Management of cholesteatoma in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
cholesteatoma management surgery treatment
search_medical_text
cholesteatoma classification types pathology pathogenesis
search_medical_image
cholesteatoma ear diagram surgical approach mastoidectomy
GradeResponse
GradeResponse
GradeResponse
search_medical_text
cholesteatoma surgical techniques canal wall up canal wall down mastoidectomy tympanoplasty
search_medical_text
cholesteatoma recurrence residual second look surgery endoscopic ear surgery recent advances
Here is a comprehensive, exam-ready answer on the Management of Cholesteatoma for 50 marks, synthesized from Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Stell & Maran's Head & Neck Surgery, Dhingra's ENT, Hazarika's Textbook of ENT, and current literature — structured for RGUHS University examinations.
MANAGEMENT OF CHOLESTEATOMA
(50 Marks — RGUHS Pattern)
1. DEFINITION
Cholesteatoma is a non-neoplastic, expansile, destructive lesion composed of keratinizing stratified squamous epithelium within the middle ear, mastoid, or petrous bone, which accumulates desquamated keratin debris, destroys adjacent bone through enzymatic activity, and carries significant risk of serious complications.
(Harrison's Principles of Internal Medicine, 21st ed., p. 1023; Bailey & Love's Surgery, 28th ed., p. 779)
2. CLASSIFICATION
A. Congenital Cholesteatoma
- Behind an intact tympanic membrane (usually antero-superior quadrant)
- No prior ear disease, surgery, or perforation
- Levenson criteria: white mass medial to intact TM in a patient with no prior otorrhea or surgery
- More common in children; origin — epithelial rest (epidermoid formation theory)
B. Acquired Cholesteatoma
| Type | Characteristics |
|---|---|
| Primary Acquired | Arises from retraction pocket of pars flaccida (attic) — most common type |
| Secondary Acquired | Arises from pars tensa retraction or migration of squamous epithelium through a perforation |
| Post-traumatic | Implantation after trauma/surgery |
| Iatrogenic | After myringoplasty, grommets |
Location-based classification (Tos, 1988):
- Pars flaccida (attic) cholesteatoma — most common (80%)
- Pars tensa cholesteatoma
- Combined type
- Congenital
3. PATHOGENESIS
Four major theories exist (Cummings, 6th ed.):
╔══════════════════════════════════════════════════════╗
║ THEORIES OF PATHOGENESIS ║
╠══════════════════════════════════════════════════════╣
║ 1. INVAGINATION / RETRACTION POCKET THEORY ║
║ (Wittmaack, 1933) — Commonest accepted ║
║ Eustachian tube dysfunction → negative ME ║
║ pressure → retraction of pars flaccida → ║
║ pocket formation → accumulation of keratin ║
╠══════════════════════════════════════════════════════╣
║ 2. BASAL CELL HYPERPLASIA THEORY (Ruedi) ║
║ Proliferation of basal cells of pars flaccida ║
╠══════════════════════════════════════════════════════╣
║ 3. SQUAMOUS METAPLASIA THEORY (Sade) ║
║ Chronic infection → metaplasia of ME mucosa ║
╠══════════════════════════════════════════════════════╣
║ 4. IMMIGRATION THEORY (Habermann, Bezold) ║
║ Migration of squamous epithelium through ║
║ marginal perforation into middle ear ║
╚══════════════════════════════════════════════════════╝
Molecular basis of bone destruction:
- Matrix metalloproteinases (MMP-1, MMP-2, MMP-9) — collagen degradation
- Prostaglandins (PGE₂) — activate osteoclasts
- IL-1α, IL-1β, TNF-α — cytokine-mediated bone resorption
- Keratinocyte hyperproliferation (Ki-67 positive)
4. CLINICAL FEATURES
