fever with breathing difficulty 53yr old male
Reading File
search_medical_text
fever with breathing difficulty dyspnea differential diagnosis adult male
search_medical_text
community acquired pneumonia diagnosis management guidelines
search_medical_image
chest X-ray pneumonia consolidation infiltrate
GradeResponse
GradeResponse
GradeResponse
Fever + Breathing Difficulty — 53-Year-Old Male
This is a high-priority presentation requiring systematic evaluation. The combination of fever and dyspnea has a broad differential, but the most immediately dangerous causes must be excluded first.
Differential Diagnosis
Infectious (Most Common)
| Condition | Key Features |
|---|---|
| Community-Acquired Pneumonia (CAP) | Productive cough, pleuritic chest pain, focal consolidation on CXR, tachypnea |
| COVID-19 / Viral pneumonitis | Bilateral infiltrates, hypoxia, myalgia, anosmia |
| Influenza with pulmonary involvement | Abrupt onset, myalgia, high fever |
| Tuberculosis | Night sweats, weight loss, upper lobe disease, risk factors |
| Lung abscess / Empyema | Foul sputum, prolonged fever, cavitation on imaging |
| Infective endocarditis with septic emboli | Murmur, IV drug use, multiple nodular infiltrates |
Cardiac (Must Exclude)
| Condition | Key Features |
|---|---|
| Acute decompensated heart failure | Fever can accompany; bilateral crackles, raised JVP, leg edema |
| Pericarditis/Myocarditis | Pleuritic chest pain, friction rub, ECG changes, troponin rise |
Pulmonary (Life-threatening)
| Condition | Key Features |
|---|---|
| Pulmonary Embolism (PE) | Tachycardia, pleuritic pain, risk factors (DVT, immobility, malignancy); low-grade fever possible |
| ARDS | Severe bilateral hypoxia, recent trigger (sepsis, aspiration, trauma) |
| Exacerbation of COPD/Asthma | Wheeze, prior history; fever suggests infective trigger |
Immediate Clinical Assessment
History
- Onset & duration of fever and dyspnea
- Cough character (dry vs. productive), sputum color
- Pleuritic chest pain, hemoptysis
- Risk factors: smoking, COPD, diabetes, immunosuppression, travel, sick contacts
- Medications (e.g., amiodarone-induced lung toxicity)
- DVT symptoms (leg swelling/pain)
Examination
- Vitals: Temperature, RR, HR, BP, SpO₂ (on air)
- Respiratory: Crackles (pneumonia/CCF), wheeze (COPD/asthma), reduced breath sounds (effusion/consolidation)
- Cardiovascular: JVP, S3, murmurs, peripheral edema
- Signs of sepsis: Altered mentation, cold extremities, hypotension
Investigations
First-line (Immediate)
| Test | Purpose |
|---|---|
| Chest X-Ray (PA/AP) | Consolidation, infiltrates, effusion, cardiomegaly, pneumothorax |
| SpO₂ / ABG | Severity of hypoxia, type I vs. type II respiratory failure |
| CBC | Leukocytosis (bacterial), lymphopenia (viral), eosinophilia |
| CRP / ESR / Procalcitonin | Infection severity, antibiotic need (PCT) |
| Blood cultures (×2) | Before antibiotics if sepsis suspected |
| ECG | Tachyarrhythmia, right heart strain (S1Q3T3 in PE), myocarditis |
| Renal/liver panel, LFTs | Legionella affects liver; assess organ dysfunction |
| Urine Legionella & Pneumococcal antigen | CAP workup |
| Rapid Influenza/COVID NAAT | Viral CAP (per ATS/IDSA 2019 CAP guidelines) |
