Bells palsy in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
Bell's palsy facial nerve anatomy etiology pathophysiology
search_medical_text
Bell's palsy clinical features grading House Brackmann diagnosis investigations
GradeResponse
GradeResponse
search_medical_text
Bell's palsy treatment management steroids antiviral prognosis recovery
search_medical_image
Bell's palsy facial nerve anatomy diagram course segments
GradeResponse
Here is a comprehensive, exam-oriented write-up on Bell's Palsy for 50 marks, structured according to RGUHS university standards, integrating Scott-Brown, Cummings, Stell & Maran, Zakir Hussain, Dhingra, Hazarika, Harrison's Principles, and recent literature.
BELL'S PALSY
(Idiopathic Facial Nerve Palsy)
50-Mark Answer | RGUHS ENT
DEFINITION
Bell's palsy is an acute, unilateral, lower motor neuron (LMN) facial nerve palsy of idiopathic origin, characterized by sudden onset paralysis of all muscles of facial expression on one side, without any detectable underlying cause.
(Dhingra, 7th ed.; Hazarika ENT)
Named after Sir Charles Bell (1821), who described the function of the facial nerve.
SURGICAL ANATOMY OF THE FACIAL NERVE
(Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology)
The facial nerve (CN VII) is a mixed nerve with:
- Motor — muscles of facial expression, stapedius, stylohyoid, posterior belly of digastric
- Sensory (special) — taste from anterior 2/3 of tongue via chorda tympani
- Parasympathetic — lacrimal gland (via greater superficial petrosal nerve/GSPN), submandibular and sublingual glands (via chorda tympani)
- General somatic afferent — skin of concha, retroauricular area
Segments of the Facial Nerve
| Segment | Course | Length | Key Branches |
|---|---|---|---|
| Intracranial | Pons → IAC | ~24 mm | — |
| Meatal (IAC) | IAC fundus | ~8 mm | — |
| Labyrinthine | IAC → Geniculate ganglion | ~4 mm | Greater superficial petrosal nerve (GSPN) |
| Tympanic (horizontal) | Geniculate ganglion → Pyramidal eminence | ~13 mm | Nerve to stapedius |
| Mastoid (vertical/descending) | Pyramidal eminence → Stylomastoid foramen | ~20 mm | Chorda tympani |
| Extratemporal | Parotid gland → Face | — | Temporal, zygomatic, buccal, marginal mandibular, cervical (TZBMC) |
The labyrinthine segment is the narrowest segment (0.68 mm diameter) with the least blood supply — this is the critical site of compression in Bell's palsy (Cummings, 7th ed.; Stell & Maran)
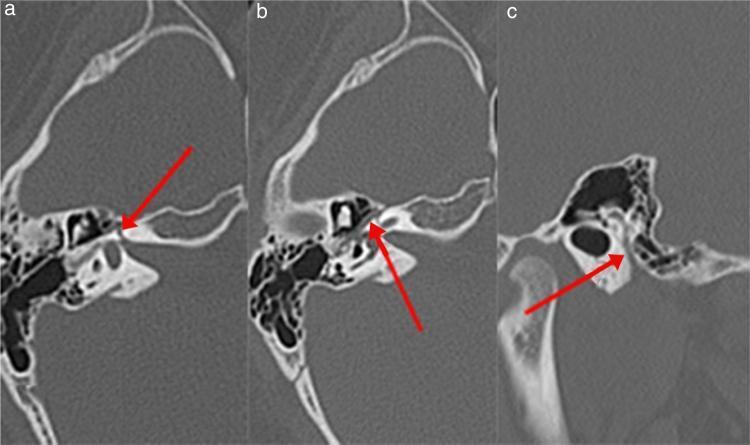
Facial Nerve Anatomy — CT Temporal Bone
INCIDENCE & EPIDEMIOLOGY
- Incidence: 20–30 per 100,000 per year (Harrison's, 21st ed.)
