Here are your complete exam notes - 15 marks for major topics and 5 marks for the short topics. Each is written to match the depth and breadth examiners expect.
🏥 GENERAL SURGERY - PHYSIOTHERAPY EXAM
COMPLETE NOTES | 15-MARK & 5-MARK FORMAT
═══════════════════════════════════════
PART A - MAJOR TOPICS (15 MARKS EACH)
═══════════════════════════════════════
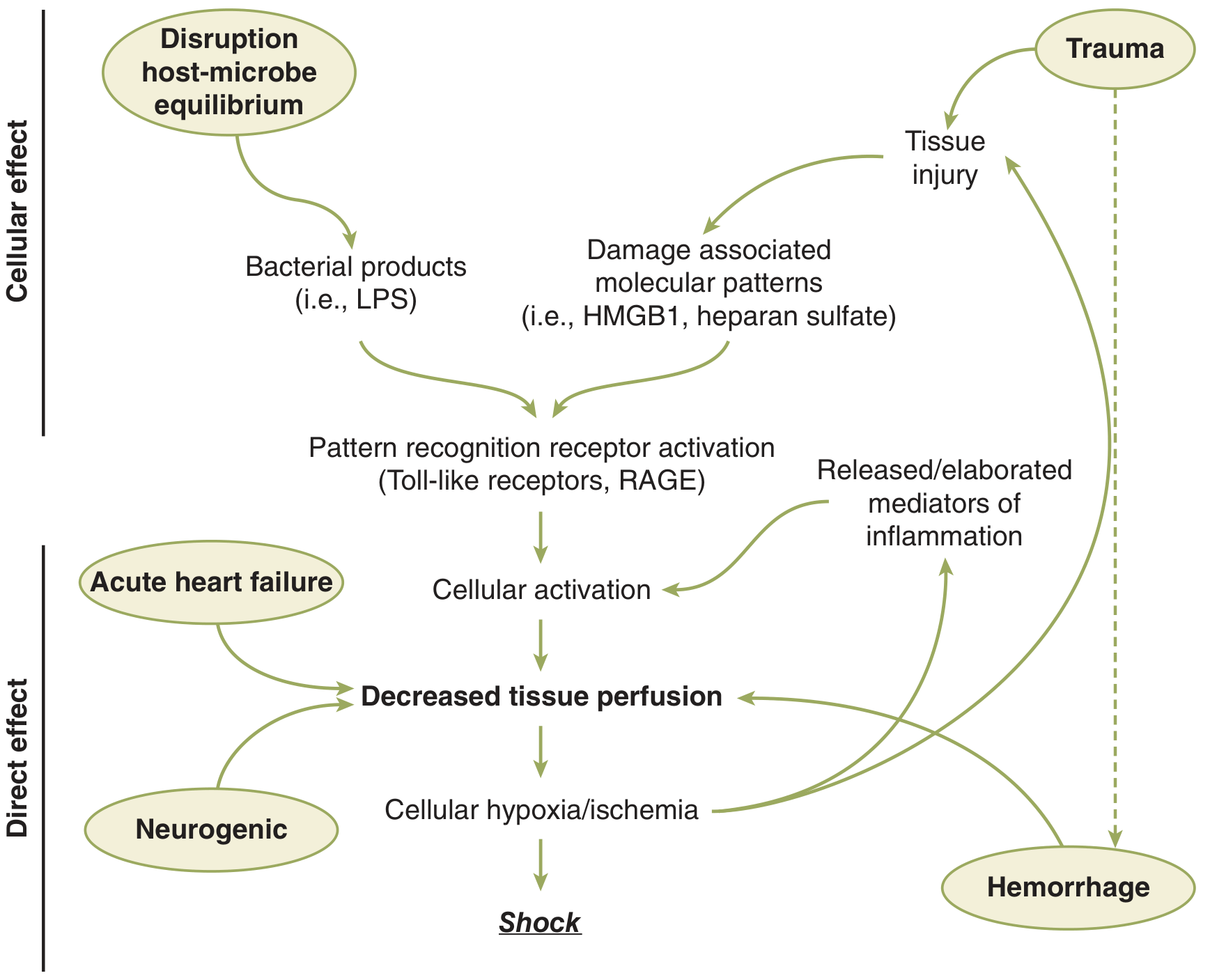
1. SHOCK (15 Marks)
Definition
Shock is the failure to meet the metabolic demands of cells and tissues due to inadequate tissue perfusion, leading to cellular hypoxia and organ dysfunction. (Schwartz's Principles of Surgery, 11th Ed.)
Classification
| Type | Primary Cause | Mechanism |
|---|
| Hypovolemic | Blood/fluid/plasma loss | Decreased preload → decreased CO |
| Hemorrhagic | Active bleeding (subset of hypovolemic) | Volume depletion |
| Septic (Vasodilatory) | Bacterial endotoxins (LPS) | Peripheral vasodilation, maldistribution |
| Cardiogenic | MI, arrhythmia, valve failure | Pump failure → decreased CO |
| Neurogenic | Spinal cord injury, spinal anaesthesia | Loss of sympathetic tone → vasodilation |
| Obstructive | Tension pneumothorax, massive PE, tamponade | Mechanical obstruction to flow |
| Traumatic | Combined hemorrhage + tissue injury | Hemorrhage + inflammatory mediator release |
Pathophysiology
Three Phases of Shock:
-
Compensated Phase: Body compensates via neuroendocrine response (catecholamines, ADH, RAAS activation) - tachycardia, vasoconstriction, fluid conservation. BP may be maintained.
-
Decompensated Phase: Compensation fails. Cellular hypoxia worsens. Anaerobic metabolism → lactic acidosis. Microcirculatory dysfunction. Organ dysfunction begins.
-
Irreversible Phase: Extensive parenchymal + microvascular injury. Volume resuscitation fails to reverse. MODS (Multi-Organ Dysfunction Syndrome) → death.
Cellular level:
- Reduced O₂ delivery → mitochondrial dysfunction
- Switch to anaerobic glycolysis → lactate production
- Cell membrane Na/K-ATPase fails → cellular edema
- Release of DAMPs (damage-associated molecular patterns) → systemic inflammation
ATLS Classification of Hemorrhagic Shock (4 Classes)
| Class | Blood Loss | Volume (70 kg adult) | HR | BP | Pulse Pressure | RR | Urine Output | Mental Status |
|---|
| I | <15% | <750 mL | <100 | Normal | Normal | 14-20 | >30 mL/hr | Normal |
| II | 15-30% | 750-1500 mL | 100-120 | Normal | Decreased | 20-30 | 20-30 mL/hr | Anxious |
| III | 30-40% | 1500-2000 mL | 120-140 | Decreased | Decreased | 30-40 | 5-15 mL/hr | Confused |
| IV | >40% | >2000 mL | >140 | Very low | Very low | >35 | Minimal | Lethargic/unconscious |
Clinical Features
Universal signs:
- Hypotension (SBP <90 mmHg)
- Tachycardia
- Oliguria (<0.5 mL/kg/hr)
- Altered consciousness
- Metabolic acidosis (lactic acidosis)
Specific to type:
- Septic shock: Initially warm, flushed skin (early distributive); then cold, clammy (late)
- Cardiogenic: Raised JVP, pulmonary edema, S3 gallop
- Neurogenic: Bradycardia + hypotension (paradox - no tachycardia due to loss of sympathetics)
- Obstructive (tamponade): Beck's triad; tension pneumothorax: absent breath sounds + tracheal deviation
Investigations
- Lactate (>2 mmol/L = hypoperfusion; >4 mmol/L = severe shock)
- ABG: metabolic acidosis, base deficit
- FBC: Hb, WBC, platelets
- Coagulation (PT, APTT) - coagulopathy in hemorrhagic
- Blood cultures (septic shock)
- ECG, troponin (cardiogenic)
- Echocardiography / bedside FAST
- Serum electrolytes, creatinine (organ function)
Management
General:
- Two large-bore IV cannulae (16G or larger)
- Oxygen supplementation
- Continuous monitoring: pulse, BP, SpO₂, urine output, ECG
- Treat the underlying cause
Hemorrhagic/Hypovolemic:
- Control hemorrhage - direct pressure, tourniquet, surgery
- Blood product resuscitation: PRBC, FFP, platelets (1:1:1 ratio in massive hemorrhage)
- Avoid "lethal triad": hypothermia + acidosis + coagulopathy
- Permissive hypotension: SBP 80-90 until hemorrhage controlled
- Tranexamic acid within 3 hours (CRASH-2 trial evidence)
Septic Shock (Surviving Sepsis Campaign):
- IV broad-spectrum antibiotics within 1 hour
- 30 mL/kg IV crystalloid within 3 hours
- Source control (drain pus, remove infected hardware, debridement)
- Vasopressors: Norepinephrine is first-line if fluid-unresponsive
- Target MAP ≥65 mmHg, urine output ≥0.5 mL/kg/hr
Cardiogenic:
- Inotropes: Dobutamine, milrinone
- Treat arrhythmias, reperfusion for MI (PCI)
- Do NOT give excessive IV fluids
Neurogenic:
- IV fluids (limited) + vasopressors (norepinephrine)
- Spinal immobilization
Physiotherapy Relevance in Shock Recovery
- Patients post-shock have prolonged ICU stays; early physiotherapy reduces muscle wasting
- Respiratory physiotherapy (suction, positioning, NIV weaning)
- Progressive mobilization once hemodynamically stable
- Management of complications: pressure sores, DVT prevention, ICU-acquired weakness
2. BURNS (15 Marks)
Definition
A burn is tissue injury caused by thermal, chemical, electrical, or radiation energy leading to protein denaturation, cell death, and inflammatory response.