Symptoms
- Foul-smelling, scanty, non-pulsatile otorrhoea (hallmark) — does not respond to antibiotics
- Hearing loss — conductive (CHL) predominantly; mixed if cochlea involved
- Pain — in complicated cases
- Tinnitus, vertigo — if labyrinth eroded
Signs
- Attic perforation (pars flaccida) with white pearly/cheesy mass — pathognomonic
- Marginal perforation with cholesteatoma medially (pars tensa type)
- Aural polyp — highly suggestive (Bailey & Love, p. 779)
- Crust/wax in attic region
- Granulation tissue
Audiological findings
- Pure tone audiometry: CHL, often 30–60 dB HL
- Mixed HL when cochlear involvement
5. INVESTIGATIONS
┌─────────────────────────────────────────────────────┐
│ DIAGNOSTIC WORKUP │
├─────────────────────────────────────────────────────┤
│ 1. OTOSCOPY / OTOENDOSCOPY │
│ — Visualization of attic/marginal perforation │
│ — Keratin/white pearly mass │
├─────────────────────────────────────────────────────┤
│ 2. PURE TONE AUDIOMETRY │
│ — CHL / Mixed HL; Carhart's notch │
├─────────────────────────────────────────────────────┤
│ 3. CT SCAN TEMPORAL BONE (HRCT) │
│ — GOLD STANDARD for imaging │
│ — Soft tissue mass in attic/ME/mastoid │
│ — Bone erosion: scutum, ossicles (long │
│ process of incus — most common) │
│ — Tegmen, sinus plate, labyrinthine erosion │
├─────────────────────────────────────────────────────┤
│ 4. MRI TEMPORAL BONE (Non-EPI DWI) │
│ — Diffusion-weighted MRI (DWI/b1000) │
│ — Differentiates cholesteatoma from other │
│ soft tissue (high diffusion restriction) │
│ — Best for residual/recurrent detection │
│ — Non-echo planar DWI (HASTE/PROPELLER) — │
│ avoids artefact from bone │
├─────────────────────────────────────────────────────┤
│ 5. CULTURE & SENSITIVITY of discharge │
│ 6. TUNING FORK TESTS (Rinne, Weber) │
└─────────────────────────────────────────────────────┘
HRCT Findings in Cholesteatoma:
- Soft tissue mass in Prussak's space (pars flaccida) or ME
- Scutum erosion (blunting) — pathognomonic
- Long process of incus erosion — most common ossicular erosion
- Tegmen erosion → meningitis risk
- Posterior fossa plate erosion → sigmoid sinus thrombosis
- Labyrinthine erosion → fistula (lateral semicircular canal — most common)
6. AIMS OF SURGERY
The primary aims (Scott-Brown's Otorhinolaryngology, 8th ed.):
- Eradicate disease — complete removal of cholesteatoma matrix
- Create a safe, dry, trouble-free ear — prevent complications
- Preserve or restore hearing — tympanoplasty and ossiculoplasty
- Avoid recurrence/residual disease
Note: The priority order — SAFETY first, HEARING second
7. MANAGEMENT FLOWCHART
╔══════════════════════════════════════════════════════════════╗
║ CHOLESTEATOMA — MANAGEMENT ALGORITHM ║
╚══════════════════════════════════════════════════════════════╝
│
┌───────────────┴───────────────┐
▼ ▼
CONSERVATIVE SURGICAL
(TEMPORIZING ONLY) (DEFINITIVE Rx)
│ │
- Elderly, unfit │
- Aural toilet ┌──────┴──────┐
- Topical antibiotics ▼ ▼
- Regular follow-up CONGENITAL ACQUIRED
*(NOT curative)* CHOLESTEATOMA CHOLESTEATOMA
│ │
Usually canal │
wall up approach ┌──┴──────────────────┐
▼ ▼
PARS FLACCIDA PARS TENSA
(Attic Type) (Posterior type)
│
┌─────────────┴─────────────┐
▼ ▼
EXTENT OF DISEASE EXTENT OF DISEASE
LIMITED (early) EXTENSIVE
│ │
▼ ▼
Canal Wall UP (CWU) Canal Wall DOWN (CWD)
Mastoidectomy Mastoidectomy
+ Tympanoplasty + Meatoplasty
│ │
2nd Look at No 2nd look
9–12 months needed usually
8. SURGICAL MANAGEMENT (DETAILED)
PRE-OPERATIVE PREPARATION
- Complete audiological assessment