- Most common cause of acute unilateral facial palsy (60–75% of all cases)
- Peak age: 15–45 years; no sex predilection
- Increased risk: Pregnancy (especially 3rd trimester), diabetes mellitus, hypertension
- Recurrence: ~10–15% of cases
- Bilateral involvement: rare (<1%)
ETIOLOGY & PATHOPHYSIOLOGY
Etiology
(Harrison's Principles; Dhingra; Zakir Hussain ENT)
- Viral reactivation — Most accepted theory:
- Herpes Simplex Virus type 1 (HSV-1): Found in endoneurial fluid and posterior auricular muscle — primary etiology in majority (Harrison's, p. 12502)
- Varicella Zoster Virus (VZV): Second most common — implicated in up to one-third of cases
- Other viruses: EBV, CMV, mumps, rubella, HIV (Bell's palsy can occur during HIV seroconversion)
- Ischemic/vascular theory — Microvascular ischemia of the vasa nervorum
- Autoimmune — Post-viral immune-mediated demyelination
- Hereditary predisposition — Narrow Fallopian canal (anatomical predisposition)
Pathophysiology
HSV-1 Reactivation in Geniculate Ganglion
↓
Perineural inflammation + Mononuclear cell infiltration
↓
Edema of facial nerve within bony Fallopian canal
↓
Compression (most critical at LABYRINTHINE SEGMENT)
↓
Nerve ischemia → Demyelination
↓
Conduction block (Neuropraxia) or Axonotmesis
↓
Loss of facial motor, sensory & autonomic functions
Sunderland's Classification Applied to Bell's Palsy
| Grade | Type | Histology | Recovery |
|---|---|---|---|
| I | Neuropraxia | Conduction block, intact axon | Complete, weeks |
| II | Axonotmesis | Axon disrupted, endoneurium intact | Good, months |
| III | Axonotmesis++ | Axon + endoneurium disrupted | Partial |
| IV | — | Only perineurium intact | Poor |
| V | Neurotmesis | Complete transection | No recovery |
In Bell's palsy, grade I (neuropraxia) is most common, explaining the excellent recovery in 85% of cases.
CLINICAL FEATURES
(Scott-Brown's; Cummings; Hazarika; Dhingra)
Symptoms — Onset to Presentation
The onset is abrupt, with maximal weakness in 48–72 hours (Harrison's, p. 12501)
Prodromal symptoms (24–48 hrs before palsy):
- Postauricular / retroauricular pain — commonest first symptom
- Low-grade fever, malaise
Cardinal Features — "FACIAL PALSY" Mnemonic
| Feature | Mechanism | Branch/Level |
|---|---|---|
| Facial drooping — all ipsilateral muscles | Motor fiber involvement | All branches |
| Ability to close eye lost (Lagophthalmos) | Orbicularis oculi paralysis | Zygomatic branch |
| Corneal reflex loss | Afferent intact (V), efferent lost (VII) | Zygomatic branch |
| Inability to wrinkle forehead | Frontalis paralysis | Temporal branch |
| Alteration in taste (ageusia) | Chorda tympani involvement | Below geniculate ganglion |
| Lacrimation reduced | GSPN involvement (proximal lesion) | Above geniculate ganglion |
| Hyperacusis | Stapedius nerve involvement | Between geniculate & chorda tympani |
Upper vs Lower Motor Neuron Palsy (Critical RGUHS Distinction)
| Feature | UMN (Central) | LMN (Peripheral) — Bell's Palsy |
|---|---|---|
| Forehead spared? | Yes (bilateral cortical representation) | No — forehead involved |
| Cause | Stroke, tumor | Bell's palsy, parotid tumor, temporal bone fracture |
| Taste | Normal | Altered (if below geniculate) |
| Lacrimation | Normal | Reduced (if above geniculate) |
| Hyperacusis | Absent | Present (if above chorda tympani) |
Bell's Phenomenon
- On attempted eye closure, the eyeball rolls upward and outward — a protective reflex
- Visible because eye does not close (lagophthalmos)
- Indicates LMN lesion — pathognomonic sign (Dhingra; Hazarika)
Crocodile Tears (Gustatory Lacrimation)
- Aberrant regeneration of secretomotor fibers of chorda tympani into GSPN
- Patient cries while eating
- A late complication indicating misdirected regeneration
TOPOGRAPHIC DIAGNOSIS / LOCALIZATION OF LESION
(Stell & Maran; Scott-Brown; Cummings)
This is a favorite RGUHS topic — determines level of lesion by clinical tests:
┌─────────────────────────────────────────────────────────────────────┐