Classification by Depth
| Degree | Layers Involved | Appearance | Sensation | Healing | Treatment |
|---|
| 1st degree (Superficial) | Epidermis only | Red, dry, no blisters | Painful | 7 days, no scar | Symptomatic, moisturizer |
| 2nd degree - Superficial partial | Epidermis + superficial dermis | Blisters, red, wet, shiny | Very painful | 14-21 days, minimal scar | Dressings, no surgery |
| 2nd degree - Deep partial | Epidermis + deep dermis | Pale/yellow, blisters, wet | Reduced pain | 3-8 weeks, scarring | May need skin graft |
| 3rd degree (Full thickness) | Full skin (epidermis + dermis) | Charred, leathery, waxy, pale | Painless (nerve destruction) | Months, severe scar | Skin graft mandatory |
| 4th degree | Skin + subcutaneous, muscle, bone | Charred, black, necrotic | Painless | Multiple surgeries | Flap/amputation |
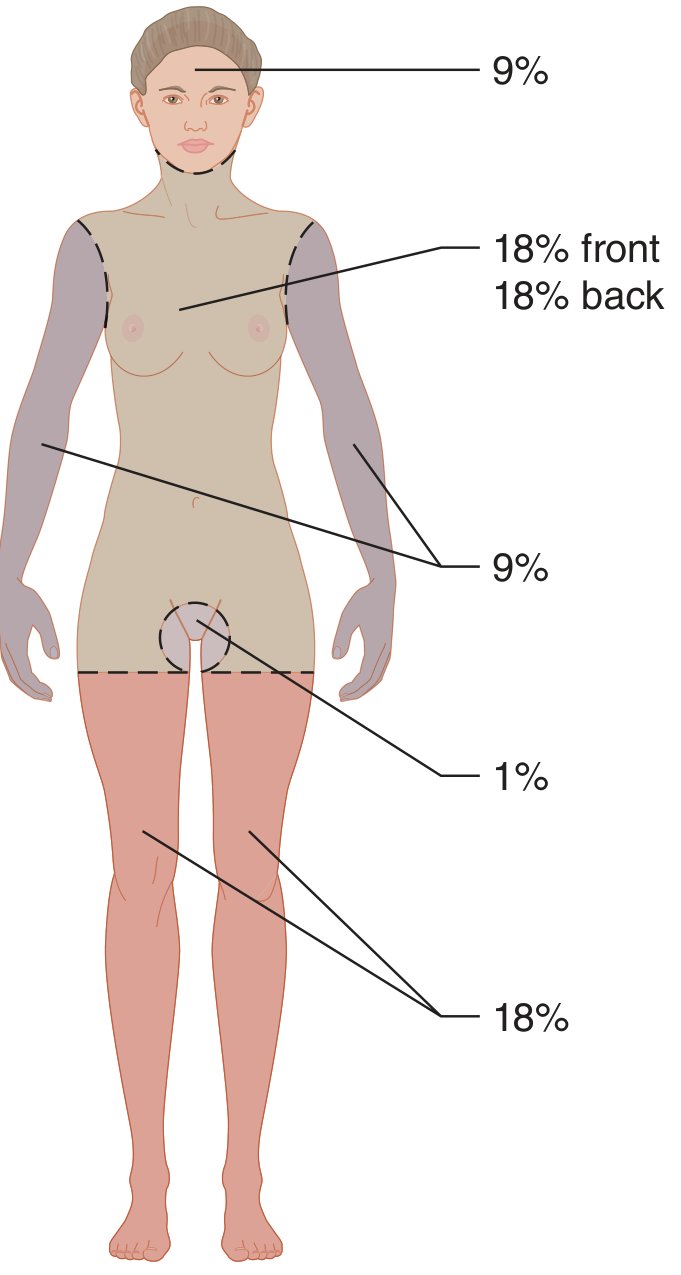
Estimation of Burn Surface Area
Rule of Nines (Wallace's Rule of Nines)
| Body Region | Adult BSA |
|---|
| Head + Neck | 9% |
| Each upper limb | 9% (arm 4%, forearm 3%, hand 2%) |
| Anterior trunk | 18% |
| Posterior trunk | 18% |
| Each lower limb | 18% (thigh 9%, leg 7%, foot 2%) |
| Perineum + genitalia | 1% |
Note: In children - head is larger (18%) and legs are smaller. Use Lund-Browder chart for accurate pediatric assessment.
Palm method: Patient's own palm = 1% BSA (useful for scattered burns)
Pathophysiology of Burns - Jackson's Zones
- Zone of Coagulation (central) - maximum damage, irreversible cell death
- Zone of Stasis (middle) - ischemic but potentially viable; management aim is to prevent conversion to zone of coagulation
- Zone of Hyperemia (periphery) - increased perfusion, full recovery expected
Systemic Effects (Major Burns >20% TBSA)
Cardiovascular: Capillary leak → hypovolemia → shock. Cardiac output falls in first 24 hrs.
Respiratory: Inhalation injury → carbon monoxide poisoning, airway edema, ARDS.
Renal: Hypovolemia + myoglobinuria (in electrical burns) → acute tubular necrosis.
Metabolic: Hypermetabolic state (BMR doubles) → catabolism, protein wasting, hyperglycemia.
Immune: Immune suppression → increased infection risk.
American Burn Association - Major Burn Classification (Requires Hospital Transfer)
- Partial thickness >25% TBSA (adult), >20% (elderly/child)
- Full thickness >10% TBSA
- Burns of face, hands, feet, genitalia, perineum, or major joints
- Circumferential extremity or chest burns
- Inhalation injury
- Chemical or electrical burns
- Burns + major trauma
Management
Immediate/First Aid:
- Stop burning process (cool with running water 10-20 min; do NOT use ice)
- Remove jewellery, non-adherent clothing
- Cover with clean dressing
- ABC assessment
Fluid Resuscitation - Parkland Formula:
4 mL × body weight (kg) × % TBSA burned
- Give half in the first 8 hours (from time of burn, not arrival)
- Give remaining half over next 16 hours
- Fluid: Lactated Ringer's solution
- Monitor: urine output target 0.5-1 mL/kg/hr (adults), 1 mL/kg/hr (children)
- Note: only 2nd and 3rd degree burns are counted; 1st degree excluded
Wound Care:
- Debride blisters (or leave intact - controversial)
- Topical agents: Silver sulfadiazine (most common), mafenide acetate, silver nitrate
- Synthetic dressings (e.g., Biobrane) for partial thickness
Surgical:
- Escharotomy: For circumferential full-thickness burns → compartment syndrome → incise eschar along full length of limb
- Fasciotomy: If compartment syndrome persists
- Early excision and skin grafting: Within 3-5 days for deep partial/full thickness
- Split-thickness skin graft (STSG): from thigh, buttock (donor site)
- Full-thickness skin graft (FTSG): for face, hands
Inhalation Injury:
- 100% O₂ via non-rebreather mask (carbon monoxide poisoning)
- Early intubation if: stridor, hoarseness, facial burns, singed nasal hair, carbonaceous sputum
- Bronchoscopy to assess airway
Nutritional support: High calorie, high protein (enteral preferred)
Infection prevention: Tetanus prophylaxis; wound care; antibiotics only for confirmed infection (not prophylactic)
Physiotherapy in Burns
- Positioning: Anti-contracture positioning from day 1 (neck extension, shoulder abduction, elbow extension, hip extension, knee extension, ankle dorsiflexion)
- Splinting: Custom splints to prevent contracture
- Exercises: Active/passive ROM, progressive strengthening
- Scar management: Pressure garments (worn 23 hrs/day for 1-2 years), silicone sheets, massage
- Ambulation: Early walking prevents complications
- Respiratory physio: Breathing exercises, suctioning, chest physio for inhalation injury patients
3. WOUND & MANAGEMENT (15 Marks)
Definition
A wound is a disruption of the normal continuity of body tissue, either intentional (surgical) or unintentional (traumatic).
