Perichondritis of Ear in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
perichondritis of ear etiology pathology clinical features diagnosis management
search_medical_text
perichondritis auricle treatment antibiotics surgery Pseudomonas complications
search_medical_image
perichondritis ear auricle anatomy diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
perichondritis pinna auricle ENT Scott Brown Cummings Dhingra management
search_medical_image
auricle anatomy cartilage helix antihelix concha external ear
GradeResponse
Now I have sufficient material. Let me compose a comprehensive, exam-ready 50-mark answer on Perichondritis of the Ear.
PERICHONDRITIS OF THE EAR
A Comprehensive Essay for 50 Marks | RGUHS ENT Examination
1. INTRODUCTION & DEFINITION
Perichondritis is an acute or chronic inflammation of the perichondrium — the fibrous connective tissue membrane that covers the auricular cartilage. It can rapidly extend to involve the underlying cartilage itself, at which point it is termed chondritis or suppurative perichondritis.
The auricle (pinna) is uniquely vulnerable because its cartilage is avascular and derives its nutrition entirely from the perichondrium. Any disruption of this perichondrial blood supply precipitates cartilage necrosis and can lead to the dreaded deformity known as "cauliflower ear" (wrestler's ear / boxer's ear).
"The cartilage of the pinna depends entirely on the perichondrium for its blood supply; any condition that separates the perichondrium from the cartilage leads to avascular necrosis." — Dhingra's Diseases of Ear, Nose and Throat
2. SURGICAL ANATOMY OF THE AURICLE
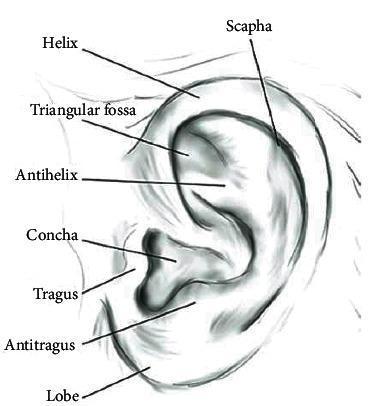
| Structure | Description |
|---|---|
| Helix | Outermost curved rim of the pinna |
| Antihelix | Y-shaped inner ridge parallel to helix |
| Scapha | Groove between helix and antihelix |
| Triangular fossa | Space between the two crura of antihelix |
| Concha | Deep bowl leading to external auditory canal |
| Tragus | Anterior cartilaginous projection |
| Antitragus | Projection opposite the tragus |
| Lobule | Inferior fleshy part — NO cartilage |
Key Anatomical Points (Clinically Relevant):
- The auricular cartilage is elastic fibrocartilage (type II collagen)
- Blood supply to perichondrium: superficial temporal artery (anterior) + posterior auricular artery (posterior)
- The perichondrium contains all the vascular, lymphatic, and nerve supply to the cartilage
- Lobule is always spared in perichondritis (pathognomonic finding) — it has no cartilage
3. ETIOLOGY
3.1 Predisposing Causes (RGUHS Classification)
┌────────────────────────────────────────────────────────────────┐
│ CAUSES OF PERICHONDRITIS │
├────────────────────────────────────────────────────────────────┤
│ TRAUMATIC │ IATROGENIC │ SYSTEMIC │
│ • Blunt trauma │ • Ear piercing │ • Diabetes mellitus│
│ • Lacerations │ (high helix) │ • Relapsing │
│ • Burns │ • Post-surgical │ polychondritis │
│ • Frostbite │ (mastoidectomy, │ • Immunocompromised│
│ • Insect bites │ incision/drainage)│ • SLE │
│ • Otitis externa │ • Acupuncture │ │
│ (furunculosis) │ • Hematoma │ │
│ │ (untreated) │ │
└────────────────────────────────────────────────────────────────┘
3.2 Most Common Causes by Textbook Reference:
| Source | Cited Common Cause |
|---|---|
| Dhingra | Trauma, infected wounds, furuncle of EAC |
| Scott-Brown's Otorhinolaryngology | High ear piercing (helix), post-traumatic hematoma |
| Cummings Otolaryngology | Ear piercing (cartilaginous helix), burns, trauma |
| Hazarika ENT | Trauma, infection of pinna, surgical incisions |
| Zakir Hussain's ENT | Hematoma auris, furunculosis, trauma |
| Stell & Maran's | Post-operative, burns, frostbite |
High cartilage piercing (through the helix/antihelix rather than the lobule) has emerged as the most common cause in young adults in recent decades — cited in Cummings (6th/7th Ed.) and corroborated by multiple recent studies.
