Topical application for different skin conditions with images
Reading File
Finding Sources
Finding Sources
Searching the Web
topical applications for skin conditions dermatology overview 2025
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have sufficient information to compose a comprehensive, well-illustrated answer. Let me compile it:
Topical Applications for Different Skin Conditions
Topical therapy is the cornerstone of dermatology - delivering active agents directly to the target site while minimizing systemic exposure. Below is a condition-by-condition guide, with clinical images from Andrews' Diseases of the Skin and Dermatology 2-Volume Set 5e.
1. Acne Vulgaris
Clinical Picture
Acne lesions include comedones, papules, pustules, and nodules, distributed primarily across the face, chest, and back.
Topical Agents
| Severity | First-Line Topicals | Alternatives |
|---|---|---|
| Mild (comedones/few pustules) | Topical retinoid ± benzoyl peroxide (BPO) | Dapsone, clascoterone, azelaic acid |
| Moderate (papules/pustules) | Topical retinoid + BPO ± topical antibiotic | Dapsone, clascoterone |
| Severe (nodules) | Topical retinoid + BPO + oral antibiotic | Isotretinoin (oral) |
Key topical agents:
- Topical retinoids (tretinoin 0.025–0.05%, adapalene, tazarotene, trifarotene): Normalize follicular keratinization, reduce comedones, and have significant anti-inflammatory effects. Applied at night; require 8–12 weeks to judge efficacy. They also increase penetration of benzoyl peroxide and antibiotics into the sebaceous follicle.
- Benzoyl peroxide (BPO): Antibacterial (kills C. acnes), comedolytic, and prevents antibiotic resistance. Available as wash or leave-on formulation.
- Topical antibiotics (clindamycin, erythromycin): Reduce inflammatory lesions; always combined with BPO to prevent resistance.
- Azelaic acid: Anti-inflammatory and comedolytic; useful in patients with post-inflammatory hyperpigmentation.
- Clascoterone: Topical androgen receptor antagonist; reduces sebum production at the follicle level.
- Dapsone gel 5–7.5%: Anti-inflammatory; especially useful in adult female acne.
Critical rule: Topical application should cover the entire affected area, not just individual lesions. Long-term daily use is the norm.
(Dermatology 2-Volume Set 5e, Ch. 36; Andrews' Diseases of the Skin, Ch. 13)
2. Atopic Dermatitis (Eczema)
Clinical Images
Flexural atopic dermatitis (popliteal fossa involvement in childhood):

Fig. 5.2 - Flexural involvement in childhood atopic dermatitis. Note the erythema, lichenification, and excoriation at the popliteal fossae. (Andrews' Diseases of the Skin)
Severe widespread atopic dermatitis:

Fig. 5.3 - Severe, widespread atopic dermatitis with diffuse erythema and scaling. (Andrews' Diseases of the Skin)
Topical Agents
1. Topical Corticosteroids (TCS)
- The mainstay of acute flare management.
- Infants: Low-potency ointments (hydrocortisone 1–2.5%).
- Children/Adults: Medium-potency (triamcinolone, mometasone) for body; mild preparations or calcineurin inhibitors preferred for the face.
- Thick plaques: High-potency (clobetasol) used in short bursts of a few days.
- Ointments preferred over creams - better moisturizing effect, fewer preservatives (lower allergy risk).
- Maintenance: twice-weekly application to high-risk areas to prevent relapse; or 1 part hydrocortisone 2.5% ointment mixed with 1–4 parts emollient.
- Wet wraps/"soak and smear" technique increases efficacy in refractory cases.
2. Topical Calcineurin Inhibitors (TCIs)
- Tacrolimus ointment (0.03% for children, 0.1% for adults): Inhibits T-cell activation; steroid-sparing agent especially useful on the face, eyelids, and skin folds.
- Pimecrolimus cream 1%: More skin-selective than tacrolimus; preferred for mild to moderate disease.
- Patients may experience initial stinging/burning for the first few days.
- Systemic absorption is minimal with both agents.
- Require brief pretreatment with a potent topical corticosteroid (up to 1 week) to improve tolerability.
3. Emollients
- Applied liberally and frequently as the foundation of all AD management.
- Prevent trans-epidermal water loss, restore the skin barrier.
- Used before TCS/TCI ("soak and smear" method).
4. Newer topicals (2025 approvals)
- Delgocitinib cream (JAK inhibitor): FDA-approved for chronic hand eczema - the first steroid-free topical JAK inhibitor for this indication.
- Roflumilast 0.3% foam (PDE4 inhibitor): First topical foam approved for plaque psoriasis, with data emerging for AD as well.
