Toxic amblyopia
Reading File
search_medical_text
toxic amblyopia etiology clinical features diagnosis
search_medical_text
toxic amblyopia treatment management nutritional optic neuropathy
GradeResponse
GradeResponse
The retrieved results are limited. I'll supplement with my own knowledge to deliver a thorough answer.
Toxic Amblyopia
Toxic amblyopia (also called toxic-nutritional optic neuropathy) is a bilateral, usually symmetric optic neuropathy caused by toxic or nutritional insults affecting the papillomacular bundle — the nerve fiber tract subserving central vision.
Etiology
Toxic and nutritional causes often coexist and are grouped together because they share identical clinical presentations and pathophysiology.
Toxic Causes
| Agent | Notes |
|---|---|
| Tobacco (tobacco-alcohol amblyopia) | Historically the most common; likely cyanide in tobacco smoke + B12 deficiency |
| Alcohol | Typically via nutritional deficiency rather than direct toxicity |
| Ethambutol | Dose-dependent; affects color vision first |
| Isoniazid | Via B6 (pyridoxine) deficiency |
| Chloramphenicol | Rare |
| Amiodarone | Can cause optic neuropathy |
| Methanol | Severe acute toxicity; damages retinal ganglion cells and optic nerve |
| Quinine | |
| Clioquinol | |
| Linezolid | Prolonged use |
| Phosphodiesterase-5 inhibitors | Rare |
Nutritional Causes
| Deficiency | Association |
|---|---|
| Vitamin B12 (cobalamin) | Most important; pernicious anemia, strict veganism, post-bariatric surgery |
| Vitamin B1 (thiamine) | Especially post-bariatric surgery, alcoholism (Harrison's, p. 12704) |
| Vitamin B2 (riboflavin) | |
| Folate | |
| Vitamin B6 (pyridoxine) | INH therapy |
| Protein-calorie malnutrition | "Tropical" or "Cuban" epidemic amblyopia |
Pathophysiology
The papillomacular bundle is selectively vulnerable because it contains small, thinly myelinated fibers with high metabolic demands. Toxins or nutritional deficiencies impair mitochondrial oxidative phosphorylation within these axons, leading to:
- Axonal degeneration of the papillomacular bundle
- Demyelination of the optic nerve (especially around the optic disc)
- In methanol poisoning: direct retinal ganglion cell toxicity (formic acid accumulation)
Clinical Features
Symptoms
- Bilateral, symmetric, painless, progressive visual loss (weeks to months)
- Central or cecocentral scotoma (connecting the blind spot to fixation) — the hallmark
- Dyschromatopsia (impaired color vision), often the earliest symptom
- Decreased contrast sensitivity
- Visual acuity typically 20/50–20/200 at presentation
Signs
- Normal or mildly hyperemic optic discs early on (unlike ischemic optic neuropathy)
- Temporal pallor of the optic disc develops late as nerve fiber loss progresses
- No afferent pupillary defect early (bilateral symmetric disease masks it)
- Fundus otherwise normal initially
Diagnosis
Clinical
- Bilateral symmetric central/cecocentral scotoma on visual field testing (Humphrey, Goldmann)
- Dyschromatopsia on Ishihara or Farnsworth-Munsell 100-hue testing
- Careful history: tobacco use, alcohol, medications, diet, bariatric surgery
Investigations
| Test | Purpose |
|---|---|
| Serum B12, folate, thiamine, B6 | Identify nutritional deficiency |
| MRI brain/orbits with gadolinium | Exclude compressive or inflammatory optic neuropathy |
| Optical coherence tomography (OCT) | Thinning of papillomacular bundle (temporal RNFL thinning) |
| Visual evoked potentials (VEP) | Prolonged latency, reduced amplitude |
| Blood methanol / formate levels | If methanol poisoning suspected |
| CBC, LFTs | Assess nutritional status and alcoholism |
The diagnosis of amblyopia requires identification of the likely cause; amblyopia without a clear etiology warrants careful workup for alternative diagnoses (Amblyopia, p. 17).
