A presentation on the topic impedence Audiometery, BERA
Reading File
search_medical_text
impedance audiometry tympanometry acoustic reflex principles
search_medical_text
BERA brainstem evoked response audiometry electrophysiology hearing
search_medical_image
tympanogram types impedance audiometry
GradeResponse
GradeResponse
GradeResponse
search_medical_image
BERA waveform brainstem auditory evoked response
GradeResponse
Here is a comprehensive presentation on Impedance Audiometry and BERA (Brainstem Evoked Response Audiometry):
Impedance Audiometry & BERA
A Clinical Presentation
PART 1: IMPEDANCE AUDIOMETRY
1. Introduction
Impedance Audiometry (also called Immittance Audiometry) is an objective, non-invasive test of middle ear function. It does not require active participation from the patient, making it invaluable in children, uncooperative patients, and medico-legal cases.
- Impedance: Opposition to flow of sound energy
- Admittance (Immittance): Ease with which sound energy flows through the middle ear system (the reciprocal of impedance)
- Modern instruments measure acoustic immittance (admittance-based)
2. Components of the Impedance Audiometry Battery
| Test | What It Measures |
|---|---|
| Tympanometry | Middle ear pressure, compliance, and mobility |
| Acoustic Reflex (AR) | Integrity of reflex arc (CN VII, CN VIII, brainstem) |
| Acoustic Reflex Decay | Retrocochlear lesion detection |
| Static Acoustic Compliance | Absolute mobility of the tympanic membrane |
3. Instrumentation
The Electroacoustic Impedance Meter (Impedance Bridge) consists of:
- Probe tip — sealed in the external ear canal
- Probe tone generator — delivers a 226 Hz probe tone (85 dB SPL) in adults; 1000 Hz in infants < 6 months
- Air pressure pump — varies canal pressure from +200 to –400 daPa
- Microphone — detects reflected sound
- Manometer — measures ear canal air pressure
- Bridge meter — measures and displays compliance
4. Tympanometry
Tympanometry measures the compliance (mobility) of the tympanic membrane and middle ear as a function of varied air pressure in the sealed ear canal.
"Tympanometry measures the impedance of the middle ear to sound and is useful in diagnosis of middle-ear effusions. A tympanogram is the graphic representation of change in impedance or compliance as the pressure in the ear canal is changed." — Harrison's Principles of Internal Medicine, 21st Ed. (p. 1039)
How it works:
- Ear canal is sealed with probe tip
- Air pressure is varied from +200 to –400 daPa
- Compliance changes are plotted as a tympanogram
5. Tympanogram Types (Jerger's Classification)
| Type | Shape | Peak Pressure | Compliance | Clinical Significance |
|---|---|---|---|---|
| Type A | Normal peak at 0 daPa | Normal (0 ± 50 daPa) | Normal (0.3–1.6 ml) | Normal middle ear |
| Type As | Shallow/reduced peak | Normal | Low (<0.3 ml) | Otosclerosis, tympanosclerosis, fixed ossicular chain |
| Type Ad | Deep/high peak | Normal | High (>1.6 ml) | Ossicular discontinuity, thin/flaccid TM |
| Type B | Flat, no peak | Absent | Minimal | Middle ear effusion, perforated TM, wax impaction |
| Type C | Peak shifted negative | < –100 daPa | Normal or low | Eustachian tube dysfunction, early OME |
"Compliance that does not change with change in pressure suggests middle-ear effusion (Type B). With negative pressure in the middle ear, as with Eustachian tube obstruction, the point of maximal compliance occurs with negative pressure (Type C)." — Harrison's (p. 1039)
6. Acoustic Reflex
The Acoustic Stapedial Reflex (ASR) is a bilateral contraction of the stapedius muscle in response to loud sound (70–100 dB above threshold).
