Diabetes mellitus from basic to advance
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus" AND management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from authoritative sources. Let me write the complete diabetes mellitus overview from basic to advanced.
Diabetes Mellitus: Basic to Advanced
Sources: Harrison's Principles of Internal Medicine 22E (2025), Guyton & Hall Textbook of Medical Physiology, and current evidence.
1. Definition and Overview
Diabetes mellitus (DM) is a syndrome of impaired carbohydrate, fat, and protein metabolism caused by either lack of insulin secretion or decreased sensitivity of tissues to insulin. It is defined by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The consequences span the entire body - from acute life-threatening emergencies to slow, progressive vascular injury over decades.
- Globally: >500 million people have DM; prevalence continues to rise
- Leading cause of new blindness (ages 20-74), end-stage renal disease, and non-traumatic lower-limb amputation
2. The Pancreas and Normal Glucose Physiology
Islets of Langerhans
The pancreas contains 1-2 million islets of Langerhans, each about 0.3 mm in diameter. Each islet contains:
| Cell Type | Proportion | Hormone Secreted |
|---|---|---|
| Beta (β) cells | ~60% | Insulin + Amylin (IAPP) |
| Alpha (α) cells | ~25% | Glucagon |
| Delta (δ) cells | ~10% | Somatostatin |
| PP cells | Small | Pancreatic polypeptide |
Cell-to-cell communication is key: insulin inhibits glucagon secretion; amylin inhibits insulin secretion; somatostatin inhibits both.