│ TOPOGRAPHIC LOCALIZATION OF FACIAL NERVE LESION │
│ │
│ Brainstem ──► Geniculate Ganglion ──► Stapedial Nerve ──► │
│ Chorda Tympani ──► Stylomastoid Foramen │
│ │
│ Tests used: │
│ 1. Lacrimation (Schirmer's test) — GSPN — Proximal to geniculate │
│ 2. Stapedial reflex — Nerve to stapedius │
│ 3. Taste (electrogustometry) — Chorda tympani │
│ 4. Submandibular salivary flow — Chorda tympani │
│ 5. Facial motor function — All levels │
└─────────────────────────────────────────────────────────────────────┘
Topographic Localization Table
| Site of Lesion | Lacrimation (Schirmer) | Stapedial Reflex | Taste | Salivation | Facial Paralysis |
|---|---|---|---|---|---|
| Brainstem / IAC | Abnormal | Abnormal | Abnormal | Abnormal | Yes |
| Geniculate ganglion | Abnormal | Abnormal | Abnormal | Abnormal | Yes |
| Between geniculate & stapedial | Normal | Abnormal | Abnormal | Abnormal | Yes |
| Between stapedial & chorda tympani | Normal | Normal | Abnormal | Abnormal | Yes |
| Below chorda tympani / stylomastoid | Normal | Normal | Normal | Normal | Yes |
GRADING SYSTEMS
1. House-Brackmann Grading System (MOST USED — Cummings, Scott-Brown)
| Grade | Description | Characteristics |
|---|---|---|
| I | Normal | Normal function all areas |
| II | Mild dysfunction | Slight weakness on close inspection; complete eye closure with effort |
| III | Moderate | Obvious difference; complete eye closure with effort; mouth moves but asymmetric |
| IV | Moderately severe | Obvious weakness; incomplete eye closure; asymmetric mouth |
| V | Severe | Barely perceptible motion; incomplete eye closure; slight mouth movement |
| VI | Total paralysis | No movement |
2. Sunnybrook Grading System (Newer, more sensitive)
3. Yanagihara 40-Point Scale (used in Japan / some Indian centers)
INVESTIGATIONS / DIAGNOSIS
Diagnosis
Bell's palsy is a diagnosis of exclusion (Cummings; Scott-Brown)
- No specific confirmatory test
- Exclude secondary causes first
Investigations
A. Electrodiagnostic Tests (Most important for prognosis)
| Test | Principle | Timing | Significance |
|---|---|---|---|
| Nerve Excitability Test (NET) | Stimulate nerve, compare thresholds | Early | Difference >3.5 mA = poor prognosis |
| Electroneuronography (ENoG / ENOG) | Compound muscle action potential | 3–14 days | Gold standard for prognosis; >90% degeneration = poor |
| Electromyography (EMG) | Detects fibrillation potentials | After 3 weeks | Fibrillations = denervation; polyphasic = reinnervation |
| Maximal Stimulation Test (MST) | Maximum current applied | 7–10 days | No response = poor prognosis |
ENoG (Electroneuronography): If amplitude drops >90% of the normal side within 14 days → surgical decompression considered (Cummings; Scott-Brown's)
B. Imaging
- MRI with gadolinium: Enhancement of geniculate ganglion and labyrinthine segment in Bell's palsy (not required routinely but helps exclude other causes)
- HRCT Temporal Bone: Evaluates bony canal (shown in image above); rules out cholesteatoma, temporal bone fracture
- Indications for MRI: Atypical features, no recovery by 6 months, recurrent palsy, suspicion of parotid/CNS lesion
C. Other Tests
- Schirmer's Lacrimation Test: Filter paper in conjunctival sac — <25 mm wetting in 5 minutes = abnormal; <30% of contralateral = significant
- Stapedial Reflex (Impedance audiometry)
- Electrogustometry — Taste testing anterior 2/3 tongue
- Blood investigations: FBS (rule out DM), HIV serology, Lyme serology (endemic areas), CBC
Flowchart: Diagnostic Approach to Bell's Palsy
ACUTE UNILATERAL FACIAL PALSY
│
┌──────────┴──────────┐
LMN Features UMN Features
(forehead involved) (forehead spared)
│ │
Full ENT Exam Neuroimaging (MRI)
+ Otoscopy → Stroke / Tumor
│
┌────┴────┐
Secondary Idiopathic
Causes? (Bell's Palsy)
│ │
Identify: Topographic Tests
- ASOM/CSOM + ENoG + EMG
- Ramsay Hunt │
- Parotid Tumor Mild (<90% Severe (>90%
- Fracture degeneration) degeneration)
- Tumor │ │