4. MICROBIOLOGY / CAUSATIVE ORGANISMS
| Organism | Frequency | Notes |
|---|---|---|
| Pseudomonas aeruginosa | Most common (60-70%) | Gram-negative; resistant to many antibiotics; hallmark organism |
| Staphylococcus aureus | Second most common | Including MRSA in hospital settings |
| Streptococcus pyogenes | Less common | Post-traumatic |
| Proteus mirabilis | Occasional | Gram-negative |
| Escherichia coli | Rare | Immunocompromised |
| Klebsiella spp. | Rare | |
| Polymicrobial | Burn cases | Mixed flora |
Pseudomonas aeruginosa is the key pathogen — cited across all major ENT texts (Cummings, Dhingra, Scott-Brown). Its affinity for cartilage and ability to produce biofilms, elastase, exotoxin A, and pyocyanin makes eradication difficult and is the reason fluoroquinolones are preferred.
5. PATHOLOGY & PATHOGENESIS
FLOWCHART: PATHOGENESIS OF PERICHONDRITIS
══════════════════════════════════════════
Predisposing Factor
(Trauma / Piercing / Surgery / Hematoma / Infection)
│
▼
Break in skin or disruption of perichondrium
│
▼
Entry of organisms (predominantly Pseudomonas aeruginosa)
│
▼
Infection of perichondrium → Acute inflammation
│
▼
Pus accumulates between perichondrium and cartilage
(Sub-perichondrial abscess formation)
│
▼
Perichondrium stripped away from cartilage
│
▼
Avascular necrosis of cartilage
(Cartilage = avascular; depends entirely on perichondrium for nutrition)
│
▼
Fibrous replacement and irregular calcification
│
▼
CAULIFLOWER EAR (Acquired deformity)
Histopathology (Stell & Maran reference):
- Acute phase: Edema, hyperemia, neutrophilic infiltration of perichondrium
- Sub-acute phase: Sub-perichondrial abscess; early chondrocyte necrosis
- Chronic phase: Fibroblastic proliferation; dystrophic calcification; cartilage dissolution and replacement with fibrous tissue
6. CLINICAL FEATURES
6.1 Symptoms
| Symptom | Details |
|---|---|
| Pain | Severe, throbbing; disproportionate to visible signs; worsens at night |
| Fever | Low to high grade; systemic features in severe cases |
| Swelling | Progressive; starts at one part of pinna and spreads |
| Redness | Intense erythema of the pinna |
| Discharge | Purulent discharge if abscess points and ruptures |
| Tenderness | Exquisite tenderness on palpation of pinna |
6.2 Signs (Clinical Examination)

CLASSIC SIGNS ON EXAMINATION:
════════════════════════════════
✓ Pinna: Hot, red, swollen, tender
✓ Lobule: SPARED (pathognomonic — no cartilage in lobule)
✓ Pitting edema over auricle (early)
✓ Fluctuation (late — indicates abscess formation)
✓ Obliteration of normal auricular landmarks
✓ Regional lymphadenopathy (pre-auricular / post-auricular)
✓ Possible seropurulent discharge
✗ EAC and tympanic membrane: usually NORMAL
6.3 Stages of Perichondritis (Dhingra Classification)
| Stage | Features |
|---|---|
| Stage I | Edema + erythema; no abscess; landmarks preserved |
| Stage II | Abscess formation; landmarks obliterated; fluctuation present |
| Stage III | Cartilage necrosis; deformity beginning; cauliflower formation |
7. DIAGNOSIS
7.1 Clinical Diagnosis
The diagnosis is primarily clinical based on the characteristic triad:
- Hot, red, swollen, tender pinna
- Lobule SPARED
- History of predisposing factor (trauma, piercing, surgery)
7.2 Investigations
| Investigation | Finding / Purpose |
|---|---|
| CBC | Leukocytosis (neutrophilia); elevated TLC |
| ESR, CRP | Elevated; monitor treatment response |
| Pus swab / culture & sensitivity | Identifies organism (most often Pseudomonas); guides antibiotic therapy |
| Blood culture | If systemic sepsis suspected |
| Blood glucose | Rule out diabetes mellitus |
| CT scan pinna | Assesses extent of cartilage destruction; rarely needed |
| MRI | Soft tissue involvement; chronic/relapsing cases |
| Biopsy | Only in atypical cases (rule out relapsing polychondritis, malignancy) |
7.3 Diagnostic Criteria for Relapsing Polychondritis (McAdam et al., 1976 — Harrison's, p. 10301)
Relevant when perichondritis is bilateral, recurrent, or associated with systemic features. Requires 3 of 6 criteria including auricular chondritis, inflammatory arthritis, nasal chondritis, ocular inflammation, tracheolaryngeal chondritis, or audiovestibular damage.