Key Differential Diagnoses
- Leber hereditary optic neuropathy (LHON) — mitochondrial genetics, typically young males
- Dominant optic atrophy — autosomal dominant, childhood onset
- Compressive optic neuropathy — MRI essential
- Demyelinating optic neuritis — typically painful, unilateral, younger patients
- Glaucoma — peripheral field loss, cupped disc
Management
Remove the Cause
- Stop the offending drug or toxin (e.g., ethambutol, linezolid, amiodarone)
- Abstain from tobacco and alcohol
- Address underlying malnutrition
Nutritional Supplementation
- Vitamin B12 (cyanocobalamin or hydroxocobalamin) — IM injections if absorption is impaired
- Thiamine — especially post-bariatric surgery; parenteral initially (Harrison's, p. 12704)
- Multivitamin B complex (B1, B2, B6, folate)
- High-protein, well-balanced diet
Prognosis
- Recovery is possible if treated early, before irreversible optic atrophy sets in
- The duration and severity of deficits before treatment are key predictors of outcome (Harrison's, p. 12704)
- Visual recovery may take weeks to months
- Temporal optic disc pallor and established optic atrophy generally indicate poor visual prognosis
Special Situations
Tobacco-Alcohol Amblyopia
Historically very common. The mechanism likely involves cyanide from tobacco inhibiting cytochrome oxidase in B12-deficient individuals. Treatment with hydroxocobalamin (which scavenges cyanide) and B-complex vitamins, combined with cessation of tobacco and alcohol, can produce recovery.
Methanol Poisoning
A distinct acute emergency. Formic acid (metabolite of methanol) directly poisons retinal ganglion cells and the optic nerve. Management includes:
- Fomepizole or ethanol (alcohol dehydrogenase inhibitors)
- Hemodialysis
- Folinic acid (to enhance formate metabolism)
- Corticosteroids (controversial, sometimes used for optic nerve inflammation)
Post-Bariatric Surgery
Rising incidence with increasing bariatric procedures. Copper deficiency, B12, and thiamine are the most implicated nutrients. Parenteral supplementation and reversal of the surgical bypass (if feasible) can improve outcomes (Harrison's, p. 12704).
Key Teaching Points
- Cecocentral scotoma + bilateral painless visual loss = toxic/nutritional optic neuropathy until proven otherwise
- Treat empirically with B-vitamins while awaiting workup — low risk, high reward
- Early treatment before optic atrophy is critical for visual recovery
Infantile esotropia for 30 marks
Reading File
search_medical_text
infantile esotropia definition clinical features characteristics
search_medical_text
infantile esotropia surgical treatment management amblyopia
search_medical_image
infantile esotropia
GradeResponse
GradeResponse
GradeResponse
Excellent results. I have strong source material plus my own knowledge base to deliver a thorough 30-mark answer.
Infantile Esotropia
Definition
Infantile esotropia (also called congenital esotropia) is a constant, convergent squint (inward deviation of one or both eyes) that presents within the first 6 months of life without spontaneous resolution (Esotropia and Exotropia, p. 10). The term "infantile" is preferred over "congenital" because the deviation is rarely present at birth but manifests in the first few months.
Epidemiology
- Most common form of strabismus in infants
- Incidence: ~1% of the general population
- More common in preterm infants and those with neurological impairment
- Familial predisposition (positive family history in ~20–30% of cases)
- Associated with cerebral palsy, hydrocephalus, Down syndrome
Etiology and Pathogenesis
The exact cause remains debated. Two major theories:
1. Motor Imbalance Theory (Worth)
Abnormal innervation or anatomical imbalance of extraocular muscles causes the deviation primarily. Sensory fusion is secondarily lost.
2. Sensory Fusion Defect Theory (Chavasse)
A primary defect in the cortical mechanism for binocular fusion leads to the deviation. This theory underpins the rationale for early surgery — to allow fusion to develop.