Classification of Wounds
By Cause:
- Incised: Clean cut by sharp instrument
- Laceration: Irregular tear
- Abrasion: Superficial scraping
- Puncture/Stab: Deep narrow wound
- Contusion: Closed, bruised tissue
- Avulsion: Skin/tissue torn away
- Bite wound: Animal/human; high infection risk
By Contamination (Surgical Wound Classification):
| Class | Type | Examples | SSI Risk |
|---|
| I | Clean | Hernia repair, joint replacement | 1-2% |
| II | Clean-contaminated | Cholecystectomy, appendicectomy (non-perforated) | 5-10% |
| III | Contaminated | Perforated appendix, traumatic wound <4 hrs | 15-20% |
| IV | Dirty/Infected | Pus, perforation, devitalized tissue | >30% |
Types of Wound Healing
-
Primary intention (First intention): Clean wound with approximated edges (sutured). Minimal scarring. Surgical incisions.
-
Secondary intention: Wound left open; heals by granulation tissue formation, contraction, epithelialization. Larger scar. Used for infected wounds, pressure ulcers, abscess cavities.
-
Tertiary intention (Delayed primary closure): Wound cleaned and left open 4-5 days, then sutured. Used for contaminated traumatic wounds.
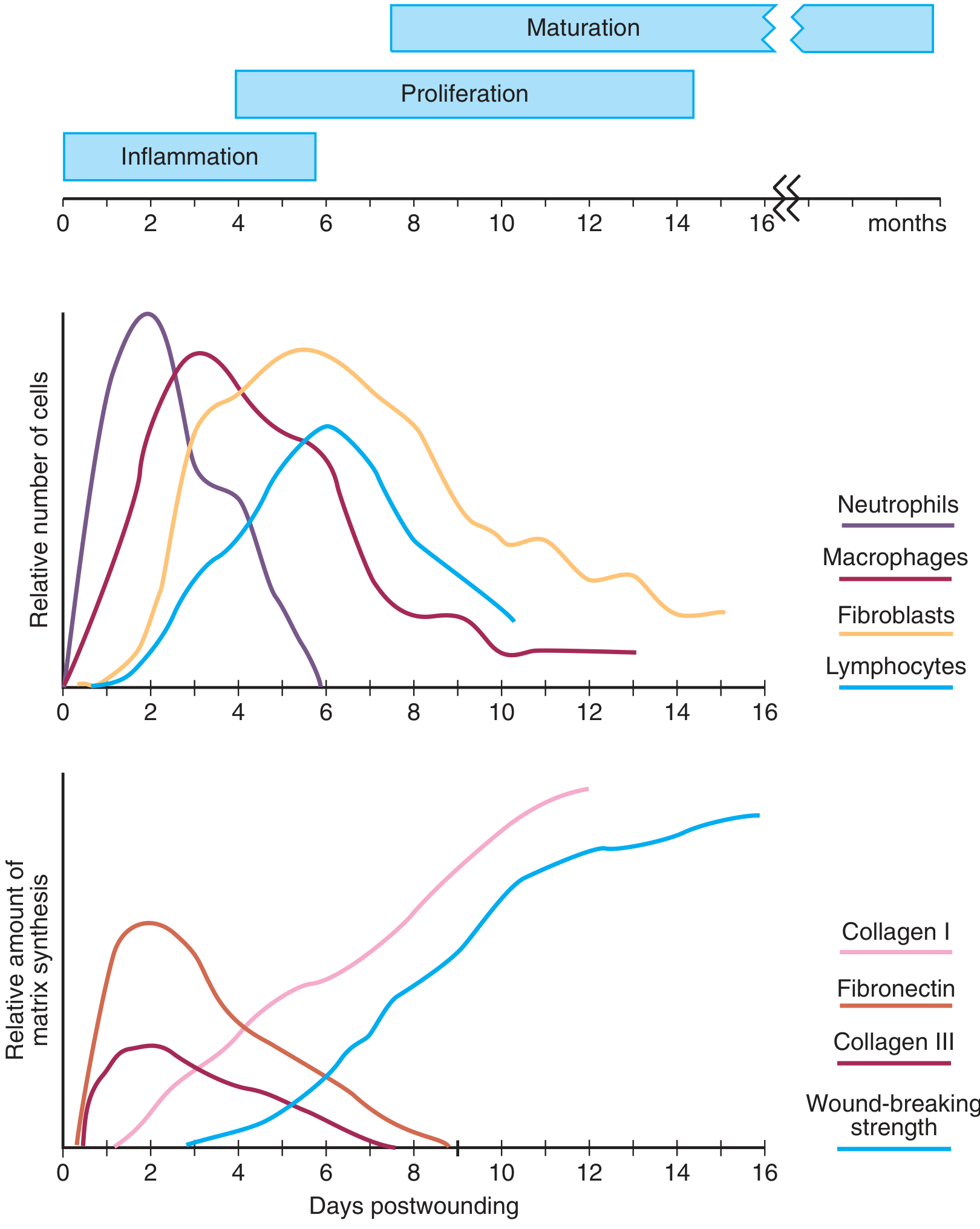
Phases of Wound Healing
Phase 1 - Hemostasis (Immediate - hours):
- Vasoconstriction (immediate, 5-10 min)
- Platelet activation and aggregation
- Coagulation cascade → fibrin clot
- Clot acts as scaffold and reservoir for growth factors
Phase 2 - Inflammatory Phase (Days 1-4):
- Vasodilation + increased permeability (mediated by histamine, prostaglandins)
- Neutrophils (peak day 1-2): phagocytosis of bacteria and debris; release of proteases and ROS
- Macrophages (peak day 2-3): the master regulators; phagocytosis + release of key growth factors (PDGF, TGF-β, VEGF, EGF, FGF)
- T-lymphocytes arrive at day 5-7; bridge inflammation to proliferation
- Signs: Redness, warmth, swelling, pain (cardinal signs)
Phase 3 - Proliferative Phase (Days 4-21):
- Fibroblasts (recruited by PDGF): proliferate, synthesize extracellular matrix
- Collagen synthesis: Type III collagen first (provisional), later replaced by Type I
- Requires: Vitamin C (for hydroxylation of proline/lysine), oxygen, zinc
- Angiogenesis: New capillaries form (VEGF-driven); granulation tissue = fibroblasts + capillaries + matrix
- Wound contraction: Myofibroblasts (differentiated fibroblasts) pull wound edges together; reduces wound size by up to 40-80%
- Re-epithelialization: Keratinocytes migrate from wound edges
Phase 4 - Remodeling/Maturation (Day 21 - 2 years):
- Type III collagen replaced by Type I collagen (stronger, organized)
- Cross-linking of collagen fibers
- Tensile strength increases progressively: 50% at 6 weeks; maximum 80% of original tissue at 1-2 years (never 100%)
- Scar initially red and raised → becomes pale and flat over months
Macrophage Activities in Wound Healing (Critical)
| Activity | Mediators |
|---|
| Phagocytosis | ROS, Nitric oxide |
| Debridement | Collagenase, elastase |
| Cell recruitment | PDGF, TGF-β, EGF, IGF |
| Angiogenesis | FGF, VEGF, TNF-α |
| Matrix synthesis | TGF-β, collagenase |
Factors Affecting Wound Healing
Local Factors:
- Infection (most common cause of delayed healing)
- Poor blood supply (ischemia, pressure, radiation)
- Foreign body / dead space
- Wound tension / edema
- Hematoma formation
- Denervation (e.g., neuropathic ulcers)
Systemic Factors:
- Diabetes mellitus (hyperglycemia impairs neutrophil function, reduces growth factors, microvascular disease)
- Malnutrition (low protein = poor collagen; Vitamin C deficiency = impaired hydroxylation; Zinc deficiency)
- Age (slower cell turnover, reduced growth factors)
- Steroids / immunosuppressants (suppress inflammation and proliferation)
- Anemia (reduced oxygen delivery)
- Jaundice / uremia (toxic metabolites impair healing)
- Smoking (vasoconstriction, reduced O₂, impairs angiogenesis)
- Obesity (poor vascularity of fat, increased tension)
- Malignancy / radiotherapy
Wound Complications
| Complication | Description |
|---|
| Infection | Most common; pus, cellulitis, fever |
| Dehiscence | Wound edges separate (usually day 5-8); risk: obesity, infection, steroids |
| Evisceration | Abdominal contents protrude through dehisced wound; emergency |
| Sinus | Blind-ending tract leading to wound surface |
| Fistula | Abnormal communication between two epithelial surfaces |
| Keloid | Excessive scar beyond wound margins; does not regress; hypertrophic scars stay within margins |
| Contracture | Excess fibrosis with functional limitation; common over joints post-burn |
| Seroma | Collection of serous fluid in wound space |
| Hematoma | Collection of blood; increases infection risk |
Wound Dressings and Management
| Dressing Type | Use |
|---|
| Simple gauze | Basic coverage |
| Hydrocolloid (e.g., DuoDERM) | Partial thickness wounds, promotes moist healing |
| Alginate | Highly exudating wounds |
| Hydrogel | Dry/necrotic wounds; rehydrates eschar |
| Silver-containing | Infected or high-infection-risk wounds |
| Negative Pressure Wound Therapy (NPWT/VAC) | Complex wounds, post-dehiscence, pressure ulcers |
| Biological (skin grafts, allografts) | Deep burns, large wounds |
4. BLOOD TRANSFUSION (15 Marks)
Definition
Blood transfusion is the therapeutic administration of blood or blood components from a donor to a recipient.
