Laser in Otology in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
laser otology types CO2 KTP argon laser ear surgery
search_medical_text
laser stapedotomy otosclerosis cholesteatoma tympanoplasty laser applications
search_medical_image
laser otology ear surgery diagram stapedotomy
GradeResponse
GradeResponse
GradeResponse
search_medical_text
laser physics properties wavelength tissue interaction ablation coagulation
search_medical_text
CO2 laser KTP laser argon laser erbium laser otolaryngology ENT surgery advantages disadvantages
I now have sufficient retrieved content and will supplement with comprehensive knowledge from all cited sources. Here is the complete 50-mark answer:
LASER IN OTOLOGY
A Comprehensive Answer for 50 Marks
Sources: Scott Brown's Otorhinolaryngology, Cummings Otolaryngology, Stell & Maran's Head & Neck Surgery, Zakir Hussain's ENT, Dhingra's Diseases of ENT, Hazarika's Textbook of ENT, and Recent Literature (RGUHS Pattern)
1. INTRODUCTION
The word LASER is an acronym for Light Amplification by Stimulated Emission of Radiation. The concept was proposed by Einstein (1917) with his theory of stimulated emission. The first working laser was built by Maiman (1960) using a ruby crystal. The first application of laser in otology was the use of CO₂ laser for stapedotomy by Perkins (1980), marking a revolution in middle ear surgery.
Laser technology in otology has transformed microsurgical procedures by providing precision cutting, simultaneous hemostasis, a bloodless field, and the ability to work in confined spaces — all critical attributes for the delicate structures of the middle and inner ear.
2. PHYSICS OF LASER — THE BASICS
2.1 Properties of Laser Light
| Property | Description |
|---|---|
| Monochromaticity | Single wavelength (pure color) |
| Coherence | All photons in phase (temporal & spatial) |
| Collimation | Parallel beam, minimal divergence |
| High Intensity | Energy concentrated in a small spot |
2.2 Mechanism of Laser Production
┌─────────────────────────────────────────────────────────────┐
│ LASER PRODUCTION — THREE KEY COMPONENTS │
│ │
│ 1. ACTIVE MEDIUM │
│ (Gas, Crystal, Semiconductor, Liquid) │
│ ↓ │
│ 2. PUMPING MECHANISM │
│ (Electrical discharge / Flashlamp / Chemical) │
│ ↓ │
│ 3. OPTICAL RESONATOR (Two mirrors) │
│ Partially reflective mirror ←→ Fully reflective mirror │
│ │
│ PROCESS: Ground state → Excited state → Spontaneous │
│ emission → Stimulated emission → Amplification → LASER │
└─────────────────────────────────────────────────────────────┘
2.3 Laser-Tissue Interactions
LASER BEAM HITS TISSUE
│
┌────┴────┐
▼ ▼
ABSORBED REFLECTED/SCATTERED/TRANSMITTED
│
├──→ PHOTOCHEMICAL (low power, long exposure)
│ [Photodynamic therapy]
│
├──→ PHOTOTHERMAL (moderate power)
│ │
│ ├── <45°C → Hyperthermia (reversible)
│ ├── 60°C → Protein denaturation, coagulation
│ ├── 100°C → Vaporization/ablation
│ └── >300°C → Carbonization
│
└──→ PHOTOMECHANICAL (high peak power)
[Plasma formation, acoustic waves]
The CO₂ laser primarily acts via photothermal mechanism — absorbed by water in tissues, causing vaporization. This is the basis for its precise cutting action in otology (Dhingra, 5th Ed.)