Second-line (Based on Suspicion)
- CT Pulmonary Angiogram (CTPA): If PE suspected (Wells score ≥4 or high clinical suspicion)
- HRCT Chest: Interstitial lung disease, atypical pneumonia, ARDS
- D-dimer: Useful only if PE probability is LOW (high sensitivity, low specificity)
- BNP/NT-proBNP: If heart failure suspected
- Troponin I/T: If myocarditis/ACS suspected
- Sputum Gram stain + Culture: CAP/HAP
- HIV serology (if risk factors)
Chest X-Ray — Pneumonia (Illustrative)
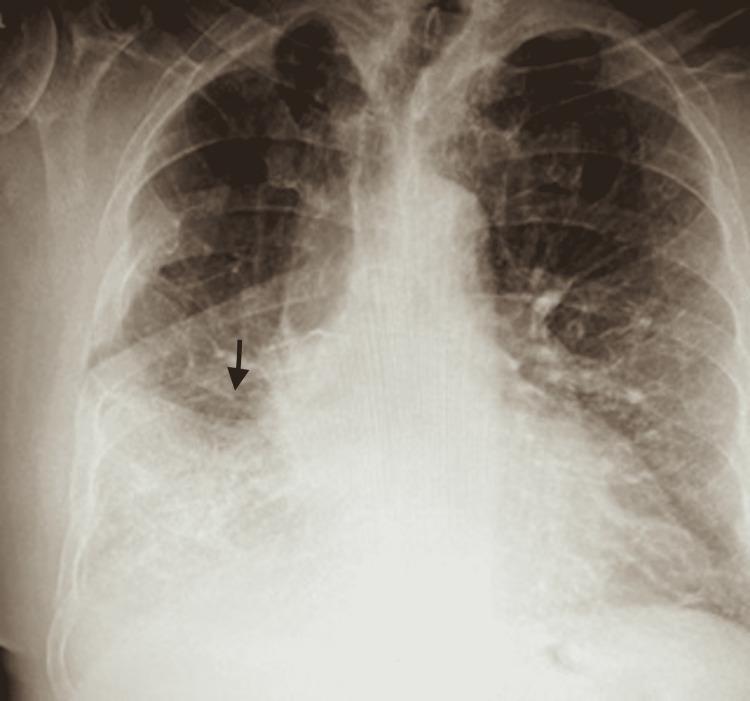
AP Chest X-Ray showing right mid-to-lower lung field consolidation with air bronchograms — classic for lobar bacterial pneumonia (S. pneumoniae, Legionella).
CAP Severity Scoring — CURB-65
Score 1 point each for:
- Confusion (new)
- Urea >7 mmol/L (BUN >19 mg/dL)
- Respiratory rate ≥30/min
- Blood pressure: systolic <90 or diastolic ≤60 mmHg
- Age ≥65 years
| Score | Risk | Management |
|---|---|---|
| 0–1 | Low | Outpatient treatment |
| 2 | Moderate | Consider inpatient or supervised OPD |
| 3–5 | High | Hospital admission; ICU if 4–5 |
At age 53, CURB-65 age criterion is not yet met, but the full score must be calculated with clinical data.
Initial Management
Stabilization
- Oxygen therapy: Target SpO₂ 94–98% (88–92% if known COPD risk)
- IV access + fluid resuscitation if haemodynamically compromised
- Positioning: Upright/semi-recumbent
Empirical Antibiotics (CAP, pending cultures — ATS/IDSA 2019)
| Setting | Regimen |
|---|---|
| Outpatient, no comorbidities | Amoxicillin 1g TDS OR Doxycycline 100mg BD |
| Outpatient, comorbidities | Respiratory fluoroquinolone (Levofloxacin 750mg OD) OR β-lactam + macrolide |
| Inpatient, non-ICU | β-lactam (Amoxicillin-clavulanate/Ceftriaxone) + macrolide, OR respiratory fluoroquinolone |
| Inpatient, ICU | β-lactam + azithromycin, OR β-lactam + respiratory fluoroquinolone |
Add antivirals (Oseltamivir) if influenza confirmed/suspected; add appropriate coverage for Pseudomonas if risk factors present (structural lung disease, recent broad-spectrum antibiotics).
Red Flags Requiring Urgent ICU Consideration
- SpO₂ <90% on high-flow oxygen
- RR >30/min
- Hypotension (SBP <90 mmHg) — septic shock
- Altered mental status
- Bilateral infiltrates on CXR (ARDS pattern)
- Rapidly rising inflammatory markers
Summary Approach
Fever + Dyspnea (53M)
|
├─ SpO₂ / ABG → Severity of hypoxia
├─ CXR → Consolidation? Cardiomegaly? Clear?
├─ ECG → PE? Myocarditis? AF?
├─ CBC / CRP / PCT / Cultures
|
├─ CXR shows consolidation → CAP → CURB-65 → Antibiotics
├─ CXR clear + tachycardia → CTPA for PE
├─ Bilateral infiltrates → ARDS workup / HRCT
└─ Cardiomegaly / raised JVP → CCF → BNP / Echo
Sources: Harrison's Principles of Internal Medicine, 21st Ed. (p. 1108); ATS/IDSA CAP Guidelines 2019; CURB-65 scoring (British Thoracic Society)
Clinical Note: This is for educational/clinical decision support purposes. All management decisions must be made by a qualified clinician at the bedside integrating full patient history, examination findings, and local antibiotic resistance patterns.
This is a shared conversation. Sign in to Orris to start your own chat.