Blood Group Systems
- ABO system: A, B, AB, O (determined by antigens on RBC)
- O negative = Universal donor
- AB positive = Universal recipient
- Rhesus (Rh) system: Most important after ABO; Rh-D antigen
- Rh-negative women of childbearing age should receive Rh-negative blood
Pre-Transfusion Testing
- ABO and Rh typing
- Antibody screen (indirect Coombs test)
- Cross-matching: Mix donor RBCs with recipient serum; detects incompatibility
- Electronic crossmatch
- Immediate spin crossmatch
- Full serological crossmatch (takes 45-60 min; most thorough)
Blood Products and Indications
| Product | Storage | Shelf Life | Indication | Dose Effect |
|---|
| Whole blood | 4°C | 21-35 days | Massive hemorrhage, combat | - |
| PRBC (Packed Red Blood Cells) | 4°C | 42 days | Anemia, hemorrhage (Hb <7-8 g/dL) | 1 unit raises Hb ~1 g/dL |
| FFP (Fresh Frozen Plasma) | -30°C | 1 year | Coagulopathy, liver failure, warfarin reversal, massive transfusion | Contains all clotting factors |
| Platelets | 20-24°C (agitated) | 5-7 days | Thrombocytopenia (<50,000 for surgery, <10,000 prophylactic) | 1 pool raises count by ~30,000 |
| Cryoprecipitate | -30°C | 1 year | DIC, hypofibrinogenemia, hemophilia A, vWD | Rich in fibrinogen, VIII, XIII, vWF |
| Albumin 4.5% | Room temp | 3 years | Hypoalbuminemia, SBP, HRS | Oncotic support |
Transfusion Triggers (Evidence-Based)
| Patient Type | Transfusion Trigger |
|---|
| Stable non-cardiac patient | Hb <7 g/dL (restrictive threshold) |
| Cardiac disease / post-cardiac surgery | Hb <8 g/dL |
| Active hemorrhage with hemodynamic instability | Regardless of Hb |
| Platelets (surgery/invasive procedure) | <50,000/µL |
| Platelets (critical bleeding) | <100,000/µL |
Complications of Blood Transfusion
ACUTE (within 24 hours):
| Reaction | Mechanism | Features | Management |
|---|
| Acute Hemolytic Reaction (most dangerous) | ABO incompatibility; IgM antibodies | Fever, chills, back pain, hemoglobinuria, hypotension, renal failure | STOP transfusion; IV fluids; furosemide; monitor renal function |
| Febrile Non-Hemolytic (most common) | Antibodies to donor WBC antigens | Fever (≥1°C rise), chills | Stop transfusion; antipyretics; restart slowly if no hemolysis |
| Allergic/Urticarial | Antibodies to plasma proteins | Urticaria, pruritus | Antihistamines; continue if mild |
| Anaphylaxis | IgA-deficient recipient with anti-IgA | Anaphylaxis, bronchospasm, shock | STOP; epinephrine; steroids |
| TRALI (Transfusion-Related Acute Lung Injury) | Donor anti-HLA/anti-neutrophil antibodies | ARDS within 6 hours; bilateral infiltrates | STOP; O₂; mechanical ventilation; no diuretics |
| TACO (Transfusion-Associated Circulatory Overload) | Volume overload | Pulmonary edema, hypertension, hypoxia | Slow rate; diuretics; upright positioning |
| Septic | Bacterial contamination (platelets highest risk) | High fever, rigor, septic shock | STOP; blood cultures; IV antibiotics |
| Air embolism | Air in line | Dyspnoea, cyanosis, cardiac arrest | Left lateral + Trendelenburg; aspiration |
DELAYED (>24 hours):
- Delayed hemolytic reaction (3-10 days): Minor blood group antibody boosting
- Post-transfusion purpura: 5-10 days; thrombocytopenia
- Alloimmunization: Development of new RBC, HLA, platelet antibodies
- Transfusion-transmitted infections: HIV, HCV, HBV, malaria, CMV, variant CJD
- Iron overload: After >20 transfusions; use desferrioxamine
- Graft-versus-host disease (TA-GvHD): Immunocompromised patients; prevent with irradiated blood
Massive Transfusion Protocol (MTP)
- Definition: ≥10 units PRBC in 24 hours (or ≥4 units in 1 hour)
- Balanced resuscitation ratio: PRBC : FFP : Platelets = 1:1:1
- Monitor for:
- Hypothermia (use blood warmers)
- Hypocalcemia (citrate chelates calcium → give 10 mL 10% calcium gluconate per 4 units)
- Hyperkalemia (older blood releases K⁺)
- Dilutional coagulopathy
- Metabolic alkalosis (citrate converted to bicarbonate)
5. MINIMALLY INVASIVE SURGERY (MIS) / LAPAROSCOPY (15 Marks)
Definition
Minimally invasive surgery refers to surgical procedures performed through small incisions (ports, 5-12 mm) using a camera (laparoscope/endoscope) and specialized instruments, as opposed to traditional open surgery.