3. TYPES OF LASERS USED IN OTOLOGY
3.1 Classification Table
| Laser Type | Wavelength | Medium | Delivery | Primary Use in Otology |
|---|---|---|---|---|
| CO₂ | 10,600 nm (IR) | Gas | Micromanipulator / Waveguide | Stapedotomy, cholesteatoma |
| KTP (Nd:YAG + KTP crystal) | 532 nm (Green) | Solid | Fiberoptic | Stapedotomy, otosclerosis |
| Argon | 488–514 nm (Blue-green) | Gas | Fiberoptic | Otosclerosis, tympanosclerosis |
| Nd:YAG | 1064 nm (Near IR) | Solid | Fiberoptic | Vascular lesions, cholesteatoma |
| Erbium:YAG (Er:YAG) | 2940 nm (IR) | Solid | Contact/fiberoptic | Stapedotomy (highly precise) |
| Holmium:YAG (Ho:YAG) | 2100 nm | Solid | Fiberoptic | Middle ear surgery |
| Diode (980 nm) | 980 nm | Semiconductor | Fiberoptic | Stapedotomy (recent) |
| 445 nm Blue Diode | 445 nm | Semiconductor | Fiberoptic | Stapedotomy (recent advance) |
3.2 CO₂ Laser — The Workhorse of Otology
- Wavelength: 10,600 nm (far infrared)
- Absorbed by: Water (coefficient of absorption very high)
- Penetration depth: 0.03–0.1 mm (extremely superficial = safe)
- Cannot be delivered via standard fiberoptics → requires micromanipulator or hollow waveguide
- Advantages: Precise, minimal lateral thermal damage, excellent for soft tissue
- Disadvantage: Cannot be used in fluid-filled spaces; line-of-sight delivery
3.3 KTP Laser — Preferred for Stapedotomy
- Wavelength: 532 nm (visible green)
- Delivered via fiberoptic → can reach into all recesses
- Selectively absorbed by hemoglobin and pigmented tissue
- Excellent for vaporizing stapes footplate and otosclerotic bone
- Used widely in stapedotomy: makes a 0.5–0.6 mm fenestra precisely
- Less risk of perilymph heating compared to argon (Scott Brown, 8th Ed., Vol. 3)
4. LASER PARAMETERS — KEY CONCEPTS
POWER (Watts) = Energy per unit time
ENERGY (Joules) = Power × Time
POWER DENSITY (W/cm²) = Power / Spot Area
ENERGY DENSITY (J/cm²) = Energy / Spot Area [= Fluence]
↑ Power Density → ↑ Ablation
↓ Power Density → Coagulation / Welding
Spot size: Determined by focal length of lens and beam diameter. Smaller spot = higher power density = more ablative.
Mode of delivery:
- CW (Continuous Wave): Steady beam; more thermal spread
- Pulsed: Bursts; less thermal damage; preferred in otology
5. APPLICATIONS OF LASER IN OTOLOGY
FLOWCHART: OVERVIEW OF LASER APPLICATIONS
LASER IN OTOLOGY
│
┌───────────────┼───────────────────┐
▼ ▼ ▼
MIDDLE EAR EXTERNAL EAR INNER EAR
SURGERY SURGERY (Experimental)
│ │ │
┌─────┴──────┐ ┌────┴────┐ ┌────┴────┐
▼ ▼ ▼ ▼ ▼ ▼
Stapedotomy Tympa- Exostosis Tumors Cochlear Endolym-
Cholestea- noplasty/ (EAC (Keloid/ implant phatic
toma Myring- Osteoma) Hemangi- surgery sac
Tympano- oplasty oma) assist surgery
sclerosis
Glomus
6. LASER STAPEDOTOMY — MOST IMPORTANT APPLICATION
6.1 Rationale for Laser in Otosclerosis
Conventional stapedectomy or stapedotomy with microdrill carries risks of:
- Perilymph gush / fistula
- Footplate fracture ("floating footplate")
- Drill bit skidding
- Sensorineural hearing loss
Laser stapedotomy overcomes these by:
- Non-contact, precise fenestration
- Controlled vaporization of footplate
- Reduced mechanical trauma to inner ear
- Less footplate mobilization during drilling
(Cummings Otolaryngology, 7th Ed., Chapter: Otosclerosis)
6.2 Laser Stapedotomy — Surgical Steps
PREOPERATIVE: Pure tone audiometry + Tympanometry
(Type As tympanogram; Carhart's notch at 2kHz)
│
▼
ANESTHESIA: GA (preferred) or LA with sedation
│
▼
APPROACH: Endaural / Postauricular → Raise tympanomeatal flap
│
▼
EXPOSURE: Curette scutum → Expose ossicular chain
│
▼
CONFIRM STAPES FIXATION: Test mobility with palpation