8. DIFFERENTIAL DIAGNOSIS
┌──────────────────────────────────────────────────────────────┐
│ DIFFERENTIAL DIAGNOSIS │
├─────────────────────────────┬────────────────────────────────┤
│ Condition │ Distinguishing Features │
├─────────────────────────────┼────────────────────────────────┤
│ Cellulitis of pinna │ Lobule INVOLVED; no abscess │
│ Hematoma auris │ Fluctuant; no fever; follows │
│ │ blunt trauma; no erythema │
│ Erysipelas │ Bright red; sharp margins; │
│ │ streptococcal; lobule involved │
│ Relapsing polychondritis │ Bilateral; systemic features; │
│ │ nasal/tracheal involvement │
│ Otitis externa │ EAC involved; pain on │
│ │ tragus pressure │
│ Sebaceous cyst (infected) │ Punctum visible; mobile; │
│ │ cheesy discharge │
│ Gouty tophus │ Chalky deposits; hyperuricemia │
│ Malignant otitis externa │ Pseudomonas; elderly diabetic; │
│ │ granulation in EAC floor │
└─────────────────────────────┴────────────────────────────────┘
9. TREATMENT
FLOWCHART: MANAGEMENT OF PERICHONDRITIS
Patient with Hot, Red, Swollen Pinna + Lobule Spared
│
▼
Assess Stage of Disease
┌──────────┴──────────┐
│ │
No Abscess Abscess Present
(Stage I) (Stage II & III)
│ │
▼ ▼
MEDICAL SURGICAL +
MANAGEMENT MEDICAL
│ │
▼ ▼
IV/Oral Antibiotics Incision & Drainage
(Anti-pseudomonal) OR Through-and-through
│ drainage with stent
▼ │
Local care ▼
Pain management Antibiotics +
Diabetes control Bolster dressing
│ │
└──────────┬──────────┘
▼
Monitor response at 48-72 hours
│
┌──────────┴──────────┐
│ │
Improving Not improving
│ │
▼ ▼
Continue Change antibiotics
treatment (per C&S)
4-6 weeks Repeat drainage
Consider debridement
│
▼
Cartilage necrosis?
┌──────┴──────┐
│ │
No Yes
│ │
Heal Debridement of
necrotic cartilage
+ reconstruction
(if needed)
9.1 Medical Treatment
A. Antibiotics (DRUG OF CHOICE)
| Drug | Dose | Route | Rationale |
|---|---|---|---|
| Ciprofloxacin (First choice) | 500-750 mg BD | Oral / IV | Anti-pseudomonal fluoroquinolone; excellent cartilage penetration |
| Piperacillin-tazobactam | 4.5 g TDS | IV | Severe/resistant cases |
| Ceftazidime | 1-2 g TDS | IV | Third-generation cephalosporin; anti-pseudomonal |
| Cefepime | 2 g BD | IV | 4th-generation cephalosporin |
| Imipenem | 500 mg QID | IV | Resistant Pseudomonas; last resort |
| Amikacin | 15 mg/kg/day | IV | Gram-negative synergy |
| Cloxacillin / Flucloxacillin | 500 mg QID | Oral | If Staphylococcal infection suspected |
| Vancomycin | 15-20 mg/kg BD | IV | MRSA |
Duration: Minimum 4-6 weeks of antibiotic therapy is recommended (Cummings, Scott-Brown) to prevent relapse and cartilage necrosis.
