Thyroid gland anatomy in detailed explanation with simple way
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have rich content from multiple authoritative textbooks. Let me compile a comprehensive, simple explanation.
Thyroid Gland Anatomy - Detailed & Simple Explanation
1. What Is the Thyroid?
The thyroid is a butterfly-shaped endocrine gland in the front of your neck. It makes hormones that control your body's metabolism - basically how fast or slow your cells work.
2. Location
- Sits anterior (in front) of the trachea (windpipe), just below the cricoid cartilage (the ring-shaped cartilage you can feel at the bottom of your voice box)
- Covered in front by the strap muscles (sternohyoid and sternothyroid)
- Flanked on each side by the carotid sheaths (containing the major neck arteries and veins)
- The esophagus (food pipe) sits behind it, especially on the left
Think of it like a shield sitting on the front of your windpipe, just below your Adam's apple.
3. Gross Shape and Size
| Feature | Detail |
|---|---|
| Shape | Two lobes joined by a bridge (isthmus) - like a butterfly |
| Weight | 15-30 grams (normal range) |
| Each lobe size | ~5 cm tall, 2-3 cm front-to-back, 3 cm wide |
| Isthmus location | Just below the cricoid cartilage |
- Right lobe and left lobe - the two wings of the butterfly
- Isthmus - the bridge connecting them in the midline, lying over the 2nd-4th tracheal rings
- Pyramidal lobe - present in about 50% of people; a finger-like projection extending upward from the isthmus, toward the tongue. It is a remnant of the thyroglossal duct from embryonic life. It is not normally felt, but becomes palpable in thyroid enlargement (goiter, Graves' disease).
4. The Capsule and Ligaments
The thyroid has two layers around it:
- True capsule - a thin, tight fibrous layer directly on the gland. It sends inward projections (septa) that divide the gland into small sections called pseudolobules.
- False capsule (pretracheal fascia) - a loose outer layer formed by the deep cervical fascia. It is easy to lift off the gland during surgery unless the gland is inflamed or cancerous.
Two important ligament condensations:
- Anterior suspensory ligament - above the isthmus, anchors the thyroid
- Ligament of Berry (posterior suspensory ligament) - a firm attachment on the back of each lobe to the cricoid cartilage and upper tracheal rings. The recurrent laryngeal nerve (RLN) runs very close to this ligament and is most at risk of injury here during thyroid surgery.
5. Blood Supply
Think of the thyroid as one of the best-supplied organs in the body - it receives blood flow roughly 5 times its own weight per minute.
Arteries (bringing blood IN):
| Artery | Origin | Where It Enters |
|---|---|---|
| Superior thyroid artery (x2) | External carotid artery | Top (apex) of each lobe |
| Inferior thyroid artery (x2) | Thyrocervical trunk (from subclavian artery) | Middle of each lobe, from behind |
| Thyroidea ima artery (1-4% of people) | Directly from aorta or innominate artery | Isthmus |
The inferior thyroid artery crosses the recurrent laryngeal nerve - this is why surgeons must find the nerve before tying off this artery.
Veins (draining blood OUT):
| Vein | Drains Into |
|---|---|
| Superior thyroid vein | Internal jugular vein |
| Middle thyroid vein | Internal jugular vein |
| Inferior thyroid veins | Brachiocephalic veins |
6. Nerve Supply (Very Important in Surgery)
Recurrent Laryngeal Nerve (RLN)
- Branch of the vagus nerve (10th cranial nerve)
- Controls all muscles of the voice box (larynx) EXCEPT one
- Left RLN: loops under the aortic arch, ascends in the tracheoesophageal groove
- Right RLN: hooks under the right subclavian artery, takes a more diagonal path upward
- Key danger zone: runs right next to the ligament of Berry and the inferior thyroid artery
- Injury = hoarse voice (one side) or airway obstruction (both sides)
External Branch of the Superior Laryngeal Nerve
- Controls the cricothyroid muscle (which tenses the vocal cord for high-pitched sounds)
- Runs alongside the superior thyroid vessels before they enter the gland
- Injury = loss of high-pitched voice (singers are particularly affected)
7. Lymphatic Drainage
The thyroid has a rich lymphatic network. Lymph from the thyroid drains to:
- Central neck nodes (paratracheal, pretracheal nodes)
- Lateral cervical nodes (deep cervical chain along the jugular vein)
- Both lobes communicate through the isthmus
This is why thyroid cancer can spread to neck lymph nodes - understanding this anatomy guides surgical dissection.