Contributing Factors
- Genetic: Autosomal dominant inheritance pattern in some families
- Neurological: High association with CNS abnormalities (up to 30% in some series)
- Accommodative element: Usually non-accommodative, though partial accommodative components can exist
Clinical Features
Core Characteristics (Esotropia and Exotropia, p. 10)
| Feature | Detail |
|---|---|
| Onset | Before 6 months of age |
| Angle of deviation | Large — typically ≥30–40 prism diopters (PD) |
| Constancy | Constant (not intermittent) |
| Laterality | Usually alternating; may be unilateral |
| Refractive error | Usually normal or mild hyperopia (not the cause) |
| Accommodation | Non-accommodative or partially accommodative |
| Progression | May increase over time |
Cross-Fixation
- A hallmark feature: the child uses the right eye to look left and the left eye to look right
- Each eye is used in adduction (turned in)
- This can mask amblyopia since both eyes are being used — though risk of amblyopia remains (Esotropia and Exotropia, p. 10)
Associated Features (may develop later)
| Feature | Description |
|---|---|
| Amblyopia | Present in ~50%; risk increases if fixation preference is strong |
| Dissociated Vertical Deviation (DVD) | Upward drift of one eye when not fixating; present in ~50–90% of cases; appears months to years after onset |
| Inferior Oblique Overaction (IOOA) | Upward and outward movement in adduction; develops in ~70% |
| Latent/Manifest Latent Nystagmus | Jerk nystagmus on monocular occlusion; fast phase toward the fixating eye |
| A or V patterns | Changes in horizontal deviation in upgaze/downgaze |
| OKN asymmetry | Monocular optokinetic nystagmus asymmetry (nasal > temporal) |
Clinical Image
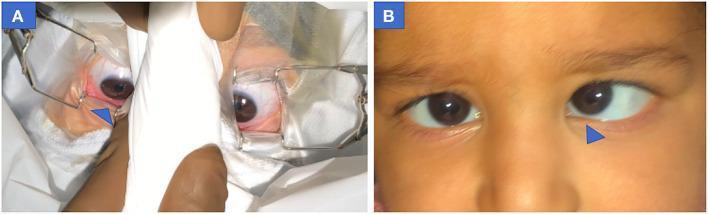
Pre-operative photograph showing infantile esotropia with dissociated vertical deviation (DVD) of the left eye (inward and upward deviation). Blue arrow highlights asymmetric alignment.
Diagnosis
History
- Age of onset, family history of strabismus, birth history (prematurity), developmental milestones, neurological symptoms
Examination
1. Visual Acuity Assessment
- Age-appropriate methods: preferential looking (Teller cards), Cardiff cards, or fixation behavior (central, steady, maintained — CSM)
- Assess fixation preference: unequal fixation indicates amblyopia
2. Cover Tests
- Cover-uncover test: reveals manifest deviation (tropia)
- Alternate cover test + prism neutralization (APCT): measures the total angle of deviation
- Krimsky test / Hirschberg test: useful in preverbal infants who cannot cooperate with prism cover test
3. Measurement of Deviation
- Prism and Alternate Cover Test (PACT): gold standard for measuring angle — measured at distance (6 m) and near (33 cm)
- Typical angle in infantile esotropia: ≥30 PD at distance
4. Cycloplegic Refraction
- Mandatory — with cyclopentolate 1% or atropine
- Identifies significant hyperopia (>+2.00 D) that may have accommodative component
- Spectacles prescribed first if significant refractive error found
5. Ocular Motility Assessment
- Assess ductions and versions in 9 cardinal positions
- Identify IOOA, superior oblique underaction, A/V patterns
6. Fundus Examination
- Rule out structural pathology (retinoblastoma, optic nerve hypoplasia, retinal dystrophy)
- Identify optic nerve pallor, macular abnormalities
7. Neuroimaging
- MRI brain if neurological signs, atypical features, or nystagmus suggesting CNS pathology
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Accommodative esotropia | Onset 2–3 years, significant hyperopia (+3 D or more), partially/fully corrected by glasses |
| Pseudoesotropia | Broad nasal bridge/epicanthic folds give appearance of squint; Hirschberg corneal reflex symmetric |
| Sixth nerve palsy | Unilateral, limited abduction, may have head turn |
| Duane retraction syndrome type 1 | Limited abduction, globe retraction and palpebral fissure narrowing on adduction |