Types of MIS
| Type | Approach | Example |
|---|
| Laparoscopy | Abdominal ports + CO₂ pneumoperitoneum | Cholecystectomy, appendicectomy |
| Thoracoscopy (VATS) | Thoracic ports | Lung biopsy, lobectomy |
| Arthroscopy | Joint | Knee meniscectomy, ACL repair |
| Endoscopy (NOTES) | Natural orifice | Endoscopic mucosal resection |
| Robotic surgery | Robotic arms (da Vinci) | Prostatectomy, gastrectomy |
Physiological Basis of CO₂ Pneumoperitoneum
When the abdomen is insufflated with CO₂ to a pressure of 12-15 mmHg:
Respiratory effects:
- Diaphragm pushed cephalad → reduced FRC, reduced lung compliance
- Ventilation-perfusion mismatch
- CO₂ absorption from peritoneum → hypercapnia (hypercarbia)
- Requires increased minute ventilation during anaesthesia
Cardiovascular effects:
- Increased intra-abdominal pressure → decreased venous return (preload)
- Compression of IVC → decreased cardiac output
- Reflex sympathetic activation → increased HR and SVR
- Reverse Trendelenburg (head up) worsens venous return
Other effects:
- Reduced renal perfusion → decreased urine output during procedure
- Risk of CO₂ embolism (rare but life-threatening)
- Hypothermia (cold dry CO₂ gas)
Steps of Laparoscopic Cholecystectomy (Standard Procedure)
- General anaesthesia + endotracheal intubation
- Veress needle inserted (umbilicus) OR Hasson technique (open) for initial access
- CO₂ insufflation to 12-15 mmHg
- 10 mm camera port at umbilicus
- 3 working ports (5 mm) - epigastric, right flank, right hypochondrium
- Patient tilted: head up (reverse Trendelenburg) + left tilt
- Gallbladder retracted; Calot's triangle dissected
- Critical view of safety: cystic duct and cystic artery identified
- Clip and divide cystic duct and artery
- Gallbladder dissected off liver bed using electrocautery
- Specimen extracted through umbilical port (via endoscopy bag)
- Deflation and port closure
Advantages vs Open Surgery
| Advantage | Mechanism | Physiotherapy Relevance |
|---|
| Smaller incisions | Less tissue cutting | Less pain → easier breathing exercises |
| Less blood loss | Magnified view aids haemostasis | Less anaemia, less fatigue |
| Shorter hospital stay | Less trauma, faster recovery | Earlier start to rehab |
| Less respiratory compromise | Smaller incision, less splinting | Easier lung recruitment |
| Reduced adhesion formation | Less peritoneal handling | Lower bowel obstruction risk |
| Better cosmesis | Smaller scars | Psychological benefit |
| Lower SSI rate | Smaller wound | Less wound care |
Disadvantages / Complications of Laparoscopy
Conversion to open surgery: If bleeding, poor visualization, technical difficulty (~5%)
Specific complications:
| Complication | Cause | Feature |
|---|
| Port site bleeding | Vessel injury at insertion | Haematoma |
| Visceral injury | Veress needle, Trocar | Bowel/bladder perforation |
| Gas embolism | CO₂ into vascular system | Cardiovascular collapse |
| Subcutaneous emphysema | CO₂ tracking under skin | Crepitus on palpation |
| Shoulder tip pain | Residual CO₂ under diaphragm (referred pain) | Right shoulder, resolves 24-48 hrs |
| Port site hernia | Fascial defect at port >10 mm | Protruding hernia |
| Bile duct injury | Misidentification | Jaundice, biliary peritonitis |
| Deep vein thrombosis | Pneumoperitoneum + positioning | DVT/PE |
Physiotherapy Post-Laparoscopy
- Shoulder tip pain: Lying flat, local heat, gentle shoulder movements; caused by diaphragmatic irritation from residual CO₂
- Deep breathing exercises: Day 1 post-op (incentive spirometry)
- Early ambulation: 4-6 hours post-operatively
- Core stability: Avoid strenuous core exercises for 2 weeks
- Port site care: Observe for hernia signs when exercises increase intra-abdominal pressure
- DVT prophylaxis: Compression stockings + early mobilization
6. ABDOMINAL INCISIONS (15 Marks)
Definition
An abdominal incision is a planned surgical cut through the abdominal wall to access the peritoneal cavity.
Principles of a Good Incision
- Adequate exposure of operative field
- Minimal nerve and muscle damage
- Good cosmetic result
- Low risk of hernia
- Extensible if needed
- Secure closure
Layers of Abdominal Wall (from outside to inside)
- Skin
- Subcutaneous fat (Camper's fascia superficial, Scarpa's fascia deep)
- External oblique aponeurosis
- Internal oblique
- Transversus abdominis
- Transversalis fascia
- Extraperitoneal fat (preperitoneal)
- Peritoneum (parietal)
Midline incision goes through: Skin → Fat → Linea alba → Transversalis fascia → Peritoneum (no muscle cutting)
Classification and Types of Incisions
VERTICAL INCISIONS:
| Incision | Location | Surgery Used For |
|---|
| Midline (Median) | Along linea alba; can be upper, lower, or total | Exploratory laparotomy, bowel resection, aortic surgery |
| Paramedian | 2.5 cm lateral to midline; splits rectus sheath, retracts muscle | Colonic surgery |
| Pararectal (Battle's) | Lateral border of rectus | Rarely used |
TRANSVERSE / OBLIQUE INCISIONS:
| Incision | Location | Surgery Used For |
|---|
| Pfannenstiel | Low transverse suprapubic (along pubic hairline) | C-section, gynaecological surgery (excellent cosmesis) |
| Kocher (Subcostal) | Below costal margin, right or bilateral | Open cholecystectomy (right), splenectomy (left) |
| Gridiron (McBurney's) | Right iliac fossa, oblique (McBurney's point = 1/3 ASIS to umbilicus) | Open appendicectomy |
| Lanz | Right iliac fossa, transverse | Appendicectomy (better cosmesis than Gridiron) |
| Rutherford-Morrison (Hockey stick) | Extends Pfannenstiel laterally | Renal transplant |
SPECIAL INCISIONS:
| Incision | Location | Surgery Used For |
|---|
| Rooftop (Chevron) | Bilateral subcostal, meeting at xiphoid | Liver transplant, gastrectomy |
| Thoracoabdominal | Chest + abdomen combined | Esophagogastrectomy, adrenalectomy |
| Kehr's incision | T-shaped in upper abdomen | Hepatic surgery |
Wound Closure - Principles
Suture materials:
- Absorbable: Vicryl, PDS, Monocryl (fascial closure, internal layers)
- Non-absorbable: Prolene, nylon, silk (skin, vessels)
Mass closure (Jenkins Rule): Suture length:wound length = 4:1; 1 cm bites, 1 cm apart; reduces incisional hernia
Tension-free closure: Essential to prevent dehiscence and hernia
Drains: Used in contaminated fields or when dead space expected (e.g., liver surgery)
Complications of Incisions
| Complication | Prevention |
|---|
| Incisional hernia | Mass closure, avoid infection, correct nutrition |
| Wound dehiscence | Adequate suturing, control infection, treat cough |
| Keloid / hypertrophic scar | Minimise wound tension, use pfannenstiel where possible |
| Nerve damage | Knowledge of anatomy (e.g., ilioinguinal nerve in gridiron) |
| Haematoma | Good haemostasis |
Physiotherapy Post-Laparotomy
- Respiratory: Risk of basal atelectasis (splinting due to pain); teach diaphragmatic breathing and huffing from day 1
- Abdominal support: Pillow or binder when coughing (reduces pain)
- Early mobilization: Sitting up day 1, walking day 1-2 (reduces ileus, DVT, pneumonia)
- Core exercises: Delayed 4-6 weeks; avoid increasing IAP (no Valsalva)
- Incentive spirometry: Every 1-2 hours while awake for first 48-72 hrs
7. SURGICAL SITE INFECTIONS (SSI) (15 Marks)
Definition (CDC)
SSI is an infection occurring at or near a surgical incision site within 30 days of surgery (or within 90 days if an implant is in place). (CDC/NHSN definition)
Classification (CDC - 3 Types)
-
Superficial Incisional SSI
- Involves skin and subcutaneous tissue only
- Signs: redness, warmth, purulent drainage, pain at wound
- Diagnosed clinically within 30 days
-
Deep Incisional SSI
- Involves deep soft tissues (fascia and muscle layers)
- Signs: wound opens spontaneously, purulent drainage from deep layer, fever
- May require re-exploration
-
Organ/Space SSI
- Involves any organ or space opened/manipulated during surgery
- Examples: intra-abdominal abscess, empyema, osteomyelitis of sternum
- Diagnosed by culture or imaging
Microbiology - Common Organisms
| Organism | Common SSI Type |
|---|
| Staphylococcus aureus (MSSA and MRSA) | Most common overall; skin flora |
| Coagulase-negative Staphylococci | Implant/device infections |
| Enterococcus faecalis/faecium | Abdominal, pelvic surgery |
| E. coli | Abdominal surgery, colorectal |
| Pseudomonas aeruginosa | ICU patients, burns, immunocompromised |
| Klebsiella pneumoniae | Abdominal surgery |
| Bacteroides fragilis | Colorectal surgery |
Risk Factors
Patient-Related:
- Diabetes mellitus (hyperglycemia impairs neutrophils)
- Obesity (poor vascularization of fat, wound tension)
- Malnutrition (poor immune function and healing)
- Immunosuppression (steroids, chemotherapy, HIV)
- Smoking (vasoconstriction, impaired healing)
- Age extremes
- Remote infection at time of surgery (skin, UTI)
- ASA class ≥3
Surgery-Related:
- Wound class (contaminated > clean-contaminated > clean)
- Duration of surgery (>2 hours = higher risk)
- Emergency surgery
- Inadequate skin preparation
- Hair removal with razor (vs. clipper)
- Hypothermia intraoperatively
- Hyperglycemia intraoperatively
- Inadequate antibiotic prophylaxis
- Poor surgical technique (excessive tissue trauma, dead space, haematoma)
- Drains left in >48 hrs
Prevention Bundle (WHO / CDC Guidelines)
Pre-operative:
- Identify and treat remote infections before elective surgery
- Nasal decolonization for MRSA carriers (mupirocin nasal ointment)
- Nutritional optimization
- Skin preparation: Chlorhexidine-alcohol (superior to povidone-iodine)
- Hair removal: Clippers on day of surgery (NOT razors - razors increase risk)
- Shower with antiseptic soap night before
Intra-operative:
- Antibiotic prophylaxis: IV cefazolin given within 60 minutes before incision (or 120 min for vancomycin)
- Redose antibiotics if surgery >4 hours (for cefazolin, t½ = 2 hrs → redose at 4 hrs)
- Maintain normothermia (body temp 36-37°C) - warming blankets, warm IV fluids
- Maintain normoglycemia (BGL <200 mg/dL; ideally <180 mg/dL)
- Maintain adequate tissue oxygenation
- Careful tissue handling; minimize dead space
- Sterile technique throughout
Post-operative:
- Wound closed with sterile dressing for 48 hours
- Do not disturb wound unnecessarily in first 48 hrs
- Proper hand hygiene before wound care
- Prophylactic drains removed early when safe
Diagnosis
Clinical signs of SSI:
- Rubor (redness/erythema)
- Calor (warmth)
- Dolor (pain/tenderness)
- Tumor (swelling)
- Functio laesa (loss of function)
- Purulent discharge from wound
- Fever >38°C after 48-72 hours post-op
- Elevated WBC and CRP
Investigations:
- Wound swab for culture and sensitivity
- Blood cultures if systemic sepsis
- Ultrasound / CT scan for deep/organ space SSI
Treatment
| SSI Type | Treatment |
|---|
| Superficial | Open wound, drainage; clean dressings; antibiotics only if cellulitis/systemic signs |
| Deep incisional | Explore, open, drain, debride; IV antibiotics; re-suture once clean |
| Organ/space | Percutaneous drainage (image-guided) or surgery; IV antibiotics tailored to culture |
| MRSA | Vancomycin (IV) or linezolid; decolonization protocols |
8. HEMORRHAGE (15 Marks)
Definition
Hemorrhage is the escape of blood from the cardiovascular system due to disruption of vessel integrity.