- HRCT temporal bone
- Informed consent (facial nerve risk, hearing loss, recurrence)
- Control of active infection (if possible)
- Aural toilet; culture-directed antibiotics
SURGICAL APPROACHES
A. CORTICAL/SIMPLE MASTOIDECTOMY
- Not used alone for cholesteatoma
- May be used as initial access
B. INTACT CANAL WALL (ICW) / CANAL WALL UP (CWU) MASTOIDECTOMY
Synonyms: Combined approach tympanoplasty (CAT), Posterior tympanotomy, ICW technique
Indications:
- Limited cholesteatoma confined to attic/mastoid
- Good pneumatization
- Serviceable contralateral hearing
- Cooperative patient for follow-up
- Congenital cholesteatoma
- Good Eustachian tube function
Steps:
1. Post-auricular incision (Wilde's incision)
2. Elevation of periosteum — exposure of mastoid cortex
3. Cortical mastoidectomy (Schwartze procedure)
— Removal of mastoid air cells
— Identification of: Tegmen plate (roof), Sigmoid sinus (posterior),
Lateral semicircular canal, Short process of incus (landmark),
Facial nerve (vertical segment)
4. Posterior tympanotomy (facial recess approach)
— Opening between: Facial nerve (medially), Chorda tympani (laterally)
— Access to posterior ME without touching canal wall
5. Removal of cholesteatoma matrix from attic + mastoid
6. Ossicular chain assessment
7. Tympanoplasty (underlay/overlay technique) with temporalis fascia/cartilage
8. Ossiculoplasty if required
9. Obliteration of mastoid cavity if needed
Advantages:
- Preserves anatomical canal
- No cavity problems
- Better hearing outcomes
- No lifelong cavity care
Disadvantages:
- Higher recurrence rate (15–40%)
- Residual disease risk
- Mandatory 2nd look surgery at 9–12 months
- Limited access to sinus tympani, tip cells
C. CANAL WALL DOWN (CWD) MASTOIDECTOMY / MODIFIED RADICAL MASTOIDECTOMY (MRM)
Steps:
1. Post-auricular incision
2. Cortical mastoidectomy as above
3. LOWERING of posterior canal wall (EAC posterior wall)
— Creates one large cavity (mastoid + EAC + ME)
4. Removal of all cholesteatoma
5. Saucerization — smooth, rounded cavity walls
6. MEATOPLASTY — enlargement of meatus for cavity aeration and cleaning
7. Preservation of ossicles if intact
8. Tympanoplasty (Atticotomy + reconstruction of ear drum)
9. Obliteration with musculoperiosteal flap/abdominal fat if needed
Indications:
- Extensive cholesteatoma
- Only hearing ear (safer access)
- Labyrinthine fistula
- Recurrent cholesteatoma after CWU
- Non-pneumatized mastoid
- Facial nerve dehiscence
- Intracranial complications
- Unreliable follow-up patient
Advantages:
- Direct visualization and complete removal
- Lower recurrence
- No need for routine 2nd look
- Safer in complications
Disadvantages:
- Cavity problem (discharge, debris accumulation)
- Lifelong cavity care
- Restriction on water activities
- Poorer hearing outcomes
- Larger post-op cavity
D. RADICAL MASTOIDECTOMY (RM)
- All of MRM + removal of remnant TM and ossicles
- Middle ear = part of mastoid cavity
- No tympanoplasty performed
- Indications: Extensive disease, very poor cochlear function, labyrinthine fistula with dead ear, intracranial complications, non-functional ear
COMPARISON TABLE: CWU vs CWD
| Feature | Canal Wall UP (CWU) | Canal Wall DOWN (CWD) |
|---|---|---|
| Posterior canal wall | Intact | Removed |
| Recurrence/residual | Higher (up to 40%) | Lower |
| 2nd look surgery | Required (9–12 months) | Usually not needed |
| Hearing outcome | Better | Poorer |
| Cavity problems | None | Present (lifelong) |
| Access to disease | Limited | Excellent |