Reflex Arc:
Loud Sound → Cochlea → CN VIII → Cochlear Nucleus
→ Superior Olivary Complex → Facial Nerve Nucleus (CN VII)
→ Stapedius Muscle contraction (bilateral)
Types of Acoustic Reflex Testing:
| Type | Probe Ear | Stimulus Ear | Tests |
|---|---|---|---|
| Ipsilateral (uncrossed) | Same ear | Same ear | CN VIII, lower brainstem, CN VII (same side) |
| Contralateral (crossed) | Opposite ear | Stimulus ear | CN VIII, entire brainstem pathway, CN VII (probe side) |
Acoustic Reflex Threshold (ART):
- Normal: 70–100 dB HL above pure tone threshold
- Absent reflex → suggests conductive loss, severe SNHL, CN VII palsy, or brainstem lesion
- Elevated reflex → seen in moderate SNHL
Clinical Significance:
| Finding | Possible Cause |
|---|---|
| Absent ipsilateral + contralateral (one ear) | CN VIII lesion (that ear) |
| Absent contralateral only | Brainstem lesion (crossed pathway) |
| Absent all reflexes with flat tympanogram | Middle ear pathology |
| Present reflex at low SL (<60 dB) | Recruitment (cochlear lesion) |
| Absent reflex at normal hearing levels | Retrocochlear (CN VIII) lesion |
7. Acoustic Reflex Decay (ARD)
- Stimulus: Sustained tone at 10 dB above ART for 10 seconds
- Positive decay (>50% amplitude reduction in 5 seconds) = retrocochlear lesion (acoustic neuroma, CN VIII lesion)
- Tested at 500 Hz and 1000 Hz
- Normal: reflex sustained for full 10 seconds
8. Static Acoustic Compliance
- Measured in milliliters (ml) or cm³
- Normal: 0.3–1.6 ml
- Reduced (<0.3 ml): Otosclerosis, middle ear effusion
- Increased (>1.6 ml): Ossicular discontinuity, flaccid TM
9. Clinical Applications of Impedance Audiometry
| Condition | Tympanogram | Acoustic Reflex |
|---|---|---|
| Normal | Type A | Present, normal |
| Otitis media with effusion (OME/Glue ear) | Type B | Absent |
| Eustachian tube dysfunction | Type C | Present or absent |
| Otosclerosis | Type As | Absent (ipsi) |
| Ossicular discontinuity | Type Ad | Absent |
| Sensorineural hearing loss (cochlear) | Type A | Elevated threshold / absent |
| Acoustic neuroma (CN VIII) | Type A | Absent + reflex decay positive |
| CN VII palsy | Type A | Absent (ipsilateral) |
| TM perforation | Type B (large volume) | Absent |
PART 2: BERA (Brainstem Evoked Response Audiometry)
1. Introduction
BERA (Brainstem Evoked Response Audiometry), also known as:
- ABR — Auditory Brainstem Response
- BAER — Brainstem Auditory Evoked Response
- BAEP — Brainstem Auditory Evoked Potential
It is an objective, electrophysiological test that measures electrical activity generated along the auditory pathway from the cochlea to the midbrain in response to sound stimuli.
"Brainstem auditory-evoked responses (BAERs)... are useful in differentiating the site of sensorineural hearing loss. In response to sound, five distinct electrical potentials arising from different stations along the peripheral and central auditory pathway can be identified using computer averaging from scalp surface electrodes." — Harrison's Principles of Internal Medicine, 21st Ed. (p. 1041)
2. Neural Generators of BERA Waves
Five major waves (Jewett waves) are identified within the first 10 milliseconds after stimulus:
| Wave | Generator (Neural Origin) | Approximate Latency |
|---|---|---|
| Wave I | Distal CN VIII (cochlear nerve) | ~1.5 ms |
| Wave II | Proximal CN VIII / Cochlear nucleus | ~2.5 ms |
| Wave III | Superior olivary complex | ~3.5 ms |
| Wave IV | Lateral lemniscus | ~4.5 ms |
| Wave V | Inferior colliculus (midbrain) | ~5.5 ms |
Waves I, III, and V are the most consistent and clinically important.