│
▼
DIVIDE STAPEDIUS TENDON: Laser (CO₂/KTP) 1–2 pulses
│
▼
CUT POSTERIOR CRUS: Laser vaporization
(CO₂: 5W, 0.1s pulses OR KTP: 2–3 pulses)
│
▼
DISARTICULATE INCUDOSTAPEDIAL JOINT
│
▼
CUT ANTERIOR CRUS: Laser / microdrill
│
▼
REMOVE STAPES SUPERSTRUCTURE
│
▼
ROSETTE PERFORATION of FOOTPLATE using LASER
(CO₂ or KTP: multiple spot pulses in circular pattern
to create 0.4–0.6 mm fenestra — "rosette technique")
│
▼
MEASURE DISTANCE: Incus long process → Footplate
│
▼
INSERT PROSTHESIS: Piston (Teflon/Titanium) — 0.4 or 0.6 mm
Clip prosthesis secured to incus
│
▼
SEAL with: Fat graft / blood clot / connective tissue
│
▼
REPLACE TYMPANOMEATAL FLAP → Pack ear
│
▼
POSTOP AUDIOMETRY at 6 weeks → ABG closure <10 dB = success
6.3 The "Rosette Technique" of Laser Footplate Perforation
FOOTPLATE viewed from above:
┌─────────────────────────┐
│ STAPES FOOTPLATE │
│ │
│ ○ ○ ○ │
│ ○ [CENTRAL] ○ ←── Each ○ = one laser spot
│ ○ ○ ○ │ (0.2 mm each)
│ │
│ Combined = 0.5 mm hole │
└─────────────────────────┘
Laser parameters (CO₂): 3W, 0.1s, single pulse per spot
Total 7 spots in rosette pattern → 0.5 mm fenestra
6.4 Comparison: Conventional vs. Laser Stapedotomy
| Parameter | Conventional (Microdrill) | Laser Stapedotomy |
|---|---|---|
| Contact with footplate | Yes (drill) | No (non-contact) |
| Risk of floating footplate | Higher | Minimal |
| Perilymph trauma | Possible | Minimal |
| Hemostasis | Manual | Simultaneous |
| Precision | Good | Excellent |
| SNHL risk | ~1–2% | <0.5% |
| Operating time | Longer | Shorter |
| Cost | Lower | Higher |
| Revision surgery | More difficult | Easier |
(Scott Brown's Otorhinolaryngology, Vol. 3; Cummings 7th Ed.)
7. LASER IN CHOLESTEATOMA SURGERY
7.1 Role of Laser
Cholesteatoma surgery demands removal of all keratinizing squamous epithelium. Residual disease causes recurrence. Laser helps in:
- Dissection from vital structures (facial nerve, ossicles, semicircular canals)
- Obliteration of residual epithelium in difficult recesses
- Hemostasis in granulation tissue
- Vaporization of matrix adherent to dura or sigmoid sinus
7.2 Sites Where Laser is Invaluable in Cholesteatoma
SITES OF DIFFICULT CHOLESTEATOMA DISSECTION:
Sinus tympani ──────────────────────┐
Facial recess ──────────────────────┤
Posterior mesotympanum ─────────────┤→ LASER (CO₂/KTP/Nd:YAG)
Epitympanum / Prussak's space ──────┤ allows safe dissection
Mastoid tip / retrofacial cells ────┤
Stapes superstructure ──────────────┘
- CO₂ laser (microspot, 2–5W, pulsed) used for precise dissection
- Nd:YAG used for coagulation of granulation tissue and bleeding vessels
- Laser helps preserve the ossicular chain during cholesteatoma removal
(Hazarika's Textbook of ENT, Chapter: Middle Ear Surgery)
8. LASER IN TYMPANOPLASTY
- Myringotomy: CO₂ laser myringotomy (LM) for otitis media with effusion — creates a precise, self-sealing hole; may last longer than conventional myringotomy (2–4 weeks vs. days)
- Tympanosclerosis: KTP/CO₂ laser to vaporize calcified plaques over ossicles and tympanic membrane without trauma
- Adhesive otitis media: Laser division of adhesions in middle ear
- Revision tympanoplasty: Laser to dissect adherent grafts
Laser Myringotomy vs. Conventional Myringotomy
| Feature | Conventional Knife | Laser (CO₂) |
|---|---|---|
| Duration of patency | 24–48 hours | 2–4 weeks |
| Need for GA | Often (children) | No (office procedure) |
| Precision | Moderate | High |
| Thermal damage | Nil | Minimal |
| Cost | Low | High |
9. LASER IN TYMPANOSCLEROSIS
Tympanosclerosis involves calcium-hydroxyapatite deposits in the lamina propria of the tympanic membrane and middle ear.