Classification
By Vessel Type:
| Type | Appearance | Rate |
|---|
| Arterial | Bright red, pulsatile | Rapid, life-threatening |
| Venous | Dark red, continuous flow | Moderate |
| Capillary | Red, oozing | Slow, usually self-limiting |
By Timing (Surgical Classification - Most Important):
| Type | Timing | Cause |
|---|
| Primary | At time of injury/surgery | Vessel damage |
| Reactionary | Within 24 hours post-op | Blood pressure rises, dislodges clot; ligatures slip |
| Secondary | 7-14 days post-op | Infection erodes vessel wall |
By Site:
| Type | Example |
|---|
| External | Visible through wound/body orifice |
| Internal | Into body cavities (hemothorax, hemoperitoneum, hemarthrosis) |
| Concealed (Occult) | Internal, not clinically obvious |
Special types:
- Hematemesis: Vomiting blood (upper GI source)
- Melena: Black tarry stools (upper GI >60 mL)
- Hematochezia: Bright red rectal bleeding (lower GI or massive upper GI)
- Hemoptysis: Coughing blood (respiratory tract)
- Epistaxis: Nasal bleeding
Physiological Response to Hemorrhage
Compensatory mechanisms (auto-triggered):
- Baroreceptor activation → sympathetic surge
- Catecholamine release → tachycardia + vasoconstriction
- ADH (vasopressin) release → water retention
- RAAS activation → aldosterone → Na+ and water retention
- Fluid shift from interstitial to intravascular
- Increased RBC production (EPO)
When compensation fails:
- Class III-IV shock develops (see Shock section)
- Lethal triad: hypothermia + coagulopathy + acidosis
Management
Immediate Hemorrhage Control:
- Direct pressure (most effective first aid)
- Elevation of limb
- Tourniquet for limb hemorrhage uncontrolled by pressure
- Wound packing with haemostatic gauze (e.g., Combat Gauze)
- Pressure points (brachial, femoral)
- Wound closure (suturing, stapling)
Surgical Hemorrhage Control:
- Ligation of bleeding vessel
- Suture-ligation for vessel in wound bed
- Diathermy/electrocautery (mono or bipolar)
- Haemostatic clips (e.g., laparoscopic surgery)
- Endovascular embolization (interventional radiology) - for solid organ, pelvic fractures
- Damage control surgery: Temporary packing and return for definitive repair after resuscitation
Pharmacological:
- Tranexamic acid (TXA): Antifibrinolytic; 1g IV given within 3 hours of injury (CRASH-2 trial showed reduced mortality)
- Desmopressin (DDAVP): For platelet dysfunction, von Willebrand disease
- Vitamin K: For warfarin reversal
- Protamine sulfate: For heparin reversal
- Prothrombin Complex Concentrate (PCC): For warfarin/DOAC reversal
Volume Replacement:
- Class I-II: Crystalloids (normal saline, Hartmann's)
- Class III-IV: Blood products + crystalloids (see Blood Transfusion)
Physiotherapy in Hemorrhage Management
- Position patient: flat (or slight Trendelenburg for limb bleeding) to maximise cerebral perfusion
- Do NOT elevate head in active hemorrhagic shock
- Compression bandaging and immobilization of fractures reduces blood loss
- Post-hemorrhage rehab: Graded exercise for fatigue/deconditioning; Hb monitoring before exercise prescription; orthostatic hypotension management
9. ANAESTHESIA (15 Marks)
Definition
Anaesthesia is the controlled, reversible loss of sensation (and often consciousness) produced by pharmacological agents to allow surgery to be performed without pain.
Components of General Anaesthesia (Triad)
- Analgesia - absence of pain
- Unconsciousness (Hypnosis) - loss of awareness
- Muscle relaxation - surgical access and airway management
(Some add: amnesia and attenuation of autonomic reflexes)
Types of Anaesthesia
A. General Anaesthesia (GA):
- Patient is completely unconscious and paralysed
- Induction: IV agents - Propofol (most common), ketamine, thiopentone
- Maintenance: Volatile inhalation agents (sevoflurane, isoflurane, desflurane) + IV (TIVA with propofol)
- Muscle relaxation: Neuromuscular blocking agents
- Depolarizing: Succinylcholine (suxamethonium) - rapid onset, short duration; causes fasciculations; risk of hyperkalemia
- Non-depolarizing: Rocuronium, vecuronium, atracurium - reversed by neostigmine (or sugammadex for rocuronium)
- Airway: Endotracheal tube (ETT), laryngeal mask airway (LMA), facemask
- Reversal: Neostigmine + atropine (or sugammadex)
B. Regional Anaesthesia:
| Type | Mechanism | Use |
|---|
| Spinal (SAB) | Local anaesthetic (bupivacaine, lignocaine) into subarachnoid space (CSF) at L3-L4 | Lower limb surgery, LSCS, urological surgery |
| Epidural | LA into epidural space (outside dura); catheter can remain for continuous infusion | Labour analgesia, post-op pain, major thoracic/abdominal surgery |
| Peripheral nerve block | US or landmark-guided injection around specific nerve | Brachial plexus (shoulder/arm), femoral nerve (knee), sciatic nerve |
| IV regional (Bier's block) | LA injected into IV of exsanguinated limb under tourniquet | Upper limb surgery <1 hour |
C. Local Anaesthesia:
- Infiltration of LA agent directly into tissue
- Agents: Lignocaine (max 3-4 mg/kg; 7 mg/kg with adrenaline), bupivacaine (long-acting), ropivacaine
- Mechanism: Block Na⁺ channels → prevent depolarization
D. Monitored Anaesthesia Care (MAC) / Sedation:
- IV sedation with maintained verbal contact
- Propofol, midazolam, fentanyl
- Used for endoscopy, minor procedures, pain procedures
Stages of General Anaesthesia (Guedel's Classification)
| Stage | Name | Features |
|---|
| Stage 1 | Analgesia | Conscious; analgesia; amnesia possible |
| Stage 2 | Excitement/Delirium | Unconscious but excited; irregular breathing; vomiting risk; DO NOT OPERATE |
| Stage 3 | Surgical anaesthesia | Regular breathing; muscle relaxation; surgery can begin |
| Stage 4 | Medullary depression | Respiratory and cardiovascular centre depression → DEATH |
Pre-anaesthetic Assessment
History: Medical history, previous anaesthesia (problems?), medications, allergies, fasting status (NPO), smoking, alcohol, family history of malignant hyperthermia.