| Meatoplasty | Not needed | Essential |
| Water restriction | No | Yes |
| Preferred in | Limited disease, children | Extensive disease, adults |
E. ATTICOTOMY (ATTIC EXPLORATION)
- Limited procedure for isolated attic cholesteatoma
- Removal of outer attic wall (scutum)
- Followed by reconstruction with cartilage
- Used in early/limited disease; good for congenital cholesteatoma
F. OBLITERATION TECHNIQUES
Used to eliminate dead space in CWD cavity:
- Bone pate — from mastoid drilling
- Hydroxyapatite granules/cement
- Abdominal fat obliteration
- Musculoperiosteal flap (Palva flap)
- Bondy's modified radical mastoidectomy — for limited pars flaccida cholesteatoma not extending below malleus
TYMPANOPLASTY (Hearing Reconstruction)
Wullstein Classification:
| Type | Procedure | Indication |
|---|---|---|
| Type I | Myringoplasty only — TM repair | Normal ossicular chain |
| Type II | Graft on incus/malleus | Malleus eroded |
| Type III | Graft on stapes head (Myringostapediopexy) | Incus + malleus eroded, stapes intact |
| Type IV | Graft on stapes footplate | Stapes suprastructure absent |
| Type V | Fenestration of SCC | Fixed footplate |
Ossiculoplasty options:
- Autograft — reshaped incus (most common)
- Homograft — cadaveric ossicles
- Alloplast (PORP/TORP) — partial/total ossicular replacement prosthesis (titanium, hydroxyapatite)
- PORP: Stapes head to TM/graft
- TORP: Footplate to TM/graft
- Cartilage interposition
9. ENDOSCOPIC EAR SURGERY (EES) — RECENT ADVANCES
(Key topic for current exams — RGUHS heavily tests this)
Transcanal Endoscopic Ear Surgery (TEES):
- Introduced by Thomassin (1990), popularized by Tarabichi, Marchese, Presutti
- 0°, 30°, 45° Hopkins rod endoscopes used through EAC
- Provides wide-angle, panoramic view of sinus tympani, facial recess, hypotympanum — areas blind to microscope
Advantages over microscope:
- No post-auricular incision
- Better visualization of hidden recesses (sinus tympani, anterior epitympanum, hypotympanum)
- Less tissue trauma
- Faster recovery
- Detection of residual cholesteatoma in "blind spots"
Disadvantages:
- One-handed surgery (scope in one hand)
- Learning curve
- Irrigation needed; no depth perception
- Heat generation from light source — facial nerve/cochlea thermal risk
- Cannot use drill and scope simultaneously
Current Consensus (ESCAT — European Consortium):
- TEES preferred for limited/congenital cholesteatoma
- Combined endoscopic-microscopic approach for extensive disease
10. SURGICAL MANAGEMENT OF COMPLICATIONS
Labyrinthine Fistula
- Most common: Lateral semicircular canal (LSC) fistula
- Diagnosis: fistula test (positive Hennebert sign/Tullio phenomenon)
- Confirmed on HRCT
Management (Quaranta classification):
Grade I — Perilabyrinthine bone erosion only → safe to remove matrix
Grade II — Fistula < 2mm, no endosteum breach → careful matrix removal,
seal with fascia/perichondrium
Grade III — Fistula > 2mm or labyrinthine breach →
In hearing ear: LEAVE matrix on fistula, seal over it
(planned residual — 2nd look + DWI-MRI surveillance)
In dead ear: open labyrinthectomy
Facial Nerve Paralysis
- Immediate: explore surgically within 24 hours
- Delayed (post-op): steroids, observation; decompress if no recovery in 6–8 weeks
- Intraoperative identification with facial nerve monitor is mandatory
Intracranial Complications (RGUHS favourite)
Management: Antibiotics + Surgery
- Meningitis → IV cefotaxime/ceftriaxone + urgent mastoidectomy
- Extradural abscess → drain at surgery