3. BERA Waveform — Clinical Example
The image below shows a real BERA recording: the right ear shows an absent/flat response (consistent with unilateral hearing loss or CN VIII dysfunction), while the left ear demonstrates a normal waveform with Waves I (1.33 ms), III (3.60 ms), and V (5.60 ms) clearly identified, and normal inter-peak intervals:
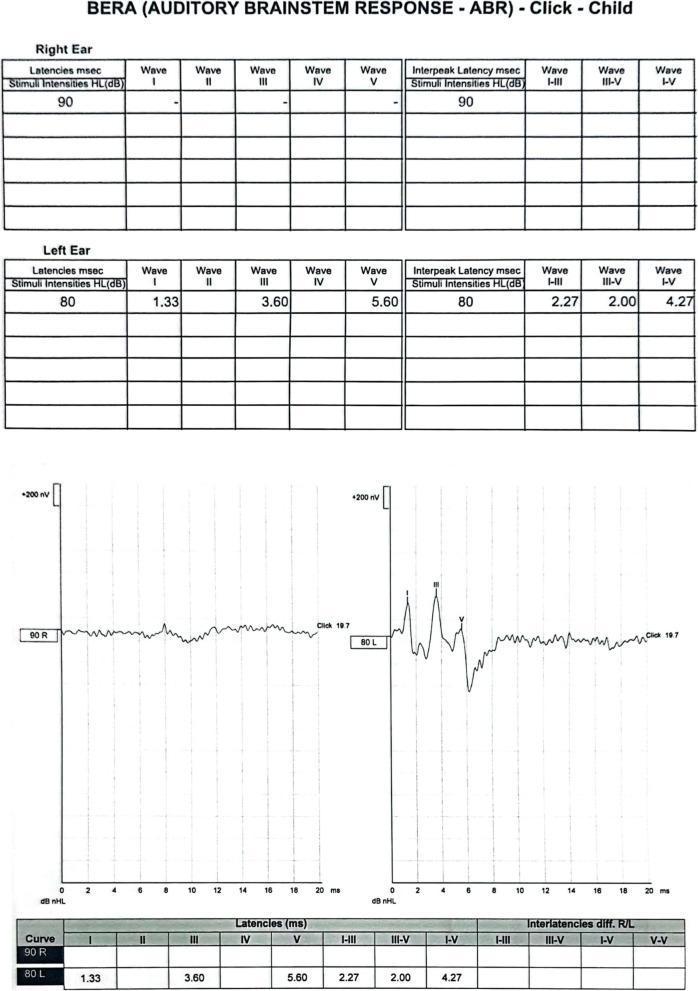
Right ear: flat/absent response. Left ear: normal waves I, III, V with normal latencies. Clinically consistent with right-sided auditory nerve dysfunction or profound unilateral hearing loss.
4. Instrumentation and Procedure
Equipment: Evoked potential recording system with:
- Surface electrodes (Ag-AgCl)
- Signal averager (computer)
- Earphones (insert or standard)
Electrode Placement:
- Active (non-inverting): Vertex (Cz) or forehead
- Reference (inverting): Ipsilateral mastoid/earlobe
- Ground: Contralateral mastoid/forehead
Stimulus:
- Click stimulus (broadband, 0.1 ms duration) — most commonly used
- Tone pip/burst — frequency-specific testing
- Rate: 10–90 clicks/second (typically 11.1/sec)
- Intensity: 60–90 dB nHL for threshold search; 80–90 dB for neurodiagnosis
- Polarity: Rarefaction, condensation, or alternating
Averaging:
- 1000–2000 sweeps averaged to extract the tiny neural signal (0.1–1 µV) from background noise
5. BERA Parameters Measured
| Parameter | Normal Value | Clinical Significance |
|---|---|---|
| Absolute latency Wave I | ~1.5 ms | Peripheral (cochlear/CN VIII) |
| Absolute latency Wave III | ~3.5 ms | Brainstem (lower) |
| Absolute latency Wave V | ~5.5–5.7 ms | Brainstem (upper/midbrain) |
| Inter-peak Interval I–III | ~2.0 ms | Peripheral to lower brainstem |
| Inter-peak Interval III–V | ~2.0 ms | Lower to upper brainstem |
| Inter-peak Interval I–V | ~4.0 ms | Total brainstem conduction |
| Interaural latency difference (ILD) Wave V | < 0.4 ms | Asymmetric lesion detection |
| Threshold estimation | 10–20 dB above behavioral | Hearing threshold |
6. Interpretation of BERA
A. Conductive Hearing Loss
- All waves present but with increased absolute latencies (shift to the right)
- Inter-peak intervals normal (I–III, III–V, I–V unchanged)
- Wave I most affected
B. Cochlear (Sensory) Hearing Loss
- Absent or poorly formed Wave I at low intensities
- Remaining inter-peak intervals normal
- Threshold elevated
C. Retrocochlear (CN VIII / Acoustic Neuroma)
- Prolonged I–III inter-peak interval (> 2.3 ms)
- Absent waves beyond Wave I, or wave V absent
- Interaural latency difference Wave V > 0.4 ms
- Positive acoustic reflex decay on impedance audiometry
D. Brainstem Pathology (e.g., MS, tumor)
- Prolonged III–V interval (> 2.3 ms)
- Abnormal waveform morphology
- Waves I and III present, but Wave V delayed/absent
7. Clinical Applications of BERA
| Indication | Use |
|---|---|