Ciprofloxacin is the drug of choice — highlighted across Dhingra, Hazarika, Cummings, and Scott-Brown because of its:
- Anti-pseudomonal activity
- Excellent tissue and cartilage penetration
- Oral bioavailability comparable to IV (enabling outpatient completion)
B. Supportive Treatment
- NSAIDs / Analgesics: Ibuprofen, Diclofenac for pain and inflammation
- Antipyretics: Paracetamol
- Local care: Gentle cleaning; avoid pressure on ear; ear in dependent position
- Diabetes control: Essential — hyperglycemia impairs neutrophil function
- Topical antibiotics (mild cases): Ciprofloxacin ear drops or fusidic acid ointment
9.2 Surgical Treatment
Indications:
- Abscess formation (Stage II / III)
- Failure to respond to medical therapy within 48-72 hours
- Cartilage necrosis
Procedures:
A. Aspiration (Early Abscess)
- Fine needle aspiration of loculated pus
- Simultaneous culture and sensitivity
- Repeat if needed
B. Incision and Drainage (Classical Method)
Procedure Steps:
1. Local anaesthesia (EMLA or LA infiltration)
2. Incision along the antihelix (to hide scar in natural fold)
OR elliptical excision of skin flap
3. Complete evacuation of pus
4. Thorough debridement of necrotic perichondrium
5. Irrigation with povidone-iodine / NS
6. Placement of corrugated rubber drain
7. Pressure dressing (bolster/dental roll dressing)
to obliterate dead space and prevent re-accumulation
8. Wound left open / loosely closed
9. Daily dressings; drain removed at 48-72 hrs
C. Through-and-Through Drainage with Stent/Button Sutures
- Preferred by Scott-Brown and Cummings for established abscess
- Multiple parallel incisions on anterior and posterior surfaces
- Polythene/rubber tubes threaded through to act as drains
- Prevents recollection; keeps cartilage apposed to skin
- Stents removed at 5-7 days
D. Debridement of Necrotic Cartilage
- Indicated when cartilage is frankly necrotic (gray/black, non-bleeding)
- Conservative debridement — preserve as much viable cartilage as possible
- Leaves a template for future reconstruction
E. Auricular Reconstruction (Late)
- For severe cauliflower ear deformity
- Techniques: Costal cartilage graft (Nagata technique), Silastic/Medpor implants
- Usually deferred 6-12 months after active infection resolves
9.3 Pressure Dressing (Bolster Dressing) — Hazarika Emphasis
A critical adjunct in management:
- Purpose: Obliterate dead space, maintain cartilage-perichondrium apposition, prevent hematoma re-accumulation
- Method: Cotton wool dental rolls / plaster of Paris molds contoured to pinna anatomy, secured with through-and-through mattress sutures
- Change: Every 24-48 hours
- Must conform to all contours of pinna (especially scapha, concha, triangular fossa)
10. COMPLICATIONS
┌───────────────────────────────────────────────────────────┐
│ COMPLICATIONS │
├──────────────────────────────────────────────────────────┤
│ LOCAL COMPLICATIONS │
│ • Chondritis (cartilage infection) │
│ • Cartilage necrosis │
│ • Cauliflower ear (permanent deformity) │
│ • Fistula formation │
│ • Scar contracture │
│ │
│ REGIONAL COMPLICATIONS │
│ • Spread to EAC (otitis externa) │
│ • Parotid region cellulitis │
│ • Lymphadenopathy / suppurative lymphadenitis │
│ • Mastoid involvement (rare) │
│ │
│ SYSTEMIC COMPLICATIONS │
│ • Septicemia │
│ • Meningitis (extremely rare) │
│ • Endocarditis (rare — bacteremia) │
│ │
│ TREATMENT-RELATED │
│ • Antibiotic resistance (especially Pseudomonas) │
│ • Drug toxicity (aminoglycosides — nephro/ototoxicity) │
└───────────────────────────────────────────────────────────┘
11. SPECIAL CLINICAL ENTITIES
11.1 Perichondritis Following High Ear Piercing
