
Extraction tips
Reading File
search_medical_text
tooth extraction techniques tips impacted tooth surgical
search_medical_image
impacted tooth dental X-ray extraction
GradeResponse
GradeResponse
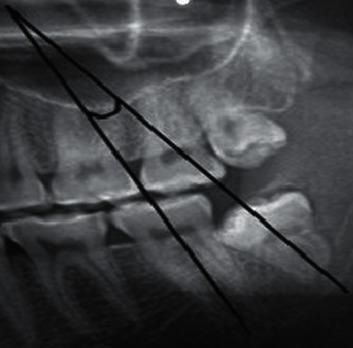
Looking at your X-ray, it appears to show an impacted mandibular third molar (lower wisdom tooth) with mesioangular or horizontal impaction — the tooth is tilted against the adjacent second molar.
Extraction Tips for an Impacted Lower Molar
Pre-op Assessment
- Classify the impaction using Winter's classification (mesioangular, horizontal, vertical, distoangular). Mesioangular is the most common and generally easier; horizontal is the most difficult.
- Assess root morphology — fused/conical roots are easier; divergent or hooked roots increase difficulty.
- Note proximity to the inferior alveolar nerve (IAN) — if the roots appear to overlap the mandibular canal on 2D X-ray, consider a CBCT before proceeding.
- Pell & Gregory classification assesses depth and ramus relationship — deeper Class C and ramus-adjacent Class III cases are more surgically demanding.
Surgical Technique
-
Incision & Flap Design
- Envelope flap: sulcular incision along the second molar extending distally with a releasing incision anteriorly.
- Adequate mucoperiosteal reflection is critical — don't cut corners here.
-
Bone Removal
- Use a surgical handpiece with copious saline irrigation.
- Remove bone on the buccal and distal aspects to expose the CEJ and give instrument purchase.
- Avoid excessive lingual bone removal (lingual nerve risk).
-
Tooth Sectioning (often necessary for impacted teeth)
- Section the crown from the root(s) for mesioangular/horizontal impactions — removes the "block" against the second molar.
- For multi-rooted teeth with divergent roots, section roots individually.
-
Delivery
- Use luxators first (fine, sharp blade) to sever the PDL before elevators.
- Apply elevator (Warwick James, Cryer) with controlled force using bone as fulcrum — never the adjacent tooth.
- Wheel and axle motion rather than levering.
-
Socket Management
- Debride the follicle, irrigate with saline.
- Smooth sharp bony edges with a bone file or bur.
- Primary closure vs. secondary healing — both acceptable, but primary closure reduces dry socket risk.
Key Pearls
| Concern | Tip |
|---|---|
| Dry socket (alveolar osteitis) | Most common complication (~5–30% for lower wisdom teeth). Avoid excessive irrigation post-op, no smoking, no straws |
| IAN injury | If roots are intimate with the canal, consider coronectomy (intentional root retention) as an alternative |
| Lingual nerve | Keep retractor firmly on bone; avoid blind cutting lingually |
| Second molar damage | Tooth sectioning reduces lateral force on the second molar |
| Difficult access | Adequate mouth opening is key — consider LA nerve block technique carefully (IANB + long buccal + lingual nerve block) |
Post-op Instructions for Patient
- Bite on gauze for 30–45 min; replace if soaking.
- Soft diet, no smoking, no straws for 72 hours minimum.
- NSAIDs (ibuprofen) ± paracetamol; prescribe antibiotics only if infection present pre-op or immunocompromised patient.
- Return if pain worsens after day 3 (classic dry socket presentation).
If you can share the full X-ray or CBCT with better angulation, a more specific extraction plan can be outlined.
This is a shared conversation. Sign in to Orris to start your own chat.