- Leukemia Medical Rx Consider Surgical
- Sarcoidosis Decompression
DIFFERENTIAL DIAGNOSIS
(Scott-Brown; Stell & Maran; Hazarika)
| Condition | Distinguishing Features |
|---|---|
| Ramsay Hunt Syndrome | Herpetic vesicles in EAC/pinna (herpes zoster oticus), pain more severe, worse prognosis |
| Acute Otitis Media | Fever, earache, pus in middle ear; otoscopy shows bulging/perforation |
| Cholesteatoma | Chronic ear discharge, attic retraction, conductive hearing loss |
| Parotid tumor | Parotid swelling, progressive palsy, FNAC/biopsy |
| Acoustic neuroma | SNHL, tinnitus, CPA syndrome, MRI confirms |
| Temporal bone fracture | History of trauma, hemotympanum, Battle's sign |
| Lyme disease | Tick exposure, erythema migrans rash, positive serology |
| Sarcoidosis (Heerfordt syndrome) | Uveitis, parotid enlargement, bilateral palsy |
| Melkersson-Rosenthal syndrome | Recurrent palsy, facial edema, fissured tongue (scrotal tongue) |
| Pontine lesions | Associated VI nerve palsy (lateral gaze palsy) — Millard-Gubler syndrome |
TREATMENT / MANAGEMENT
(Cummings; Scott-Brown; Dhingra; Hazarika; Zakir Hussain; Recent RGUHS Guidelines)
Goals of Treatment
- Hasten recovery of facial function
- Prevent corneal complications
- Prevent incomplete recovery and sequelae
Medical Management
1. Corticosteroids — First-line treatment
- Prednisolone 1 mg/kg/day (max 60 mg/day) × 10 days, then taper
- Must be started within 72 hours of onset for maximum benefit
- Mechanism: Reduces nerve edema and inflammation within bony canal
- Evidence: Sullivan et al. (NEJM 2007), Engström et al. (Lancet 2008) — steroids significantly improve recovery
- NNT = 10 (i.e., 1 in 10 patients benefit)
2. Antiviral Agents — Adjunctive (controversial)
- Acyclovir 400 mg 5×/day × 10 days OR Valacyclovir 1g TDS × 7 days
- Rationale: HSV-1 reactivation as etiology
- Current evidence: Antivirals alone NOT superior to placebo; steroids + antivirals may give marginal benefit over steroids alone (Engström et al., Lancet 2008)
- RGUHS standard: Combination of steroid + acyclovir recommended in moderate-severe palsy
Treatment Flowchart
CONFIRMED BELL'S PALSY
│
┌────────────┴────────────┐
Within 72 hours After 72 hours
│ │
Prednisolone 1 mg/kg × 10d Steroids still beneficial
+ Acyclovir/Valacyclovir (within 1 week)
│
┌───────┴────────┐
Eye Care Physiotherapy
(Lubricants, (Facial exercises,
Eye patch) massage)
│
Follow-up at 3 weeks
│
┌───────┴────────┐
Recovery No Recovery (>3 weeks)
(>80% grade I/II) │
│ ENoG/EMG
│ │
Continue >90% degeneration <90%
conservative within 14 days │
│ Continue
Surgical conservative
Decompression
(controversial)
3. Eye Care — Critical to prevent blindness
- Artificial tears (methylcellulose drops) — every 2 hours while awake
- Lubricating eye ointment — at night
- Moisture chamber / taping eyelid shut at night
- Tarsorrhaphy — temporary lateral tarsorrhaphy if lagophthalmos severe and prolonged
- Gold weight implant in upper lid — for permanent lagophthalmos
4. Physiotherapy
- Facial massage, active/passive exercises
- Electrostimulation — controversial; some benefit in preventing atrophy
- Mirror biofeedback therapy
- Start early to prevent muscle atrophy
Surgical Management
Surgical Decompression of Facial Nerve
Indications (Cummings; Scott-Brown):
- ENoG shows ≥90% degeneration within 14 days of onset
- EMG: absence of voluntary motor unit potentials (denervation)
- No recovery or worsening despite maximal medical therapy
- Must be performed within 14 days of onset for benefit (controversial after)
Surgical Approaches:
| Approach | Decompresses | Hearing Risk |
|---|---|---|
| Middle cranial fossa (MCF) | Labyrinthine segment + geniculate ganglion | Low (hearing preserved) |
| Transmastoid | Tympanic + mastoid segments | Low |
| Translabyrinthine | All segments | Deafness inevitable |
Middle cranial fossa approach is preferred when hearing is to be preserved and proximal decompression needed (Cummings, 7th ed.)