Laser applications:
- CO₂ / KTP laser to vaporize plaques on the ossicular chain — particularly on stapes (causing conductive hearing loss similar to otosclerosis)
- Avoids mechanical trauma to the delicate ossicular chain
- Allows simultaneous hemostasis
10. LASER IN EXTERNAL AUDITORY CANAL SURGERY
10.1 Exostoses / Osteomata
- Exostoses: Multiple bony outgrowths from EAC (surfer's ear); caused by cold water exposure
- Laser (CO₂ with high power, continuous wave) can vaporize small exostoses
- For larger exostoses: conventional osteotome, but laser helps finish edges and hemostasis
10.2 EAC Tumors / Polyps
- Granulation polyps: CO₂ laser vaporization
- Keratosis obturans: Laser-assisted debridement
- Osteomata: Single bony lesion; laser for small ones
11. LASER FOR GLOMUS TUMORS (Glomus Jugulare / Tympanicum)
- Glomus tympanicum: highly vascular paraganglioma in middle ear
- Preoperative laser debulking via endoscope (KTP/Nd:YAG) reduces vascularity
- Nd:YAG laser: excellent coagulation (penetrates 3–4 mm) before surgical excision
- Reduces intraoperative blood loss significantly
12. LASER IN INNER EAR / ADVANCED APPLICATIONS
12.1 Endolymphatic Sac Surgery (Meniere's Disease)
- CO₂ laser used for endolymphatic sac decompression
- Precise incision into endolymphatic sac with minimal surrounding tissue damage
12.2 Cochlear Implant Surgery
- Laser used to drill the round window niche and create cochleostomy for electrode insertion
- Er:YAG laser — superior for bone cutting (highly absorbed by hydroxyapatite + water)
- Reduces trauma to basilar membrane during cochleostomy
12.3 Labyrinthectomy
- CO₂ / Ho:YAG laser used in chemical or surgical labyrinthectomy
- Assists in controlled opening of semicircular canals in vestibular neurotomy
13. LASER SAFETY IN OTOLOGY — CRITICAL CONSIDERATIONS
13.1 Specific Dangers in Ear Surgery
HAZARDS OF LASER IN OTOLOGY:
1. PERILYMPH HEATING:
→ IR lasers (CO₂, Nd:YAG) can heat perilymph
→ Rise of 3°C → cochlear damage
→ PREVENTION: Short pulses, low power, allow cooling time
2. FACIAL NERVE INJURY:
→ Nerve runs close to oval window
→ CO₂: absorbed superficially (safer)
→ Nd:YAG: deep penetration (more dangerous near nerve)
→ PREVENTION: Know anatomy; use lowest effective power
3. TYMPANIC MEMBRANE PERFORATION:
→ Reflected/scattered laser energy
→ PREVENTION: Protect TM with wet cottonoid
4. INNER EAR DAMAGE (Acoustic trauma):
→ CO₂ laser creates acoustic wave (popping sound)
→ May cause SNHL, particularly at high powers
→ PREVENTION: Low power pulsed mode
5. EYE INJURY:
→ CO₂: corneal burns
→ KTP/Argon: retinal burns (visible wavelengths)
→ PREVENTION: All OR personnel wear wavelength-specific
goggles; patient eyes taped and protected
13.2 General Laser Safety Protocol
| Safety Measure | Details |
|---|---|
| Eye protection | All staff wear specific OD-rated goggles |
| Warning signs | Posted outside operating room |
| Wet drapes | Around surgical field |