| Nystagmus blockage syndrome | Esotropia associated with nystagmus that dampens in convergence |
Management
Management follows a sequential, stepwise approach:
Step 1: Correct Refractive Error
- Cycloplegic refraction performed
- Spectacles prescribed if hyperopia ≥ +2.00 D or significant astigmatism
- Re-examine after 6–8 weeks of spectacle wear — if deviation fully corrected, it is accommodative
Step 2: Treat Amblyopia
- Occlusion therapy (patching): patch the preferred (fixing) eye to stimulate the amblyopic eye
- Part-time patching (2–6 hours/day) depending on age and depth of amblyopia
- Pharmacological penalization: atropine drops to preferred eye (blurs near vision, forces use of amblyopic eye)
- Must treat amblyopia before surgery if possible, as amblyopia treatment alone will not correct the angle
Step 3: Surgical Correction
Surgery is indicated when glasses and amblyopia treatment fail to align the eyes (Esotropia and Exotropia, p. 18). Surgery is not performed for small deviations (<12 PD).
Timing of Surgery
- Ideal: before 2 years of age (some advocate before 12–18 months) to maximize potential for binocular vision development
- Sensory critical period: earlier correction improves prospects for bifoveal fusion and stereopsis
- Surgery delayed until amblyopia is controlled and angle is stable
Surgical Options
| Procedure | Indication |
|---|---|
| Bilateral medial rectus recession (BRC) | Most common; for large angle deviations ≥30–35 PD |
| Recession + resection (R&R) | Unilateral procedure: recession of medial rectus + resection of lateral rectus of same eye; for moderate angles |
| Inferior oblique weakening | Added if IOOA significant (recession, myectomy, or anteriorization) |
| Superior oblique tuck | For superior oblique underaction / A-pattern |
Surgical Goals
- Achieve orthotropia or small-angle residual esotropia (within 10 PD of straight)
- Surgical success defined as alignment within 8–10 PD of orthotropia
- Gross stereopsis (peripheral fusion) is realistic; fine stereopsis is usually not achieved if surgery is delayed
Botulinum Toxin (Botox)
- Chemodenervation of medial rectus as an alternative or adjunct to surgery
- More useful in acquired or small-angle esotropias
- Less predictable for large-angle infantile esotropia; not first-line
Step 4: Postoperative Management
- Continue amblyopia therapy postoperatively
- Monitor for DVD — may require subsequent surgery (inferior rectus recession or superior rectus posterior fixation / Faden procedure)
- Monitor for IOOA — inferior oblique recession/myectomy
- Regular follow-up for refractive changes and re-development of amblyopia
Prognosis and Outcomes
| Outcome | Expectation |
|---|---|
| Motor alignment | Achievable in ~70–80% with one surgery |
| Binocular vision | Peripheral fusion possible if corrected early; fine stereopsis rarely achieved |
| Amblyopia | Reversible if treated in critical period; may recur after surgery if fixation preference shifts |
| DVD/IOOA | Develops in majority; manageable with additional procedures |
| Second surgery | Required in ~30–40% (for residual/recurrent esotropia, DVD, or oblique overaction) |
Key Points Summary
- Infantile esotropia = constant esotropia presenting before 6 months without resolution
- Large angle (≥30 PD), cross-fixation, alternating — key hallmarks
- Non-accommodative; cycloplegic refraction essential to rule out accommodative component
- Amblyopia, DVD, and IOOA are major associated features
- Management is stepwise: refraction → amblyopia treatment → surgery
- Surgery before age 2 (bilateral medial rectus recession) optimizes sensory outcomes
- Fine stereopsis is rarely achieved; motor alignment and peripheral fusion are realistic goals
- Long-term follow-up mandatory for amblyopia recurrence, DVD, and IOOA
This is a shared conversation. Sign in to Orris to start your own chat.