How Insulin Is Secreted (Glucose-Stimulated Insulin Secretion)
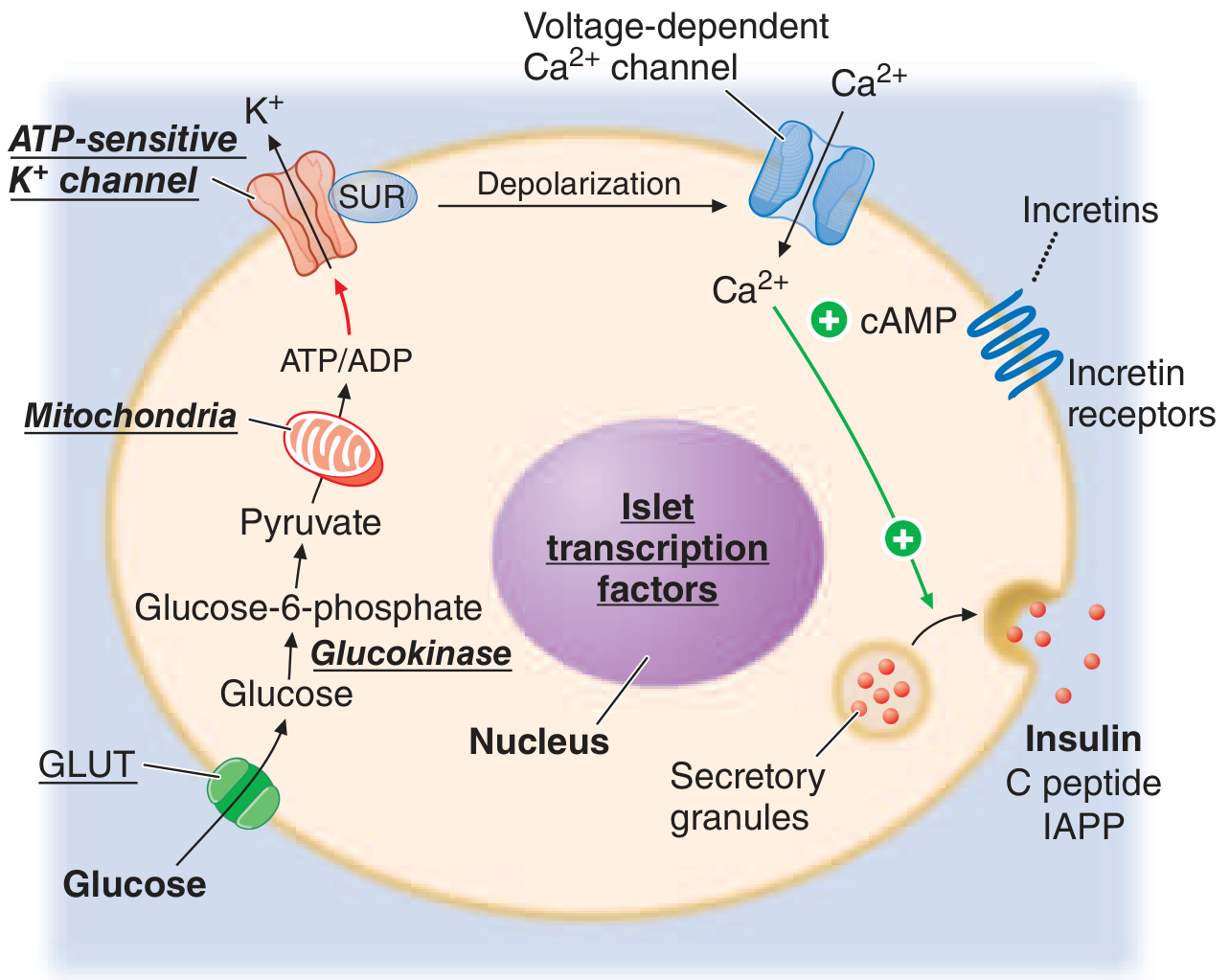
Glucose enters beta cells via GLUT transporters → Glucokinase phosphorylates it to Glucose-6-phosphate → Glycolysis generates ATP → Elevated ATP:ADP ratio closes ATP-sensitive K⁺ channels (K_ATP) → Membrane depolarization → Voltage-gated Ca²⁺ channels open → Ca²⁺ influx → Insulin granule exocytosis. Incretins (GLP-1, GIP) amplify this via cAMP. Sulfonylureas act on the SUR subunit of the K_ATP channel to mimic this effect.
(Harrison's Principles of Internal Medicine 22E, p. 3242)
Insulin's Metabolic Actions
Insulin acts on three main target tissues:
Liver:
- Inactivates phosphorylase → halts glycogenolysis
- Activates glucokinase → traps glucose-6-phosphate intracellularly
- Activates glycogen synthase → promotes glycogen storage (up to 100g in liver)
- Suppresses gluconeogenesis
Skeletal Muscle:
- Stimulates GLUT4 translocation to cell surface → increases glucose uptake 15-fold
- Promotes glycogen synthesis (up to 2-3% muscle concentration)
- Stimulates protein synthesis
Adipose Tissue:
- Activates lipoprotein lipase → promotes fat storage
- Inhibits hormone-sensitive lipase → suppresses lipolysis and free fatty acid release
Insulin Receptor Signaling
Insulin binds its receptor → activates intrinsic tyrosine kinase → receptor autophosphorylation → recruits Insulin Receptor Substrates (IRS proteins) → activates PI3-kinase pathway → GLUT4 translocation → glucose uptake in muscle and fat.