(Andrews' Diseases of the Skin, Ch. 5; Dermatology 2-Volume Set 5e)
3. Psoriasis
Topical Agents
Psoriasis affects ~2% of the population and often requires lifetime management. Topical therapy is first-line for mild-to-moderate disease.
| Agent | Mechanism | Notes |
|---|---|---|
| Topical corticosteroids | Anti-inflammatory | Mainstay; combined with vitamin D analogues |
| Vitamin D3 analogues (calcipotriol/calcipotriene, calcitriol) | Inhibit keratinocyte proliferation, normalize differentiation | Combined formulation (calcipotriol + betamethasone) is highly effective |
| Topical retinoids (tazarotene) | Normalizes keratinocyte differentiation | More irritating than calcipotriol; used with TCS |
| Coal tar | Antiproliferative, anti-pruritic | Older agent; messy but still useful for scalp |
| Anthralin (dithranol) | Antiproliferative | Short-contact therapy; stains skin/clothes |
| Salicylic acid | Keratolytic | Used first to remove scale and enhance penetration of other agents |
| Tacrolimus/pimecrolimus | Anti-inflammatory | Useful for inverse/intertriginous psoriasis and facial psoriasis |
| Roflumilast 0.3% foam | PDE4 inhibitor | FDA-approved 2025 for scalp and body plaque psoriasis |
Scalp psoriasis: Requires shampoo-based or foam/solution formulations (coal tar shampoos, clobetasol solution, calcipotriol solution, roflumilast foam). The 308 nm excimer laser is effective for resistant lesions.
(Dermatology 2-Volume Set 5e, Ch. 30 & 71)
4. Rosacea
Topical Agents
Rosacea is managed differently based on subtype:
| Agent | Subtype | Mechanism |
|---|---|---|
| Metronidazole (0.75–1% gel/cream) | Papulopustular | Anti-inflammatory, antimicrobial |
| Azelaic acid (15–20% gel/cream) | Papulopustular | Anti-inflammatory, reduces erythema |
| Ivermectin 1% cream | Papulopustular | Kills Demodex mites, anti-inflammatory |
| Sodium sulfacetamide + sulfur | Papulopustular | Antibacterial, keratolytic |
| Brimonidine 0.33% gel | Erythematotelangiectatic | α2-adrenergic agonist - vasoconstriction lasting ~12 hours |
| Oxymetazoline 1% cream | Persistent facial erythema | α1A-adrenoreceptor agonist - reduces redness |
| Benzoyl peroxide | Phymatous (glandular) subset | Better tolerated than metronidazole in this subtype |
| Pimecrolimus/tacrolimus | Erythematotelangiectatic | Calms inflammation; caution - tacrolimus ointment may worsen glandular type |
(Andrews' Diseases of the Skin, Ch. Rosacea section)
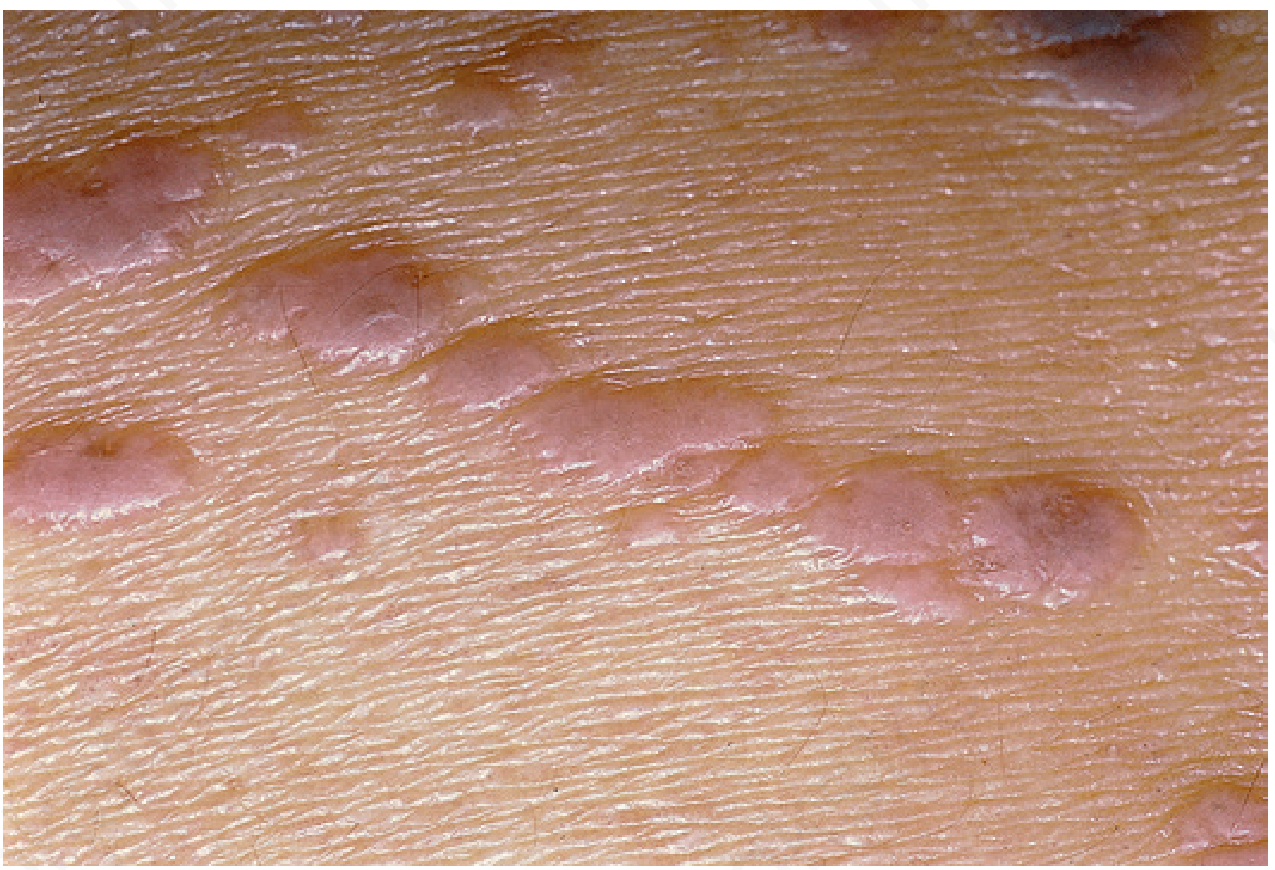
