | Signal change, intact surface |
| II | Partial thickness defect < 50% |
| III | Partial thickness defect ≥ 50% |
| IV | Full thickness defect (bone exposed) |
4E. Extensor Mechanism
The extensor mechanism (Bailey & Love's, p. 511) consists of:
Quadriceps muscle
↓
Quadriceps tendon
↓
Patella
↓
Patellar tendon
↓
Tibial tuberosity
- Best visualized on sagittal images
- T2/PD: normal tendons are low signal (dark); tears show high signal disruption
4F. Bursae & Other Soft Tissues
| Structure | Location | Clinical Relevance |
|---|---|---|
| Prepatellar bursa | Anterior to patella | "Housemaid's knee" |
| Infrapatellar bursa | Below patellar tendon | "Clergyman's knee" |
| Baker's cyst | Posterior (semimembranosus-gastrocnemius) | Popliteal swelling, associated with intraarticular pathology |
| Iliotibial band | Lateral, axial plane | IT band syndrome |
5. Axial MRI Series — Slice-by-Slice Guide
The image below shows a 3×5 grid of sequential axial MRI slices (MR1200–MR1214) demonstrating:
- Distal femoral condyles (top slices)
- Patellofemoral trochlear groove (mid slices)
- Proximal tibia and joint space (lower slices)
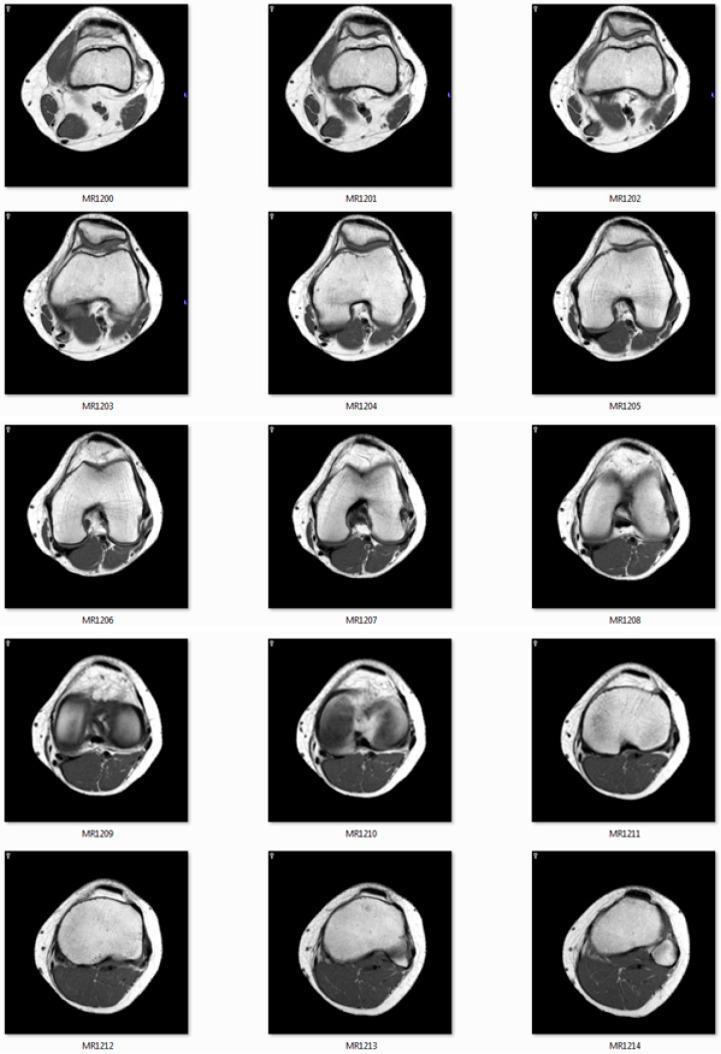
Key axial landmarks by level:
| Slice Level | Structures Seen |
|---|---|
| Suprapatellar | Quadriceps tendon, suprapatellar pouch, distal femoral shaft |
| Patellar | Patella, trochlear groove, medial/lateral retinaculae |
| Joint line | Femoral condyles, intercondylar notch, ACL/PCL origins |
| Proximal tibia | Tibial plateaus, IT band insertion, popliteal vessels |
6. Quick Reference: "Where is it on MRI?"
| Structure | Primary Plane | Secondary Plane |
|---|---|---|
| ACL | Sagittal | Coronal (oblique) |
| PCL | Sagittal | — |
| MCL | Coronal | — |
| LCL | Coronal | Axial |
| Medial meniscus | Sagittal (horns) | Coronal (body) |
| Lateral meniscus | Sagittal (horns) | Coronal (body) |
| Patellar tendon | Sagittal | Axial |
| Articular cartilage | Coronal | Sagittal |
| Baker's cyst | Axial | Sagittal |
| Bone marrow edema | STIR any plane | — |
7. Common Pathologies at a Glance
| Pathology | MRI Sequence | Finding |
|---|---|---|
| ACL tear | PD/T2 sagittal | Loss of fibrillar pattern, high signal, edema |
| PCL tear | PD/T2 sagittal | Discontinuity of posterior low-signal band |
| Meniscal tear | PD fat-sat sagittal | High signal touching articular surface |
| Cartilage loss | PD fat-sat coronal | Focal thinning/defect |
| Bone bruise | STIR | Ill-defined marrow high signal |
| Baker's cyst | T2 axial/sagittal | Posterior cystic structure between semimembranosus and medial gastrocnemius |
| Osteonecrosis | T1 + STIR | Low T1 subchondral lesion with perilesional edema |
8. Teaching Pearls for Students
💡 ACL rule of 45° — On a true sagittal MRI, the ACL should be parallel to the roof of the intercondylar notch (Blumensaat's line). If it is not, suspect a tear.
💡 "Dark on all sequences" — Normal ligaments and menisci are dark (low signal) on T1, T2, and PD. Any bright signal = pathology until proven otherwise.
💡 Meniscal "bow-tie" sign — On consecutive sagittal 5mm slices, you should see the meniscus as a bow-tie on ≥2 slices. Only 1 = bucket-handle tear.
💡 PCL integrity — The PCL is a reliable landmark; it is the last structure to tear. If the PCL is intact, the knee is likely not dislocated.
💡 Patellofemoral assessment — Always check patellar tilt and trochlear dysplasia on axial sequences.
References
- Harrison's Principles of Internal Medicine, 21st Edition — p. 10396
- Bailey and Love's Short Practice of Surgery, 28th Edition — pp. 511, 585
This guide covers the full spectrum of normal knee MRI anatomy, imaging planes, sequences, and common pathologies for student education. Use it alongside hands-on MRI workstation sessions for maximum learning.
This is a shared conversation. Sign in to Orris to start your own chat.