Examination: Airway assessment (Mallampati score, mouth opening, thyromental distance, neck mobility), cardiorespiratory status.
Investigations: FBC, U&E, LFTs, coagulation, ECG (>40 yrs or cardiac history), chest X-ray, echocardiography if indicated.
ASA Physical Status Classification:
| Grade | Description |
|---|
| ASA I | Healthy patient; no systemic disease |
| ASA II | Mild systemic disease (controlled DM, hypertension) |
| ASA III | Severe systemic disease, functional limitation (COPD, uncontrolled DM) |
| ASA IV | Severe systemic disease, constant threat to life (recent MI, severe HF) |
| ASA V | Moribund; not expected to survive 24 hrs |
| ASA VI | Brain-dead organ donor |
| ASA E suffix | Emergency surgery (adds risk to any grade) |
Fasting Guidelines (NPO):
- Clear fluids: 2 hours before
- Breast milk: 4 hours before
- Light meal/non-human milk: 6 hours before
- Full meal: 8 hours before
Complications of Anaesthesia
Airway:
- Aspiration (Mendelson's syndrome): Stomach contents aspirated; chemical pneumonitis → ARDS. Reason for strict NPO.
- Failed intubation: Difficult airway algorithm; can't intubate/can't oxygenate = surgical airway (cricothyroidotomy)
- Laryngospasm, bronchospasm
Cardiovascular:
- Hypotension (vasodilation from induction agents)
- Arrhythmias (volatile agents sensitize myocardium to catecholamines)
- Cardiac arrest
Respiratory:
- Hypoventilation, atelectasis
- Post-op respiratory depression (opioids, residual relaxants)
Metabolic:
- Malignant hyperthermia (MH): Rare; autosomal dominant; triggered by halogenated agents or succinylcholine; uncontrolled Ca²⁺ release → hyperthermia, muscle rigidity, acidosis, rhabdomyolysis. Treatment: Dantrolene (direct acting muscle relaxant)
Post-operative:
- PONV (Post-operative nausea and vomiting): Most common complaint; treat with ondansetron, dexamethasone, droperidol
- Post-operative delirium: Common in elderly; prevention with orientation, early mobilization
- Pain: VAS/NRS score guided multimodal analgesia
Physiotherapy Considerations
- Residual neuromuscular blockade → impaired cough, respiratory weakness
- Opioid analgesia → respiratory depression, reduced mobility
- Spinal anaesthesia → lower limb sensory/motor block (resolves in 2-4 hrs); assist early ambulation
- Epidural analgesia: maintains good pain control → better cooperation with breathing exercises; monitor for hypotension and epidural haematoma
- Post-GA: incentive spirometry + deep breathing from recovery room
10. ASSESSMENT OF A TRAUMA PATIENT (15 Marks)
Concept
The ATLS (Advanced Trauma Life Support) system provides a standardized, systematic approach to trauma assessment: PRIMARY SURVEY → RESUSCITATION → SECONDARY SURVEY → DEFINITIVE CARE → TERTIARY SURVEY
The goal: identify and treat immediately life-threatening conditions first.
PRIMARY SURVEY - ABCDE
A - Airway with Cervical Spine Protection
- Assess: Is the patient talking? (Patent airway if yes)
- Look for: stridor, gurgling, foreign bodies, maxillofacial injury, tracheal deviation
- All blunt trauma patients - assume C-spine injury until excluded
- Apply hard cervical collar + sandbags + tape (NOT soft collar)
- Airway manoeuvres: chin lift, jaw thrust
- Simple adjuncts: nasopharyngeal airway (NPA), oropharyngeal airway (OPA/Guedel)
- Definitive airway: Rapid Sequence Intubation (RSI) with in-line stabilization
- Cannot intubate: surgical airway (cricothyroidotomy)
B - Breathing and Ventilation
- Inspect, palpate, percuss, auscultate the chest
- Life-threatening conditions - identify and treat IMMEDIATELY:
| Condition | Signs | Treatment |
|---|
| Tension pneumothorax | Absent BS, hyperresonance, tracheal deviation, JVD, shock | Immediate needle decompression (2nd ICS, MCL) → chest tube |
| Open chest wound | Sucking chest wound | 3-sided occlusive dressing → chest tube |
| Massive hemothorax | Absent BS, dullness to percussion, shock | IV fluids + chest tube; may need surgery |
| Flail chest + pulmonary contusion | Paradoxical chest movement | Mechanical ventilation |
C - Circulation and Hemorrhage Control
- Assess: HR, BP, skin color/temperature/perfusion, pulse quality, capillary refill
- Control external bleeding: direct pressure, tourniquet
- IV access: 2 large-bore peripheral IVs (16G or larger)
- Fluid resuscitation: Warmed crystalloid + blood products
- Life-threatening conditions - treat immediately:
| Condition | Signs | Treatment |
|---|
| Major external hemorrhage | Visible bleeding | Direct pressure, tourniquet |
| Cardiac tamponade | Beck's triad, pulsus paradoxus | Pericardiocentesis; thoracotomy |
| Massive hemothorax | (See above) | Chest tube + surgery |
| Hemorrhagic shock | Tachycardia, hypotension | Fluid + blood resuscitation |
| Pelvic fracture | Pelvis unstable, hemodynamic instability | Pelvic binder, angioembolization |
D - Disability (Neurological Status)
- GCS (Glasgow Coma Scale):
| Component | Score |
|---|
| Eye opening (E): Spontaneous/To voice/To pain/None | 4/3/2/1 |
| Verbal response (V): Oriented/Confused/Words/Sounds/None | 5/4/3/2/1 |
| Motor response (M): Obeys/Localizes/Withdraws/Flexion/Extension/None | 6/5/4/3/2/1 |
| Total | 3-15 |
- GCS ≤8 = severe brain injury; intubate
- Pupil size and reactivity: unilateral fixed dilated pupil = herniation ipsilateral; bilateral fixed = brainstem
- Blood glucose (hypoglycemia mimics brain injury; treat with IV dextrose)
- AVPU scale (rapid): Alert / Voice / Pain / Unresponsive
E - Exposure and Environmental Control
- Fully undress patient to detect all injuries
- Logroll (4 people + team leader for head) to examine posterior
- Check: spine, buttocks, perineum, posterior wounds
- Prevent hypothermia: warm blankets, warm IV fluids, warm room
Concurrent RESUSCITATION (runs with primary survey)
- 2 large-bore IVs + IV fluids
- High-flow O₂ (15L/min via NRM)
- Cardiac monitor, pulse oximetry, capnography
- Urinary catheter (NOT if urethral injury suspected: blood at meatus, scrotal haematoma, high-riding prostate)
- Nasogastric tube (NOT if basal skull fracture: Battle's sign, raccoon eyes, haemotympanum, CSF leak - use oral-gastric instead)
FAST Exam (Focused Assessment with Sonography in Trauma):
- Pericardial space (tamponade)
- Right upper quadrant (hepatorenal space - Morrison's pouch)
- Left upper quadrant (splenorenal)
- Pelvis (free fluid)
- E-FAST adds lung scan (pneumothorax, hemothorax)
SECONDARY SURVEY (Head-to-Toe)
Begins ONLY when primary survey complete and patient is being resuscitated.