5. Superficial Basal Cell Carcinoma (BCC)

Fig. 29.20 - Multiple basal cell carcinomas in nevoid BCC syndrome. Raised, reddish-brown lesions of varying sizes on the back. (Andrews' Diseases of the Skin)
Topical Agents (for superficial BCC only)
| Agent | Protocol | Cure Rate |
|---|---|---|
| Imiquimod 5% cream | 5x/week × 6 weeks (without occlusion) or 3x/week × 6 weeks with occlusion | ~80% for superficial BCC |
| 5-Fluorouracil (5-FU) 5% cream | Twice daily × 6+ weeks | Acceptable in properly selected thin tumors; high recurrence |
| Photodynamic therapy (PDT) | Light-activated photosensitizer | Imiquimod is superior; 5-FU not inferior to PDT per RCT |
Nodular BCC has only ~65% cure rate with topical therapy - surgical excision is preferred for those cases.
(Andrews' Diseases of the Skin, Ch. 29)
6. Lichen Planus
eFig. 12.1 - Lichen planus. Violaceous, flat-topped papules with minimal scale. (Andrews' Diseases of the Skin)
Topical Agents
- Potent/superpotent topical corticosteroids (clobetasol, betamethasone dipropionate): First-line for localized cutaneous LP; applied once or twice daily.
- Topical calcineurin inhibitors (tacrolimus 0.1%, pimecrolimus 1%): Useful for oral LP, genital LP, and facial LP where steroids cause skin atrophy.
- Topical retinoids (tretinoin): Limited use; may help hypertrophic lesions.
- Intralesional corticosteroids (triamcinolone acetonide): For hypertrophic lesions unresponsive to topicals.
7. Summary Table: Topical Vehicle Choice
The formulation vehicle is as important as the active ingredient - it affects penetration, compliance, and tolerability.
| Vehicle | Best For | Notes |
|---|---|---|
| Ointment | Thick plaques, dry/lichenified skin, AD | Most occlusive, best penetration, no preservatives |
| Cream | General use, cosmetically acceptable | Easier to apply; may sting on inflamed skin |
| Gel | Scalp, acne, oily areas | High penetration; can be drying |
| Foam | Scalp, hairy areas | Good cosmetic acceptability (roflumilast foam for psoriasis) |
| Solution/lotion | Scalp, large areas | Easy spread; less occlusive |
| Shampoo | Scalp psoriasis/seborrhoeic dermatitis | Coal tar, ketoconazole, selenium sulfide |
Sources: Andrews' Diseases of the Skin: Clinical Dermatology | Dermatology 2-Volume Set 5e | Fitzpatrick's Dermatology | 2025 FDA dermatology drug approvals (delgocitinib cream for CHE; roflumilast 0.3% foam for psoriasis)
This is a shared conversation. Sign in to Orris to start your own chat.