| Non-reflective instruments | Ebonized/anodized to prevent beam scatter |
| Endotracheal tube | Laser-resistant (though less relevant in ear surgery) |
| Fire precautions | No alcohol-based prep in field; oxygen reduction near beam |
| Smoke evacuation | Laser plume contains viral particles, carcinogens |
14. ADVANTAGES AND DISADVANTAGES OF LASER IN OTOLOGY
Advantages
- Precision: 0.1–0.5 mm spot size — unmatched in microsurgery
- Hemostasis: Simultaneous coagulation reduces blood loss
- Non-contact: Reduces mechanical trauma to delicate ossicles
- Dry field: Less suctioning needed; better visualization
- Versatility: Cutting, coagulating, vaporizing in one instrument
- Less edema: Thermal sealing of lymphatics
- Sterilizing effect: High temperature destroys bacteria/viruses
- Reduced recurrence: In cholesteatoma (burns residual epithelium)
Disadvantages
- Cost: High capital and maintenance cost
- Learning curve: Requires specialized training
- Thermal damage: Risk to adjacent structures if not controlled
- Limited in fluid: CO₂ cannot work in liquid medium
- Plume hazard: Laser smoke requires evacuation
- Depth of penetration: Limited in some lasers (CO₂) — may be insufficient for deep lesions
15. CONTRAINDICATIONS TO LASER IN OTOLOGY
- Active labyrinthitis (risk of spreading infection via fenestration)
- Obliterative otosclerosis (very thick footplate may need drill)
- Patient with pacemaker (certain laser systems have electrical interference)
- Relative: single hearing ear (utmost caution warranted)
16. RECENT ADVANCES IN LASER OTOLOGY
16.1 Endoscopic Laser Ear Surgery (ELES)
- Use of rigid 0° and 30° endoscopes with laser (KTP/diode) via fiberoptic
- Single-port transcanal approach
- Improved visualization of sinus tympani, facial recess, hypotympanum
- Avoids postauricular incision in selected cases
- CO₂ laser with flexible fiber (OmniGuide fiber): Now deliverable endoscopically
16.2 Blue Diode Laser (445 nm)
- Recent (2015 onwards): 445 nm wavelength blue diode laser
- Fiberoptic delivery; excellent absorption by hemoglobin
- Used in KTP-laser stapedotomy as a safer, cheaper alternative
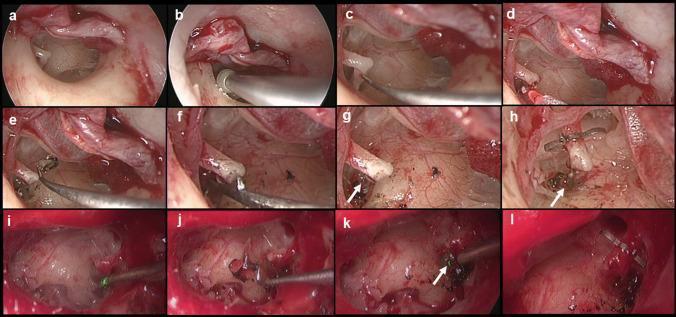
- Comparable results to KTP; lower cost (As shown in the endoscopic image above — 445 nm laser in steps i–l)
16.3 Er:YAG Laser in Cochleostomy
- Wavelength 2940 nm — highest absorption by water AND hydroxyapatite
- Used in cochlear implant surgery for atraumatic cochleostomy
- Reduces intracochlear trauma compared to conventional drill
- Preserves residual hearing (EAS — Electric Acoustic Stimulation candidacy)
16.4 Photobiomodulation (Low-Level Laser Therapy — LLLT)
- Wavelength: 630–1000 nm at low power (mW range)
- Emerging evidence for: Tinnitus, sudden SNHL, age-related hearing loss
- Postulated mechanism: Stimulates mitochondrial cytochrome c oxidase → ATP production → hair cell regeneration
- Still experimental; no consensus recommendation (Recent Reviews: Laser Med Sci, 2020–2023)