- Brain abscess → neurosurgical drainage + mastoidectomy
- Sigmoid sinus thrombosis → IV antibiotics, anticoagulation controversial, surgical skeletonization
11. SECOND-LOOK SURGERY
Indications:
- After CWU mastoidectomy — routine at 9–12 months
- Suspected residual cholesteatoma
- To perform staged ossicular reconstruction
Current trend (2020s):
- Non-EPI DWI-MRI at 12–18 months is replacing routine 2nd look
- If DWI negative → avoid surgery
- If DWI positive → proceed to 2nd look
- Sensitivity ~90%, specificity ~85% for residual cholesteatoma ≥3mm
(This is a key recent advance for RGUHS examinations)
12. MANAGEMENT FLOWCHART — DECISION ALGORITHM
DIAGNOSED CHOLESTEATOMA
│
┌───────┴────────┐
▼ ▼
Medically FIT Medically UNFIT
│ │
Surgery Aural toilet
(mainstay) Surveillance
│ (palliative)
▼
HRCT + Audiometry
│
┌────┴──────────────────┐
▼ ▼
CONGENITAL ACQUIRED
│ │
Transcanal/ ┌─────┴──────────────────────┐
Post-auricular ▼ ▼
Atticotomy or LIMITED DISEASE EXTENSIVE DISEASE
CWU + Tympanoplasty │ │
CWU + Posterior CWD + Meatoplasty
Tympanotomy + Tympanoplasty
+ Ossiculoplasty + Ossiculoplasty
│ │
2nd look at DWI-MRI at 12–18 months
9–12 months if positive → re-explore
(or DWI-MRI)
13. INTRAOPERATIVE IMAGE
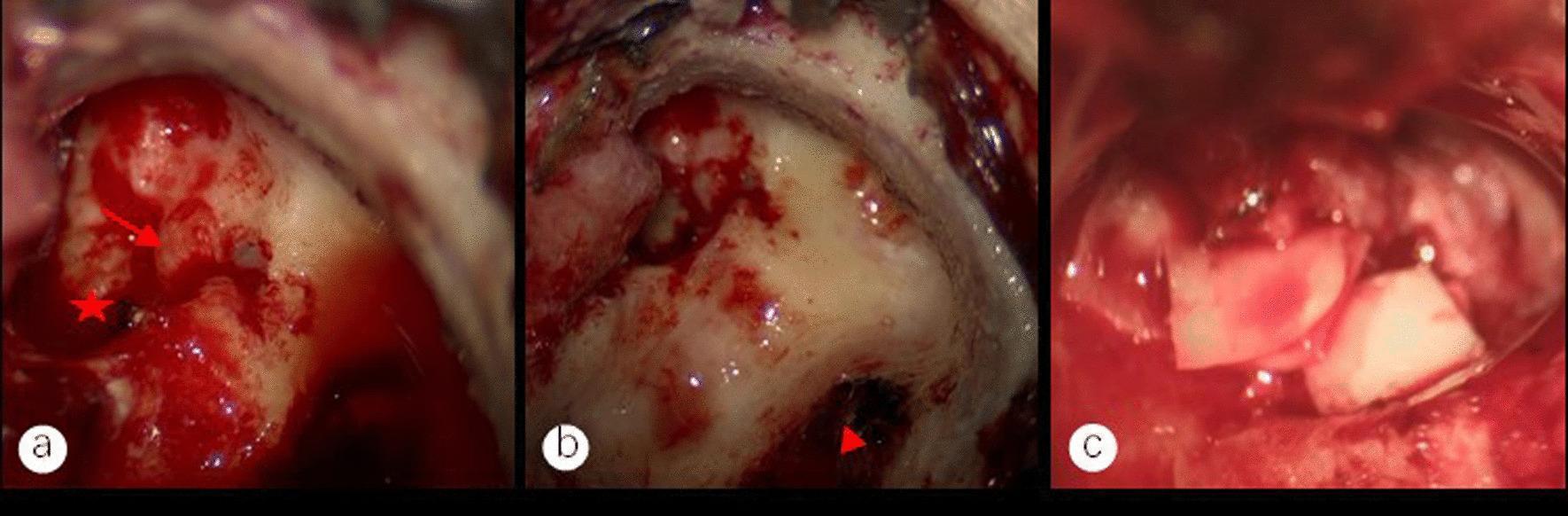
Figure: Intraoperative endoscopic images of modified mastoidectomy and tympanoplasty for middle ear cholesteatoma. (a) Exposed facial nerve canal (red arrow) and stapedial base (red star) after cholesteatoma removal. (b) Sigmoid sinus wall (red triangle) after mastoid bone removal. (c) Type III tympanoplasty using auricular cartilage graft for ossicular chain reconstruction to vestibular window.
(Source: PMC Clinical VQA Dataset — Otolaryngology)
14. RECENT ADVANCES IN CHOLESTEATOMA MANAGEMENT (2018–2024)
(RGUHS frequently tests recent advances)
1. Non-EPI DWI MRI (Diffusion-Weighted MRI)
- HASTE, PROPELLER, BLADE sequences
- Highly accurate for residual/recurrent cholesteatoma (cholesteatoma shows restricted diffusion — bright on DWI)
- Replaces routine 2nd look surgery in many centres
- European Academy of Otology and Neurotology (EAONO) recommends DWI-MRI as first-line surveillance
2. Fully Endoscopic Ear Surgery (FEES / TEES)
- Tarabichi's approach now widely adopted globally
- Exclusive endoscopic CWU mastoidectomy feasible for select cases
- Better sinus tympani visualization → reduced residual rates
3. Powered Instruments
- Microdebriders for cholesteatoma matrix dissection
- Reduces risk of matrix perforation
4. Laser-Assisted Surgery
- CO₂ laser, KTP laser, diode laser
- Useful near facial nerve, ossicles, fistula area
- Vaporizes matrix without traction
5. Otoendoscopy in Office Setting
- Narrow band imaging (NBI) — experimental for early cholesteatoma detection
6. Molecular Targeted Therapy (Experimental)
- MMP inhibitors, anti-RANKL antibodies under research
- Aim to halt bone erosion pre-operatively
- Not yet in clinical practice
7. Robot-Assisted Cochlear/Mastoid Surgery
- Experimental; Heliodor, OAKCP robot systems (University of Bern)
- Precise canal wall opening without damaging structures
8. PROPELLER/BLADE DWI MRI Protocol
- Overcomes susceptibility artifacts near temporal bone
- Now accepted as gold standard for post-operative surveillance
9. Cholesteatoma Staging — EAONO/JOS Classification (2017)
(James et al. — now used in research and audit)
Stage I: Cholesteatoma confined to one anatomical sub-site (e.g., pars flaccida)
Stage II: Extension to 2 or more sub-sites without complications