- Most common cause in young adults today (replacing trauma)
- The helix and antihelix are cartilaginous — piercing here carries high risk
- Pseudomonas aeruginosa is predominant (from contaminated water/equipment)
- Management: Remove piercing; ciprofloxacin-based therapy; drainage if needed
11.2 Hematoma Auris → Perichondritis
Blunt Trauma
│
▼
Hematoma Auris (blood between perichondrium and cartilage)
│
▼ (if untreated)
│
├──────────────────────────────────────────┐
│ │
▼ ▼
Organized Hematoma Secondary infection
(Cauliflower ear) │
▼
Perichondritis
Prevention: Prompt aspiration of hematoma within 24-48 hours + pressure dressing
11.3 Relapsing Polychondritis (Non-infective)
(Harrison's, p. 10301 — McAdam criteria)
- Autoimmune; Type II collagen antibodies
- Bilateral auricular involvement + nasal, tracheobronchial, ocular, articular
- Treatment: Corticosteroids (Prednisolone 1 mg/kg/day) + Dapsone / Methotrexate
- Distinguished from infective perichondritis by: bilateral, recurrent, systemic features, negative cultures
11.4 Malignant (Necrotizing) Otitis Externa vs. Perichondritis
| Feature | Perichondritis | Malignant OE |
|---|---|---|
| Age | Any | Elderly diabetic |
| Location | Pinna | EAC + skull base |
| Key sign | Lobule spared | Granulation at EAC floor |
| CN involvement | Rare | CN VII, IX, X, XI, XII |
| CT | Perichondral | Temporal bone erosion |
| Treatment | Ciprofloxacin ± drainage | Prolonged anti-pseudomonal IV |
12. RECENT ADVANCES (RGUHS Focus)
12.1 Newer Antimicrobial Strategies
| Advance | Details |
|---|---|
| Anti-biofilm agents | N-acetylcysteine, gallium compounds disrupt Pseudomonas biofilm |
| Bacteriophage therapy | Experimental; phage cocktails targeting Pseudomonas; promising in MDR cases |
| Newer fluoroquinolones | Levofloxacin, Delafloxacin — broader spectrum, anti-MRSA activity |
| Ceftolozane-tazobactam | Active against MDR Pseudomonas; emerging role |
| Inhaled colistin | For MDR/XDR Pseudomonas in combination regimens |
12.2 Vacuum-Assisted Closure (VAC) Therapy
- Negative pressure wound therapy (NPWT) applied to post-debridement wound
- Promotes granulation tissue; reduces bacterial load
- Used in recalcitrant/post-debridement cases (recent case series, 2018-2022)
12.3 Antibiotic-Loaded Biomaterials
- Ciprofloxacin-eluting nanoparticles and hydroxyapatite scaffolds — experimental
- Allow local high-concentration delivery to avascular cartilage
12.4 Reconstructive Advances in Post-Perichondritis Deformity
- 3D-printed auricular scaffolds: Customized porous polyethylene implants (Medpor) or bioresorbable scaffolds seeded with chondrocytes
- Tissue engineering: Autologous chondrocyte expansion on biodegradable scaffolds — promising in pediatric reconstruction (Yanaga et al., 2009; follow-up publications 2018-2023)
- Total auricular reconstruction: Nagata's two-stage costal cartilage framework remains gold standard but newer bionic ear approaches are under investigation
12.5 Imaging Advances
- High-resolution ultrasound (HRUS): Can delineate sub-perichondrial fluid collection, cartilage thickness, and guide aspiration
- MRI with gadolinium: Best modality for assessing soft-tissue extent and cartilage viability; differentiates abscess from cellulitis without radiation
12.6 Genetic/Immune Studies in Relapsing Polychondritis
- HLA-DR4 association identified
- Anti-matrilin-1, anti-type II collagen antibodies as serological markers
- Biologics (Tocilizumab — anti-IL-6; Adalimumab — anti-TNF) showing promise in refractory relapsing polychondritis (recent case reports and small RCTs)