3. Classification of Diabetes Mellitus
(ADA/Harrison's Classification)
Type 1 DM
- Autoimmune or idiopathic destruction of beta cells
- Absolute insulin deficiency
- ~5-10% of all DM cases
- Often presents before age 14 (juvenile DM) but can occur at any age
Type 2 DM
- Insulin resistance + progressive beta cell failure
- Initially non-insulin dependent; may require insulin later
- ~90-95% of all DM cases
- Strongly associated with obesity, physical inactivity, family history
MODY (Maturity-Onset Diabetes of the Young) / Monogenic Diabetes
- Single gene defects in beta cell function: GCK (glucokinase), HNF-1α, HNF-4α, HNF-1β, IPF-1, NeuroD1, KLF11, CEL, PAX4, INS, BLK, ABCC8, KCNJ11, APPL1
- Mutations in the K_ATP channel (ABCC8, KCNJ11) can cause either neonatal DM or MODY
- Autosomal dominant; does NOT require insulin initially
Gestational Diabetes Mellitus (GDM)
- Glucose intolerance developing in the 2nd or 3rd trimester
- Caused by pregnancy-related insulin resistance from placental hormones
- Affects ~16% of pregnancies worldwide (IDF, 2021)
- 35-60% risk of progressing to T2DM within 10-20 years
- ADA recommends lifelong screening every ≥3 years post-GDM
Secondary / Other Causes
| Category | Examples |
|---|---|
| Exocrine pancreas disease | Pancreatitis, pancreatectomy, cystic fibrosis, hemochromatosis |
| Endocrinopathies | Acromegaly, Cushing's syndrome, glucagonoma, pheochromocytoma, hyperthyroidism |
| Drug-induced | Glucocorticoids, tacrolimus, thiazides, antipsychotics (2nd-gen), HIV antiretrovirals, PCSK9 inhibitors, immune checkpoint inhibitors |
| Genetic syndromes | Down, Klinefelter, Turner, Wolfram, Prader-Willi, Friedreich's ataxia |
| Infections | Congenital rubella, CMV, coxsackievirus |
| Immune-mediated | Stiff-person syndrome, anti-insulin receptor antibodies |
(Harrison's Principles of Internal Medicine 22E, p. 3229)
4. Pathophysiology
Type 1 DM
- Autoimmune destruction of beta cells, mediated by T cells and autoantibodies against islet cell antigens (ICA, anti-GAD65, anti-IA-2, anti-insulin, anti-ZnT8)
- HLA associations: HLA-DR3 and HLA-DR4 (especially DR3/DR4 heterozygotes) confer highest risk; HLA-DR2 is protective
- Viral triggers (enterovirus), molecular mimicry, and genetic susceptibility interact
- Results in absolute insulin deficiency → unchecked glucagon secretion → hepatic glucose overproduction + peripheral underutilization
- Without insulin: lipolysis is unchecked → excess free fatty acids → ketone body formation (acetoacetate, β-hydroxybutyrate) → diabetic ketoacidosis (DKA)
Type 2 DM - "Ominous Octet" (DeFronzo)
T2DM is a multi-organ defect:
- Insulin resistance in muscle - impaired GLUT4 translocation, reduced glucose uptake
- Hepatic insulin resistance - failure to suppress gluconeogenesis
- Beta cell failure - progressive loss of insulin secretory capacity (often ~50% lost by diagnosis)
- Incretin defect - reduced GLP-1 secretion + response
- Alpha cell dysfunction - hyperglucagonemia even in the fed state
- Kidney - increased glucose reabsorption by SGLT2
- Brain - insulin resistance centrally, impaired satiety signaling
- Adipose tissue - excess lipolysis, ectopic fat deposition worsening insulin resistance
The central sequence: insulin resistance → compensatory hyperinsulinemia → beta cell exhaustion → overt hyperglycemia.