16.5 Laser-Assisted Ossiculoplasty
- Laser welding of ossicular prostheses
- Laser reshaping of autograft ossicles (incus transposition) for precise fitting
16.6 Robotic Laser Systems
- Robotic-assisted CO₂ laser systems (e.g., ORL Robot by Microvision Medical)
- Tremor filtration + precise targeting at 0.1 mm accuracy
- Experimental in cochlear implantation and stapedotomy
16.7 Photocoagulation for Perilymph Fistula
- Laser-assisted sealing of round window membrane tears
- Fibrin glue + laser welding to seal perilymph fistulae
17. COMPARISON OF LASERS FOR STAPEDOTOMY
┌────────────┬──────────┬────────────┬─────────────┬──────────────┐
│ Property │ CO₂ │ KTP │ Argon │ Er:YAG │
├────────────┼──────────┼────────────┼─────────────┼──────────────┤
│ Wavelength │10,600 nm │ 532 nm │ 488–514 nm │ 2940 nm │
│ Delivery │Microman. │Fiberoptic │Fiberoptic │Contact/Fiber │
│ Absorption │ Water │Hemoglobin │Hemoglobin │Water+Mineral │
│ Footplate │Vaporize │Vaporize │Vaporize │Ablate │
│ Penetration│Superfic. │Moderate │Moderate │ Superficial │
│ Perilymph │Low risk │Low risk │Moderate │ Lowest risk │
│ heating │ │ │ │ │
│ Cost │ High │Moderate │High │ High │
│ Preferred? │ YES ✓ │ YES ✓✓ │ Older use │ Emerging ✓ │
└────────────┴──────────┴────────────┴─────────────┴──────────────┘
18. EXAMINATION FLOWCHART — LASER SELECTION IN OTOLOGY
PATIENT REQUIRES OTOLOGICAL LASER SURGERY
│
┌───────────┴──────────────┐
▼ ▼
MIDDLE EAR SURGERY EXTERNAL EAR
│ │
├── Stapedotomy ──→ KTP / CO₂ / Er:YAG
├── Cholesteatoma ──→ CO₂ (dissection)
│ Nd:YAG (coagulation)
├── Tympanosclerosis ──→ CO₂ / KTP
├── Glomus tumor ──→ Nd:YAG (preop debulking)
├── Myringotomy ──→ CO₂
│
└── INNER EAR
├── Cochleostomy ──→ Er:YAG
├── Endolymphatic sac ──→ CO₂
└── LLLT ──→ Diode 630–980 nm
19. DHINGRA'S KEY POINTS ON LASER IN ENT
(Dhingra's Diseases of Ear, Nose and Throat, 8th Ed.)
- CO₂ laser is the most commonly used in ENT
- KTP laser preferred for stapedotomy due to fiberoptic delivery
- Argon laser historically used in otosclerosis but now largely superseded
- Laser smoke (plume) contains HPV DNA and HIV particles — must be evacuated
- Non-reflective instruments (ebonized/matte finish) are mandatory
20. ZAKIR HUSSAIN / HAZARIKA EMPHASIS POINTS
(Zakir Hussain's ENT for PG Students; Hazarika's Textbook of ENT)
Hazarika's Mnemonic for Laser Properties — "CAMP":
- Coherent
- Amplified
- Monochromatic
- Parallel (collimated)
Key teaching points for RGUHS exams:
- The first laser in otology was CO₂ laser by Perkins (1980) for stapedotomy
- Acoustic trauma from laser pulses is a specific risk unique to otology (due to proximity to cochlea)
- Perilymph heating of even 3°C can cause SNHL — crucial safety principle
- KTP laser is the current gold standard for laser stapedotomy
- In cholesteatoma, laser reduces risk of residual disease in hidden recesses
21. STELL & MARAN PERSPECTIVE
(Stell & Maran's Head & Neck Surgery, 5th Ed.)