Note: The role of surgical decompression remains highly controversial. The 2013 AAO-HNS guidelines recommend AGAINST routine decompression and advise against it in the absence of robust evidence. Shared decision-making is recommended.
PROGNOSIS
(Hazarika; Dhingra; Harrison's)
Good Prognostic Factors
- Incomplete paralysis (House-Brackmann grade I–III)
- Early recovery (within 3 weeks)
- Young age
- No hyperacusis
- ENoG degeneration <90%
Poor Prognostic Factors
- Complete paralysis from onset
- Age >60 years
- Hypertension / Diabetes
- ENoG >90% degeneration in 14 days
- No recovery by 3 months
Recovery Statistics (Cummings; Scott-Brown)
- ~85% of patients recover completely without treatment
- With steroids: recovery improved to 94%
- 10–15% have residual weakness
- 5% have permanent severe dysfunction
Sequelae of Incomplete Recovery
- Synkinesis — Involuntary co-contraction (e.g., eye closure with smiling) due to misdirected regeneration
- Hemifacial spasm — Involuntary twitching of facial muscles
- Contracture — Tightening of paralyzed muscles
- Crocodile tears (Gustatory lacrimation) — Aberrant regeneration of GSPN fibers
- Corneal ulcer / Exposure keratitis — Due to lagophthalmos
- Psychosocial impact — Depression, social withdrawal
BELL'S PALSY IN SPECIAL SITUATIONS
Bell's Palsy in Pregnancy
- 3× more common in third trimester
- Managed with prednisolone (safe after first trimester)
- Antivirals: use with caution (Acyclovir generally considered safe)
- Prognosis similar to non-pregnant patients (Cummings)
Bell's Palsy in Children
- Generally excellent prognosis
- Full dose steroids may be used; adjust per weight
- EBV and Lyme disease must be excluded
Bilateral Bell's Palsy
- Rare (<1%) — always suspect Lyme disease, sarcoidosis, Guillain-Barré syndrome, leukemia, or HIV
RAMSAY HUNT SYNDROME vs BELL'S PALSY
| Feature | Bell's Palsy | Ramsay Hunt Syndrome |
|---|---|---|
| Etiology | HSV-1 reactivation | VZV reactivation |
| Vesicles | Absent | Present (EAC, pinna, palate) |
| Pain | Mild retroauricular | Severe |
| Hearing loss | Usually absent | Common (SNHL) |
| Vertigo | Absent | Present (vestibulocochlear involvement) |
| Prognosis | Better (~85% full recovery) | Worse (~50% full recovery) |
| Treatment | Steroids ± Acyclovir | Steroids + Acyclovir mandatory |
RECENT ADVANCES
(From recent literature — 2018–2024)
1. Viral Etiology — Molecular Evidence
- Murakami et al. confirmed HSV-1 DNA in endoneural fluid of Bell's palsy patients undergoing decompression — establishing viral basis beyond doubt
- Next-generation sequencing studies support HSV-1 > VZV in classic Bell's palsy
2. Medical Management Updates
- 2019 Cochrane Review (Gagyor et al.): Corticosteroids significantly improve recovery; combination antiviral + steroid shows marginal benefit — steroids alone remain first-line
- Valacyclovir preferred over acyclovir for better bioavailability
- High-dose Methylprednisolone IV: Used in severe complete palsy (grade VI) in some centers
3. Surgical Decompression — Evolving Evidence
- AAO-HNS 2013 Clinical Practice Guidelines: Decompression should NOT be routinely offered; insufficient evidence
- Recent meta-analyses (2020–2022) continue to show no definitive survival benefit of decompression over medical therapy
- Middle cranial fossa decompression within 14 days: some studies show benefit in ENoG-selected patients
4. Imaging Advances
- 3T MRI with gadolinium: Superior to 1.5T for detecting geniculate ganglion enhancement
- Diffusion tensor imaging (DTI): Newer technique to assess nerve fiber integrity — predicts prognosis more accurately