| Neonatal hearing screening | Objective threshold in newborns (UNHS programs) |
| Infants/uncooperative patients | Cannot do behavioral audiometry |
| Acoustic neuroma / VS detection | Retrocochlear site of lesion |
| Multiple Sclerosis | Detects subclinical brainstem demyelination |
| Intraoperative monitoring | CN VIII and brainstem during skull base surgery |
| Brain death determination | Absent all BERA waves (except Wave I) |
| Auditory neuropathy spectrum disorder (ANSD) | Absent/abnormal ABR with present OAEs |
| Medico-legal | Objective hearing threshold estimation |
| Comatose/unconscious patients | Prognostication after TBI or hypoxia |
8. Factors Affecting BERA
| Factor | Effect |
|---|---|
| Age | Latencies shorten with maturation (adult values by ~18 months) |
| Gender | Females have shorter latencies and larger amplitudes |
| Body temperature | Hypothermia prolongs latencies (~0.2 ms/°C) |
| Sedation/anesthesia | Minimal effect (advantage of BERA) |
| Hearing loss | Elevated thresholds, prolonged latencies |
| Stimulus intensity | Higher intensity → shorter latencies, larger amplitudes |
9. Advantages and Limitations
| BERA | Impedance Audiometry | |
|---|---|---|
| Objective | Yes | Yes |
| No patient cooperation needed | Yes | Yes |
| Tests middle ear | No | Yes |
| Tests cochlea | Threshold estimation | No |
| Tests CN VIII / brainstem | Yes | Partially (reflex arc) |
| Frequency specific | Limited (tone-burst) | No |
| Sedation sometimes needed | Yes (infants) | No |
| Site of lesion | Yes | Partially |
PART 3: COMBINED INTERPRETATION
| Clinical Scenario | Impedance | BERA |
|---|---|---|
| Otitis Media with Effusion | Type B, absent reflexes | Normal (or elevated threshold) |
| Otosclerosis | Type As, absent reflexes | Normal inter-peak intervals, elevated threshold |
| Acoustic Neuroma (Vestibular Schwannoma) | Type A, absent/decaying reflex | Prolonged I–III, large ILD Wave V |
| Cochlear SNHL | Type A, elevated/absent reflex | Elevated threshold, normal IPIs |
| Auditory Neuropathy (ANSD) | Type A, absent reflex | Absent/abnormal ABR |
| Brainstem lesion (MS) | Type A, abnormal crossed reflex | Prolonged III–V interval |
| Normal | Type A, reflexes present at 70–100 dB | Normal latencies, clear waves I–V |
Summary
- Impedance Audiometry evaluates the middle ear (tympanometry), stapedial reflex arc (CN VII, CN VIII, brainstem), and helps localize conductive vs. sensorineural pathology.
- BERA evaluates the entire auditory pathway from cochlea to midbrain — it is the gold standard for objective hearing threshold estimation and retrocochlear lesion detection.
- Together, they form a powerful objective audiological test battery essential in ENT, Neurology, Pediatrics, and Audiology practice.
Sources: Harrison's Principles of Internal Medicine, 21st Edition (pp. 1039, 1041); Clinical Audiology principles.