Stage III: Extension to contiguous structures but intracranial compartment not involved
Stage IV: Intracranial extension or involvement of the only hearing ear
Stage II: Extension to 2 or more sub-sites without complications
Stage III: Extension to contiguous structures but intracranial compartment not involved
Stage IV: Intracranial extension or involvement of the only hearing ear
15. COMPLICATIONS OF CHOLESTEATOMA (RGUHS MUST-KNOW)
Extracranial
| Complication | Notes |
|---|---|
| Labyrinthine fistula | LSC — most common; vertigo, positive fistula test |
| Facial nerve palsy | Dehiscent nerve in ME |
| Subperiosteal abscess | Mastoid cortex erosion |
| Bezold's abscess | Tip cells erosion → abscess along sternomastoid |
| Citelli's abscess | Digastric groove erosion |
| Gradenigo's syndrome | Petrous apicitis — V, VI nerve palsy + otorrhoea triad |
| Petrous apicitis | Erosion into petrous apex |
Intracranial
- Meningitis (most common intracranial complication)
- Extradural abscess
- Subdural abscess
- Brain abscess (temporal lobe / cerebellar)
- Sigmoid sinus thrombosis
- Otitic hydrocephalus
16. PROGNOSIS AND FOLLOW-UP
- Recurrence rate: CWU — 15–40%; CWD — 5–15%
- Residual disease: Up to 30% after CWU (due to hidden recesses)
- Follow-up: Every 6 months initially, then annually
- DWI-MRI at 12–18 months post-op for CWU patients
- Long-term audiological review and hearing aid fitting if needed
- Children — higher recurrence (aggressive disease, poor ET function)
17. SUMMARY TABLE — SURGICAL OPTIONS
| Procedure | Cavity | Recurrence | Hearing | Meatoplasty | 2nd Look |
|---|---|---|---|---|---|
| Atticotomy | No | Moderate | Good | No | No |
| CWU Mastoidectomy | No | High | Good | No | Yes |
| CWD / MRM | Yes | Low | Moderate | Yes | Usually No |
| Radical Mastoidectomy | Yes | Lowest | Poor/None | Yes | No |
| Bondy's MRM | Yes (limited) | Low | Good | Yes | No |
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed. — Gleeson et al., Vol. 3, Otology. pp. 3314–3360
- Cummings Otolaryngology: Head and Neck Surgery, 7th ed. — Flint et al. Chapter on Chronic Otitis Media and Cholesteatoma
- Stell and Maran's Head and Neck Surgery, 4th ed. — O'Brien; Chapter — Ear disease, pp. 180–210
- Dhingra's Diseases of Ear, Nose and Throat, 7th ed. — P.L. Dhingra; Chapter 12 — Chronic Suppurative Otitis Media, pp. 85–98
- Hazarika's Textbook of ENT and HNS, 3rd ed. — Chapter on CSOM Unsafe type and cholesteatoma
- Zakir Hussain's Textbook of ENT, relevant sections on mastoid surgery and cholesteatoma
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 779
- Harrison's Principles of Internal Medicine, 21st ed., p. 1023
- EAONO/JOS Classification of Cholesteatoma — James et al., Otology & Neurotology, 2017
- Non-echo-planar DWI MRI for cholesteatoma — Profant et al., Eur Arch Otorhinolaryngol, 2020
- Endoscopic ear surgery for cholesteatoma — Tarabichi M., Laryngoscope, 2010; Presutti et al., 2014
- ESCAT consensus on endoscopic cholesteatoma surgery — Eur Arch Otorhinolaryngol, 2021
RGUHS Exam Tip: For a 50-mark answer, always cover — Definition → Classification → Pathogenesis → Clinical features → Investigations (emphasize HRCT + DWI-MRI) → Aims of surgery → Detailed surgical techniques (CWU vs CWD with comparison table) → Tympanoplasty types → Complications management → Recent advances (DWI-MRI, TEES, staging) → Flowchart. Diagrams and tables carry significant marks.
This is a shared conversation. Sign in to Orris to start your own chat.