- High-resolution MRI distinguishes Bell's palsy from perineural tumor spread
5. Neuromodulation & Rehabilitation
- Electromyographic biofeedback (EMG-BF): Level I evidence for reducing synkinesis
- Botulinum toxin (Botox): For treatment of synkinesis and hemifacial spasm post-recovery
- Transcranial Magnetic Stimulation (TMS): Experimental — may enhance cortical reorganization and recovery
6. Genetic Predisposition
- Recent studies identify HLA type associations and narrow Fallopian canal variants as predisposing factors — may explain familial Bell's palsy
7. COVID-19 and Facial Palsy
- Bell's palsy reported as rare complication of COVID-19 infection and mRNA COVID-19 vaccines (Pfizer-BioNTech, Moderna)
- Large studies confirm no significant increased risk with vaccination vs. infection itself
- Managed with standard Bell's palsy protocol
8. Telemedicine Assessment
- eFACE digital grading and AI-based facial motion analysis: Objective tools for tracking recovery, reducing examiner bias
SUMMARY FLOWCHART: Bell's Palsy — At a Glance
┌────────────────────────────────────────────────────────────────┐
│ BELL'S PALSY │
│ │
│ DEFINITION: Acute idiopathic LMN facial palsy │
│ │
│ ETIOLOGY │
│ HSV-1 (primary) → Geniculate ganglion reactivation │
│ VZV (secondary, 1/3 cases) │
│ │
│ PATHOPHYSIOLOGY │
│ Viral reactivation → Inflammation → Edema → Compression │
│ at labyrinthine segment (narrowest) → Ischemia → Demyelination│
│ │
│ CLINICAL │
│ Retroauricular pain → Facial palsy (48-72h) + Bell's │
│ phenomenon + Lagophthalmos ± Ageusia ± Hyperacusis │
│ │
│ DIAGNOSIS: Clinical (exclusion) + ENoG + EMG │
│ MRI if atypical / no recovery by 6 months │
│ │
│ GRADING: House-Brackmann I–VI │
│ │
│ TREATMENT │
│ Prednisolone 1mg/kg/d × 10d (within 72h) ← CORNERSTONE │
│ + Acyclovir/Valacyclovir (adjunctive) │
│ + Eye care (artificial tears, taping, tarsorrhaphy) │
│ + Physiotherapy │
│ Surgery: MCF decompression if ENoG >90% (within 14d) │
│ │
│ PROGNOSIS │
│ 85% full recovery; 10-15% residual; 5% permanent │
└────────────────────────────────────────────────────────────────┘
REFERENCES FOR RGUHS
- Dhingra PL, Dhingra S — Diseases of Ear, Nose and Throat, 7th Edition; Chapter on Facial Nerve
- Hazarika P — Textbook of ENT & Head-Neck Surgery, 4th Edition
- Zakir Hussain — ENT Textbook for Undergraduates (Indian Standard Reference)
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery — 8th Edition, Vol 3 (Temporal Bone)
- Cummings Otolaryngology — Head & Neck Surgery, 7th Edition; Chapter 136 (Facial Nerve)
- Stell & Maran's Head and Neck Surgery — Facial Nerve Chapter
- Harrison's Principles of Internal Medicine, 21st Edition, p. 12501–12502
- Sullivan FM et al. — Early treatment with prednisolone or acyclovir in Bell's palsy. NEJM 2007; 357:1598–1607
- Engström M et al. — Prednisolone and valaciclovir in Bell's palsy. Lancet Neurol 2008; 7:993–1000
- Gagyor I et al. — Antiviral treatment for Bell's palsy. Cochrane Database 2019
- AAO-HNS Clinical Practice Guideline — Bell's Palsy, Otolaryngol Head Neck Surg, 2013
Exam Tip (RGUHS): For a 50-mark answer, always include: definition, anatomy (table of segments), pathophysiology flowchart, UMN vs LMN table, House-Brackmann grading, topographic localization table, treatment protocol, ENoG criteria for surgery, and at least 2 recent advances (COVID-19 association + Cochrane 2019 steroids). Bell's phenomenon and crocodile tears must be mentioned with mechanisms.
This is a shared conversation. Sign in to Orris to start your own chat.