5. Diagnosis
Diagnostic Criteria (ADA 2024)
| Test | Prediabetes | Diabetes |
|---|---|---|
| Fasting Plasma Glucose (FPG) | 100-125 mg/dL (5.6-6.9 mmol/L) | ≥126 mg/dL (7.0 mmol/L) |
| 2-h Glucose (75g OGTT) | 140-199 mg/dL (7.8-11.0 mmol/L) | ≥200 mg/dL (11.1 mmol/L) |
| HbA1c | 5.7-6.4% (39-47 mmol/mol) | ≥6.5% (48 mmol/mol) |
| Random Glucose | - | ≥200 mg/dL + symptoms |
- Any single criterion must be confirmed by repeat testing (except when symptoms + random ≥200 mg/dL)
- Renal threshold for glucosuria: ~200 mg/dL (11 mmol/L)
Additional Tests
- C-peptide: low/absent in T1DM; normal/elevated in T2DM
- Islet autoantibodies: confirm T1DM (anti-GAD65 is most sensitive)
- HbA1c: reflects mean glucose over ~3 months (weighted toward recent weeks); affected by conditions that alter RBC lifespan (hemolytic anemia → falsely low; iron deficiency → falsely high)
6. Clinical Features
Acute Symptoms (Hyperglycemia)
- Polyuria - osmotic diuresis from glucosuria
- Polydipsia - secondary to dehydration from osmotic diuresis
- Polyphagia - cellular starvation despite elevated blood glucose
- Weight loss - catabolism of fat and protein (especially T1DM)
- Blurred vision - osmotic changes in lens
- Fatigue, weakness
T1DM vs T2DM Clinical Comparison
| Feature | Type 1 | Type 2 |
|---|---|---|
| Age at onset | Usually <30 (but any age) | Usually >40 (increasingly younger) |
| Body habitus | Normal/thin | Overweight/obese |
| Onset | Acute (days-weeks) | Insidious (years) |
| Insulin dependence | Immediate, lifelong | May not require initially |
| Ketosis | Prone | Rare (unless stress) |
| Autoantibodies | Present | Absent |
| C-peptide | Very low/absent | Normal or elevated early |
| Family history | Less strong | Strong |
(Guyton & Hall Textbook of Medical Physiology, Table 79.3)
7. Acute Complications
Diabetic Ketoacidosis (DKA)
- Predominantly T1DM (can occur in T2DM with stress)
- Triad: hyperglycemia + ketonemia/ketonuria + metabolic acidosis
- Precipitants: infections, missed insulin, new T1DM diagnosis, surgery
- Pathophysiology: absolute insulin deficiency → unchecked glucagon → lipolysis → free fatty acids → hepatic ketogenesis → anion gap metabolic acidosis
- Blood glucose: typically 300-600 mg/dL; pH <7.3; bicarbonate <18
- Treatment: IV fluids, insulin infusion, potassium replacement, monitor glucose/electrolytes hourly
Hyperosmolar Hyperglycemic State (HHS)
- Predominantly T2DM (elderly)
- Severe hyperglycemia (glucose often >600 mg/dL) + profound dehydration + altered consciousness
- No significant ketosis (residual insulin sufficient to suppress ketogenesis)
- Serum osmolality >320 mOsm/kg
- Mortality ~5-20%
Hypoglycemia
- Blood glucose <70 mg/dL (symptomatic threshold)
- Causes: excess insulin dose, missed meals, exercise, alcohol
- Symptoms: adrenergic (tremor, palpitations, sweating, anxiety) → neuroglycopenic (confusion, seizure, coma)
- Treatment: 15g fast-acting carbohydrate (rule of 15); glucagon IM if unconscious
- Hypoglycemia unawareness: autonomic neuropathy → loss of adrenergic warning signs; more common with recurrent hypoglycemia
8. Chronic Complications
Chronic complications arise from sustained hyperglycemia causing:
- Non-enzymatic glycation of proteins (AGEs - Advanced Glycation End-products)
- Polyol pathway activation (sorbitol accumulation)
- Protein kinase C activation
- Oxidative stress
- Hexosamine pathway activation
All five mechanisms converge to damage the vascular endothelium.