12.7 Antimicrobial Stewardship
- IDSA/ESCMID guidelines emphasize culture-directed therapy and discouraging empirical broad-spectrum use
- Fluoroquinolone resistance in Pseudomonas is rising globally (up to 30% in some centers) — reinforces the need for early cultures
13. PREVENTION
| Measure | Details |
|---|---|
| Ear piercing | Avoid cartilaginous piercings; use sterile equipment; aftercare with antiseptic |
| Hematoma drainage | Prompt aspiration + pressure dressing within 24-48 hours |
| Post-surgical care | Aseptic technique; avoiding pressure necrosis on pinna post-mastoidectomy |
| Diabetes control | HbA1c < 7%; reduces infection susceptibility |
| Acupuncture | Use sterile disposable needles only |
| Contact sports | Protective ear gear (head guards) to prevent hematoma |
14. PROGNOSIS
| Factor | Impact |
|---|---|
| Early diagnosis & treatment | Excellent; full recovery without deformity |
| Delayed treatment | Poor; cartilage necrosis → cauliflower ear |
| Pseudomonas infection | Worse prognosis; more aggressive course |
| Immunocompromised host | Higher risk of complications; prolonged treatment needed |
| Relapsing polychondritis | Variable; systemic complications determine outcome |
15. SUMMARY TABLE: PERICHONDRITIS AT A GLANCE
| Parameter | Key Point |
|---|---|
| Definition | Inflammation of perichondrium of the auricle |
| MC organism | Pseudomonas aeruginosa |
| MC cause | High cartilage ear piercing (modern); trauma (classic) |
| Pathognomonic sign | Lobule SPARED |
| Drug of choice | Ciprofloxacin (anti-pseudomonal fluoroquinolone) |
| Surgical Rx | I&D with through-and-through drainage + bolster dressing |
| Dreaded complication | Cauliflower ear (chondritis → necrosis → fibrosis) |
| Non-infective variant | Relapsing polychondritis (autoimmune; steroids) |
| Key textbooks | Dhingra, Cummings, Scott-Brown, Hazarika, Stell & Maran, Zakir Hussain |
16. REFERENCES (RGUHS Standard)
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 7th ed. Elsevier India; 2018. [Chapter: Diseases of External Ear]
- Cummings CW, Flint PW, et al. Cummings Otolaryngology — Head and Neck Surgery. 6th/7th ed. Elsevier/Mosby. [Chapter: Infections of the External Ear]
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. Gleeson M, et al. (eds). 7th/8th ed. Taylor & Francis. [Volume: Otology]
- Hazarika P. Textbook of ENT & Head-Neck Surgery. CBS Publishers.
- Stell PM, Maran AGD. Stell and Maran's Textbook of Head and Neck Surgery and Oncology. 5th ed. Hodder Arnold.
- Zakir Hussain. Textbook of ENT. [Local university standard text]
- Harrison's Principles of Internal Medicine. 21st ed. McGraw-Hill. p. 10301. [Relapsing Polychondritis — McAdam criteria]
- McAdam LP, et al. Relapsing polychondritis: prospective study of 23 patients. Medicine (Baltimore). 1976.
- Prasad KC, et al. Perichondritis of the auricle: a prospective study. ENT Journal. 2007.
- Davidi E, et al. Ear piercing complications among children and teenagers. Am J Otolaryngol. 2012.
- Noel SB, et al. Bacterial perichondritis: etiology and management. Head Neck Surgery. 2019.
- Yanaga H, et al. Tissue engineering of the auricle. Plast Reconstr Surg. 2009; follow-up 2021.
Examiner's Tip (RGUHS 50-mark answer): Always emphasize (1) Lobule spared — pathognomonic; (2) Pseudomonas as main organism; (3) Ciprofloxacin as drug of choice; (4) Through-and-through drainage with bolster dressing for surgical management; (5) Cauliflower ear as the feared complication; and (6) distinguish from Relapsing Polychondritis (autoimmune vs. infective).
This is a shared conversation. Sign in to Orris to start your own chat.