History - AMPLE:
- Allergies
- Medications
- Past medical history
- Last meal (fasting status)
- Events/mechanism of injury
Head-to-toe Exam:
| Region | Key Exam Points |
|---|
| Head/Scalp | Lacerations, depressed skull fracture |
| Face | Maxillofacial fractures (tripod, LeFort), eye injury |
| Ears | Haemotympanum, Battle's sign → basal skull fracture |
| Eyes | Raccoon eyes → basal skull fracture; visual acuity |
| Nose | Septal haematoma, CSF rhinorrhoea |
| Mouth | Dental injury, tongue laceration |
| Neck | Tracheal deviation, venous distension, C-spine tenderness, penetrating wound zones |
| Chest | Rib fractures (flail segment), lung fields, heart sounds |
| Abdomen | Tenderness, rigidity, distension; FAST/CT if indicated |
| Pelvis | Compress iliac wings for instability (once only); perineal injury |
| Extremities | Fractures, dislocations, neurovascular assessment, compartment syndrome signs |
| Neurological | Full GRCS, cranial nerves, sensation, power, reflexes; complete spinal exam |
| Posterior | Logroll: spine palpation, posterior chest, buttocks |
TERTIARY SURVEY
- Repeated head-to-toe exam at 24-72 hours
- Once sedation/paralysis reversed and patient cooperative
- Reviews all imaging
- Aims to catch missed injuries (commonly: small pneumothorax, hairline fractures, ligamentous injuries)
Physiotherapy in Trauma Assessment
- Physiotherapists are key members of the trauma rehabilitation team
- Early respiratory physiotherapy prevents atelectasis and pneumonia (especially with rib fractures)
- Rib fractures: incentive spirometry, IPPB, epidural analgesia facilitates deep breathing
- Spinal injury: logroll technique; positioning; bed mobility
- Limb fractures: elevation, cryotherapy, early joint mobilization once stable
- Traumatic brain injury: level of consciousness guides therapy approach; sensory stimulation, positioning
11. ULCER (15 Marks)
(See previous notes for full content - all ulcer subtypes, staging, and management principles covered comprehensively)
12. TUMORS (15 Marks)
(See previous notes for full content - classification, nomenclature, TNM staging, tumor markers, benign vs malignant features)
═══════════════════════════════════════
PART B - SHORT TOPICS (5 MARKS EACH)
═══════════════════════════════════════
1. PRIMARY & SECONDARY SURVEY IN TRAUMA (5 Marks)
Primary survey = ABCDE (identify immediate life threats)
| Letter | Assessment | Life Threat Treated |
|---|
| A | Airway + C-spine | Obstruction |
| B | Breathing + Ventilation | Tension PTX, open chest, massive hemothorax, flail |
| C | Circulation + Hemorrhage control | Major bleeding, tamponade |
| D | Disability (GCS + pupils) | Herniation, severe TBI |
| E | Exposure + prevent hypothermia | Hidden injuries |
Secondary survey = full head-to-toe exam + AMPLE history. Only begins after primary complete + resuscitation initiated. - Schwartz's Principles of Surgery, 11th Ed.
2. FIBROADENOMA (5 Marks)
- Most common benign breast tumor in young women (15-35 yrs)
- "Breast mouse" - firm, rubbery, well-defined, highly mobile, non-tender
- Estrogen-sensitive - grows in pregnancy; involutes post-menopause
- Histology: fibrous stroma + compressed epithelial ducts; intracanalicular or pericanalicular pattern
- Diagnosis: Triple assessment (Clinical + USS + FNAC)
- Management: Observation if <3 cm, confirmed benign; excision if >3 cm, rapid growth, or uncertain diagnosis
- Giant fibroadenoma (>5 cm): Excision; common in adolescents
3. HEMANGIOMA (5 Marks)
- Benign vascular tumor/hamartoma
- Types:
- Capillary (Strawberry nevus): Most common tumor of infancy; appears 2-4 weeks; rapid growth 6-12 months; spontaneously involutes by age 7; treat with propranolol if threatening
- Cavernous: Large dilated channels; most common benign liver tumor; does NOT involute; incidental finding; MRI shows peripheral nodular enhancement
- Port wine stain: Congenital capillary malformation; does not involute; associated with Sturge-Weber syndrome
- Kasabach-Merritt syndrome: Large hemangioma → platelet trapping → thrombocytopenia + DIC
4. BURKITT TUMOR / LYMPHOMA (5 Marks)
- Highly aggressive B-cell non-Hodgkin's lymphoma; fastest doubling time of any human cancer
- Types: Endemic (African) - jaw/facial bones, 100% EBV+; Sporadic - ileocecal region; Immunodeficiency-related (HIV)
- Translocation: t(8;14) → MYC oncogene overexpression (80%)
- Histology: "Starry sky" pattern - sheets of lymphocytes with scattered pale macrophages
- Features: Rapidly growing mass, B symptoms (fever, weight loss, night sweats), very high LDH
- Treatment: Intensive chemotherapy (CODOX-M/IVAC) + Rituximab; ~90% cure rate with early treatment
5. SUBDURAL HAEMATOMA (5 Marks)
- Blood collection between dura and arachnoid from bridging vein rupture
- Types:
| Type | Timing | CT Appearance |
|---|
| Acute | <72 hrs | Hyperdense (white) crescent |
| Subacute | 3-20 days | Isodense |
| Chronic | >3 weeks | Hypodense (dark) crescent |
- Crescent-shaped collection crosses suture lines (unlike EDH which is biconvex)
- Acute: Head injury, deteriorating GCS → craniotomy
- Chronic: Elderly, alcoholics; minor/forgotten trauma → headache, confusion, cognitive decline → burr-hole drainage
- Investigation of choice: Non-contrast CT scan
6. CARDIAC TAMPONADE (5 Marks)
- Blood/fluid in pericardial space → increased intrapericardial pressure → impaired cardiac filling → decreased CO
- Beck's Triad: Hypotension + Raised JVP + Muffled heart sounds
- Additional signs: Pulsus paradoxus (>10 mmHg SBP drop on inspiration); tachycardia; Kussmaul's sign
- ECG: Sinus tachycardia + low voltage + electrical alternans (pathognomonic)
- Diagnosis: Bedside ECHO/e-FAST (gold standard - pericardial fluid + RV diastolic collapse)
- Treatment: IV fluids (maintain preload) → pericardiocentesis (subxiphoid route) → pericardial window if recurs
- Common cause in trauma: Penetrating chest injury
7. PNEUMOTHORAX & TENSION PNEUMOTHORAX (5 Marks)
- Air in pleural space → lung collapse
- Tension pneumothorax: One-way valve mechanism → progressive air accumulation → mediastinal shift → contralateral lung compression + IVC kinking → obstructive shock → DEATH
5 Classic Signs of Tension PTX:
- Tracheal deviation (away from affected side)
- Absent breath sounds (ipsilateral)
- Hyperresonance on percussion (ipsilateral)
- Distended neck veins
- Hypotension + tachycardia
⚠️ CLINICAL DIAGNOSIS - Do NOT wait for X-ray. Treat immediately!
Immediate Treatment: Needle decompression - 2nd ICS, midclavicular line → followed by ICD (5th ICS, midaxillary line)
Simple pneumothorax <20%: High-flow O₂ + observation
Simple pneumothorax >20% or symptomatic: Aspiration or ICD
🔑 MASTER CHEAT SHEET - KEY NUMBERS
| Topic | Key Fact |
|---|
| Shock definition | Failure of tissue perfusion |
| Class III shock blood loss | 30-40% (1500-2000 mL) |
| Septic shock antibiotics | Within 1 hour |
| Parkland formula | 4 mL × kg × %TBSA |
| Burns - 1st half fluid | First 8 hours |
| Rule of Nines - each leg | 18% |
| 3rd degree burn | Painless, needs skin graft |
| Wound max tensile strength | 80% at 1-2 years |
| Type III → Type I collagen | Remodeling phase |
| PRBC raises Hb | ~1 g/dL per unit |
| Transfusion trigger (stable) | Hb <7 g/dL |
| Massive transfusion ratio | 1:1:1 (PRBC:FFP:Plt) |
| MTP definition | ≥10 units PRBC/24 hrs |
| SSI definition | 30 days (90 with implant) |
| Antibiotic prophylaxis | 60 min before incision |
| Laparoscopy insufflation | CO₂ 12-15 mmHg |
| Laparoscopy shoulder pain | Diaphragm irritation from CO₂ |
| Primary survey | ABCDE |
| GCS intubate | ≤8 |
| Needle decompression site | 2nd ICS, midclavicular line |
| ICD site | 5th ICS, midaxillary line |
| Fibroadenoma nickname | "Breast mouse" |
| Burkitt translocation | t(8;14) |
| Burkitt histology | Starry sky pattern |
| Subdural - bridging veins | Crescent-shaped, crosses sutures |
| Beck's triad | Hypotension + JVD + muffled heart sounds |
| Malignant hyperthermia treatment | Dantrolene |
| ATLS golden hour | Timely prioritized intervention |
| Tranexamic acid window | Within 3 hours of injury |
Sources: Schwartz's Principles of Surgery 11th Ed. | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Miller's Anesthesia 10th Ed. | Barash's Clinical Anesthesia 9th Ed. | Robbins Pathology