Microvascular Complications
Diabetic Retinopathy (most common cause of new blindness, ages 20-74 in US)
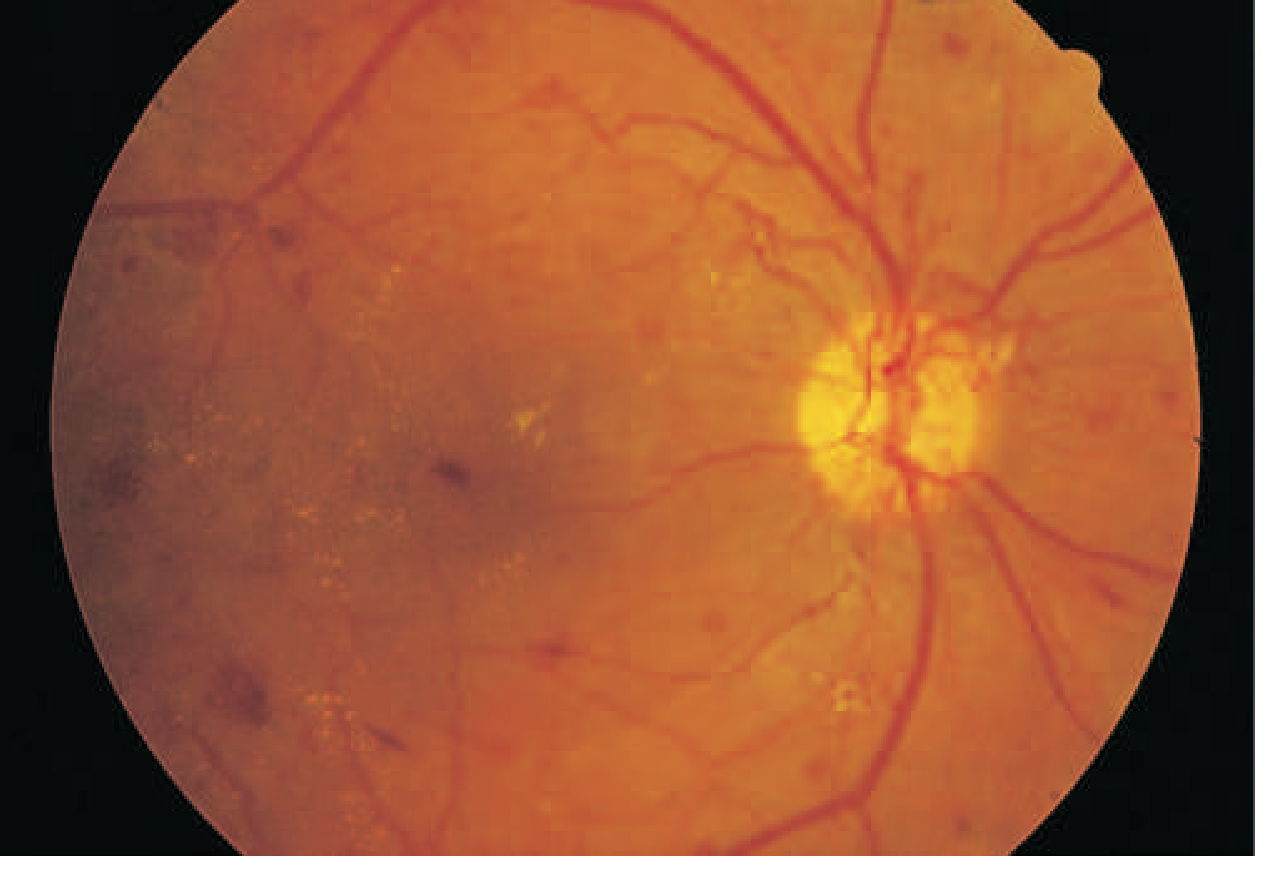
This fundus photo shows neovascularization from the optic disc, scattered hemorrhages, and yellow exudates - hallmarks of proliferative diabetic retinopathy requiring urgent panretinal laser photocoagulation.
- Non-proliferative (NPDR): microaneurysms, blot hemorrhages, cotton-wool spots, venous beading, intraretinal microvascular abnormalities (IRMAs)
- Proliferative (PDR): neovascularization → vitreous hemorrhage → traction retinal detachment
- Diabetic Macular Edema (DME): can occur at any stage; leading cause of vision loss
- Management: tight glycemic + BP control; anti-VEGF injections (ranibizumab, bevacizumab) for DME/PDR; laser photocoagulation for PDR
(Harrison's Principles of Internal Medicine 22E, p. 3267)
Diabetic Nephropathy
- Leading cause of end-stage renal disease (ESRD) globally
- Stages: hyperfiltration → microalbuminuria (30-300 mg/day) → macroalbuminuria (>300 mg/day) → declining GFR → ESRD
- Pathology: Kimmelstiel-Wilson nodular glomerulosclerosis (pathognomonic), diffuse mesangial expansion, basement membrane thickening
- Management: ACE inhibitors or ARBs (first-line for proteinuria); SGLT2 inhibitors (dapagliflozin, empagliflozin) have proven renoprotective effects; tight glucose + BP control
Diabetic Neuropathy (most common complication overall)
- Distal symmetric polyneuropathy (DSPN): classic "stocking-glove" distribution; numbness, tingling, burning pain, loss of vibration and position sense
- Autonomic neuropathy: cardiovascular (orthostatic hypotension, resting tachycardia, cardiac denervation); GI (gastroparesis - delayed gastric emptying, constipation/diarrhea); urogenital (erectile dysfunction, neurogenic bladder); sudomotor dysfunction
- Mononeuropathies: CN III palsy (painful, pupil-sparing - distinguishes from aneurysm), carpal tunnel, foot drop
- Diabetic amyotrophy (Bruns-Garland): proximal asymmetric muscle weakness/pain; immune-mediated
- Management: tight glycemic control (slows progression); pregabalin/gabapentin, duloxetine, TCAs, capsaicin for pain
Macrovascular Complications
DM accelerates atherosclerosis 2-4x compared to the non-diabetic population.