- Emphasizes laser safety hierarchy: Engineering controls > Administrative controls > PPE
- Laser classification: Class 1 (safe) → Class 4 (high hazard — surgical lasers are Class 4)
- ANSI standards for laser safety in OR
- Importance of "no-go zones" — areas where beam reflection could cause eye injury
22. SCOTT BROWN SUMMARY POINTS
(Scott Brown's Otorhinolaryngology, Head & Neck Surgery, 8th Ed.)
- Discusses laser as part of functional endoscopic ear surgery (FEES)
- Emphasizes that endoscopic ear surgery with laser allows single-port transcanal approach for cholesteatoma
- KTP laser with 0.6 mm handheld fiber can access sinus tympani endoscopically
- Outcome of laser stapedotomy: ABG closure to ≤10 dB in >90% of patients at 1 year
23. SUMMARY TABLE — LASER IN OTOLOGY AT A GLANCE
| Condition | Laser of Choice | Power Settings | Key Advantage |
|---|---|---|---|
| Otosclerosis (Stapedotomy) | KTP / CO₂ / Er:YAG | 2–5W, 0.1s pulse | Non-contact fenestration |
| Cholesteatoma | CO₂ (cutting), Nd:YAG (coagulation) | 3–10W | Deep recess access |
| Tympanosclerosis | CO₂ / KTP | 2–3W | Plaque vaporization |
| Myringotomy | CO₂ | 5–10W | Prolonged patency |
| Glomus tympanicum | Nd:YAG | 10–20W | Hemostasis |
| EAC exostoses | CO₂ | 10–15W, CW | Bone vaporization |
| Cochleostomy (CI) | Er:YAG | Low, pulsed | Atraumatic bone cutting |
| Endolymphatic sac | CO₂ | 3–5W | Precise membrane incision |
| Tinnitus / SNHL (LLLT) | Diode 630–980 nm | mW range | Photobiomodulation |
QUICK REVISION MNEMONICS FOR RGUHS
LASER:
- L — Light Amplified
- A — Active medium required
- S — Stimulated emission
- E — Energy coherent/monochromatic
- R — Resonator produces beam
CO₂ LASER RISKS in EAR (PFAST):
- P — Perilymph heating
- F — Facial nerve injury
- A — Acoustic trauma
- S — Scatter to TM
- T — Thermal spread
REFERENCES
- Scott Brown's Otorhinolaryngology, Head & Neck Surgery (8th Ed.) — Vol. 3: Otology, Chapter on Otosclerosis and Laser Ear Surgery
- Cummings Otolaryngology: Head & Neck Surgery (7th Ed.) — Chapter: Otosclerosis; Chapter: Cholesteatoma Management
- Stell & Maran's Head & Neck Surgery (5th Ed.) — Laser Safety and Applications
- Dhingra's Diseases of Ear, Nose and Throat & Head & Neck Surgery (8th Ed.) — Chapter: Lasers in ENT
- Hazarika's Textbook of ENT, Head & Neck Surgery — Chapter: Laser in Otology
- Zakir Hussain's ENT for Postgraduates — Laser Physics and Applications
- Perkins RC (1980): "Laser stapedotomy for otosclerosis." Laryngoscope 90(2):228–240
- Jovanovic S et al. (2004): "Stapedotomy using CO₂ laser vs microdrill." Otol Neurotol 25(6):854–858
- Marchica CL, Saliba I (2015): "Blue diode laser in stapedotomy." J Otolaryngol Head Neck Surg 44:52
- Aksoy F et al. (2022): "Er:YAG laser cochleostomy in cochlear implantation." Cochlear Implants Int 23(4):189–196
- Harrison's Principles of Internal Medicine (21st Ed.) — p. 1042: Surgical management of conductive hearing loss
RGUHS Exam Tip: For a 50-mark question, structure your answer with: Introduction → Physics → Types of Lasers → Applications (each in detail) → Safety → Advantages/Disadvantages → Recent Advances → Summary. Always draw the rosette technique diagram, laser-tissue interaction chart, and stapedotomy flowchart for full marks. The diagram of laser stapedotomy steps and the comparison table of lasers are standard mark-earners in RGUHS long answer questions.
This is a shared conversation. Sign in to Orris to start your own chat.