- Coronary artery disease: leading cause of death in T2DM; often "silent MI" due to autonomic neuropathy
- Cerebrovascular disease: 2-4x increased stroke risk
- Peripheral arterial disease: 10x increased risk of lower-limb amputation
Diabetic Foot:
Triad of neuropathy + peripheral arterial disease + impaired immunity → ulceration, infection, gangrene. Wagner classification grades 0-5 for clinical management.
9. Management
Glycemic Targets
| Parameter | General Target | High-risk (elderly/hypoglycemia-prone) |
|---|---|---|
| HbA1c | <7.0% (53 mmol/mol) | <8.0% |
| Fasting glucose | 80-130 mg/dL | Individualized |
| Peak postprandial | <180 mg/dL | Individualized |
Non-Pharmacologic: Lifestyle
- Medical nutrition therapy: carbohydrate counting, Mediterranean/DASH diet, caloric restriction
- Physical activity: 150 min/week moderate aerobic + resistance training
- Weight loss: 5-7% body weight loss can prevent/delay T2DM (DPP trial)
- Self-monitoring of blood glucose (SMBG) or continuous glucose monitoring (CGM)
Pharmacotherapy - Type 2 DM
Step 1: Metformin (first-line unless contraindicated)
- Mechanism: Activates AMPK → suppresses hepatic gluconeogenesis; modest improvement in insulin sensitivity
- Benefits: No hypoglycemia, weight neutral/mild loss, cheap, CV neutral/slightly beneficial, renal protective at low doses
- Contraindications: eGFR <30 mL/min (risk of lactic acidosis), active liver disease, contrast procedures
- HbA1c reduction: ~1-1.5%
Step 2: Add second agent based on comorbidities
GLP-1 Receptor Agonists (semaglutide, liraglutide, dulaglutide, exenatide)
- Mechanism: Mimic endogenous GLP-1 → glucose-dependent insulin secretion + glucagon suppression + gastric emptying delay + central satiety
- Benefits: Significant weight loss (5-15%), CV benefit (LEADER, SUSTAIN-6 trials), renal protection
- SE: Nausea/vomiting/diarrhea (common early), pancreatitis (rare), worsening retinopathy with rapid glucose lowering
- Recent 2025 meta-analysis: GLP-1 RAs effective and safe in pediatric obesity/T2DM (PMID: 40952752)
SGLT2 Inhibitors (empagliflozin, dapagliflozin, canagliflozin)
- Mechanism: Block SGLT2 in proximal tubule → prevent reabsorption of ~90% filtered glucose → glucosuria + osmotic diuresis
- Benefits: Weight loss, BP reduction, proven heart failure benefit (reduces hospitalization by ~35%), proven renal benefit (reduces progression to ESRD), cardiorenal protection independent of glucose-lowering
- SE: Urogenital infections (candida), Fournier's gangrene (rare), DKA (rare in T2DM), euglycemic DKA, polyuria, dehydration
DPP-4 Inhibitors (sitagliptin, saxagliptin, linagliptin, alogliptin)
- Mechanism: Inhibit dipeptidyl peptidase-4 → prevent degradation of endogenous GLP-1 and GIP → prolonged incretin effect
- Benefits: Weight neutral, low hypoglycemia risk, oral, well tolerated
- SE: Nasopharyngitis, pancreatitis (rare), joint pain (rare)
- HbA1c reduction: ~0.5-0.8%
Thiazolidinediones / Glitazones (pioglitazone, rosiglitazone)
- Mechanism: Activate PPARγ → improve peripheral insulin sensitivity + reduce hepatic glucose production
- Benefits: Durable effect, pioglitazone reduces CV events (PROactive trial)
- SE: Weight gain, fluid retention (contraindicated in CHF), bone fractures, bladder cancer risk (pioglitazone)
Sulfonylureas (glipizide, glibenclamide/glyburide, glimepiride)
- Mechanism: Bind SUR1 subunit of K_ATP channel on beta cells → channel closure → depolarization → insulin secretion (glucose-independent)
- Benefits: Cheap, effective (HbA1c -1 to -1.5%)
- SE: Hypoglycemia (significant risk), weight gain; older generation (glibenclamide) highest hypoglycemia risk
GIP/GLP-1 Dual Agonist (Tirzepatide)
- Dual agonism of GIP + GLP-1 receptors
- Superior HbA1c reduction and weight loss compared to semaglutide alone (SURPASS trials)
- Approved for T2DM (2022) and obesity (2023 in US)
Insulin Therapy in T2DM
Needed when: HbA1c remains uncontrolled on oral agents, during acute illness/surgery, pregnancy, or when beta cell failure is advanced.
Pharmacotherapy - Type 1 DM
T1DM requires complete insulin replacement for survival. The goal is to mimic physiologic insulin delivery:
Insulin preparations:
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting | Aspart, Lispro, Glulisine | <15 min | 30-90 min | 3-5 h |
| Rapid, inhaled | Technosphere insulin | <15 min | 1-2 h | 3 h |
| Short-acting | Regular insulin | 30-60 min | 2-3 h | 4-8 h |
| Intermediate | NPH | 2-4 h | 4-10 h | 10-16 h |
| Long-acting | Glargine | 2-4 h | Flat | 20-24 h |
| Ultra-long | Degludec | 1-9 h | Flat | >42 h |
(Harrison's Principles of Internal Medicine 22E, p. 3249)
Intensive insulin regimens:
- Multiple Daily Injections (MDI): 1-2 basal injections + rapid-acting bolus with each meal
- Continuous Subcutaneous Insulin Infusion (CSII/insulin pump): Programmable basal rates + boluses
- Automated Insulin Delivery (AID/"closed loop"): CGM + pump + algorithm that auto-adjusts basal rate in real time; some deliver correction boluses (hybrid closed loop)
- Sensor-Augmented Pump (SAP): CGM + pump, with auto-suspend feature when glucose falls/predicted to fall
Targets in T1DM (DCCT trial principles): Intensive glycemic control (HbA1c ~7%) reduced microvascular complications by 50-76% vs conventional therapy.
10. Advanced Topics
Immunotherapy in T1DM
- Teplizumab (anti-CD3 antibody): FDA-approved (2022) to delay clinical T1DM in at-risk individuals (stage 2 T1DM); median delay of ~2 years
- Screens high-risk relatives with 2+ islet autoantibodies + dysglycemia
Beta Cell Replacement
- Pancreas transplantation: Primarily for T1DM patients undergoing simultaneous kidney transplant; insulin independence in ~80% at 1 year
- Islet transplantation (Edmonton Protocol): Infusion of donor islets into portal vein; requires immunosuppression; currently investigational for recurrent severe hypoglycemia
- Stem cell-derived beta cells: Multiple clinical trials underway; Vertex Pharmaceuticals (VX-880, VX-264) showing promising results in 2024-2025
Cardiovascular Risk Reduction (ASCVD)
DM confers equivalent CV risk to established coronary artery disease in some guidelines. Key interventions:
- Statins: All T2DM patients aged 40-75 should receive moderate-to-high intensity statin (ADA 2024)
- BP target: <130/80 mmHg (ACE-I or ARB preferred, especially with proteinuria)
- SGLT2 inhibitors + GLP-1 RAs have independent CV benefits beyond glucose lowering and should be prioritized in patients with established ASCVD, HF, or CKD regardless of baseline HbA1c
- Aspirin: Low-dose for secondary prevention; primary prevention only if >10% 10-year ASCVD risk
Monogenic Diabetes
- MODY subtypes require genetic testing; some respond to sulfonylureas (HNF-1α/4α MODY) rather than insulin
- Neonatal DM from KCNJ11 or ABCC8 mutations often switches from insulin to high-dose sulfonylureas
Diabetes in Special Populations
- Pregnancy: Target HbA1c <6% if achievable without hypoglycemia; insulin is the standard (metformin and glyburide cross the placenta); close fetal monitoring; GDM screening at 24-28 weeks
- CKD: Dose-adjust/avoid metformin at eGFR <30; prefer linagliptin (no renal excretion); SGLT2i renoprotective down to eGFR 20 for cardiorenal indication
- Elderly: Relax HbA1c to 7.5-8.5%; avoid hypoglycemia risk (falls, fractures, dementia association); prefer DPP-4i, GLP-1 RA with caution re: GI effects
Emerging Therapies (2024-2026)
- Oral GLP-1 RAs: Oral semaglutide (Rybelsus) widely available; newer higher-dose oral formulations in trials
- Triple agonists (GLP-1/GIP/glucagon): Retatrutide and others in Phase 3 trials
- Closed-loop insulin delivery: Second-generation AID systems approaching full automation
- GLP-1 RAs in T1DM: Adjunct use to reduce insulin doses and glycemic variability (off-label, evidence building; PMID: 40952752 in pediatric T2DM)
11. Monitoring and Screening
- HbA1c: Every 3 months if uncontrolled; every 6 months if at target
- Annual: Urine albumin-to-creatinine ratio (ACR), serum creatinine/eGFR, lipid panel, ophthalmologic exam (dilated fundus or retinal photography), foot exam (monofilament, vibration, pulses)
- Screening for T2DM: All adults ≥35 years; earlier if BMI ≥25 + 1 risk factor (family history, GDM, prediabetes, high-risk ethnicity)
- Thyroid function (TSH): Screen in T1DM (associated autoimmune disease)
- Celiac disease antibodies: Screen in T1DM
Summary Table: Key Distinguishing Features
| T1DM | T2DM | MODY | GDM | |
|---|---|---|---|---|
| Mechanism | Autoimmune beta cell destruction | Insulin resistance + beta cell failure | Single gene mutation | Placental insulin resistance |
| Age | Any (often <30) | Usually >40 | <25 | Pregnancy |
| Genetics | Polygenic + HLA | Polygenic | Autosomal dominant | Complex |
| Autoantibodies | Yes | No | No | No |
| C-peptide | Low/absent | Normal-high early | Variable | Normal |
| Insulin needed | Always | Eventually | Sometimes | Often |
| Ketosis risk | High | Low | Low | Low |
Key Recent Evidence (2025):
- GLP-1 RAs are effective and safe in children/adolescents with obesity or T2DM [Systematic Review/Meta-Analysis, JAMA Pediatrics, 2025 - PMID: 40952752]
- GLP-1 RA-associated GI adverse events comprehensively characterized [Meta-Analysis, Gastroenterology, 2025 - PMID: 40499738]
- Digital interventions improve T2DM self-management outcomes [Systematic Review, J Med Internet Res, 2024 - PMID: 39037772]
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill); Guyton and Hall Textbook of Medical Physiology; ADA Standards of Medical Care in Diabetes 2024; PubMed recent evidence.
Note
Asking for Preferences
Reading File
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace
Running Command
mkdir -p /home/daytona/workspace/diabetes-notes
This is a shared conversation. Sign in to Orris to start your own chat.