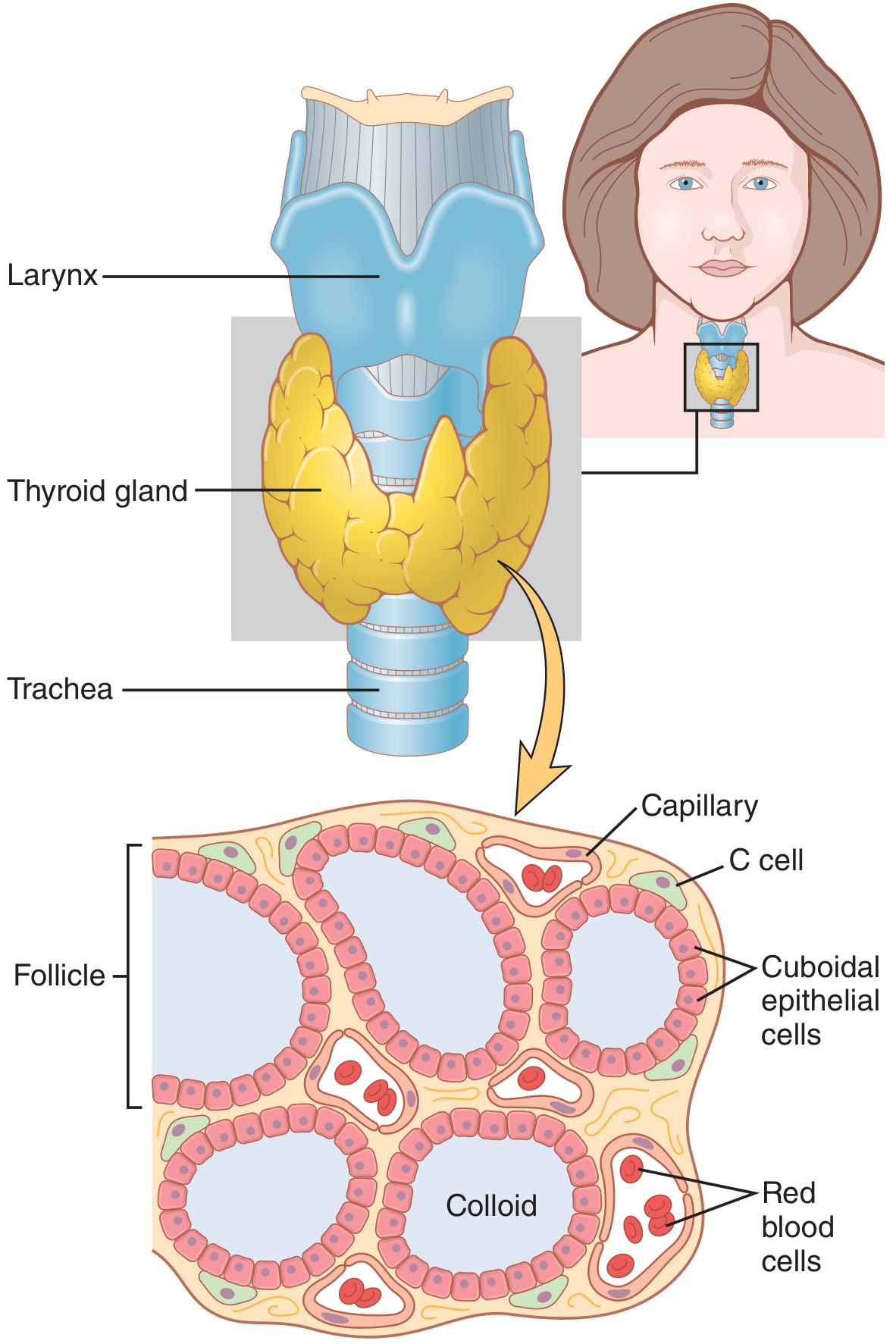
8. Microscopic (Histological) Anatomy
This is what the gland actually looks like under a microscope:
Follicles
- The gland is made up of thousands of tiny closed sacs called follicles (100-300 micrometers in diameter)
- Each follicle is lined by a single layer of cuboidal (follicular) epithelial cells
- When the thyroid is active, these cells become columnar (tall); when inactive, they become flat
Colloid
- The hollow center of each follicle is filled with a thick, gel-like substance called colloid
- Colloid is made mostly of thyroglobulin - a large protein that is the storage form of thyroid hormones (T3 and T4)
- The hormones are stored here until the body needs them
C Cells (Parafollicular Cells)
- Scattered between follicles (NOT inside them)
- Produce calcitonin - a hormone that helps lower blood calcium levels
- These are the cells that give rise to medullary thyroid cancer
9. Embryology (Where the Thyroid Comes From)
The thyroid develops from two sources in the embryo:
- Median anlage - forms the main bulk of the thyroid; starts at the base of the tongue (at the foramen cecum) and descends down the neck via the thyroglossal duct
- Lateral anlage (ultimobranchial bodies) - contribute the C cells
The thyroglossal duct normally disappears. If it does not:
- Thyroglossal duct cyst forms in the midline neck (moves up when you stick out your tongue - a classic clinical sign)
- Lingual thyroid forms if the gland fails to descend at all
10. Neighboring Structures to Remember
| Structure | Relation to Thyroid |
|---|---|
| Trachea | Directly behind/posterior |
| Esophagus | Behind and slightly left |
| Carotid sheath (artery, vein, vagus) | Lateral to each lobe |
| Parathyroid glands | 4 tiny glands embedded in the back (posterior) of each thyroid lobe |
| Strap muscles | In front |
| Cricoid cartilage | Just above the isthmus |
Parathyroid Glands
- 4 glands (2 superior, 2 inferior), each the size of a grain of rice (~50 mg each)
- Sit on the posterior capsule of the thyroid
- Their blood supply comes from the inferior thyroid artery
- Must be identified and preserved during thyroid surgery to avoid hypoparathyroidism (low calcium)
Quick Summary in Simple Terms
The thyroid is a butterfly-shaped gland on the front of your windpipe below your Adam's apple. It has two lobes, a connecting bridge (isthmus), and sometimes a upward-pointing pyramid. Inside, it is packed with tiny sacs (follicles) full of thyroid hormone storage material (colloid). It has excellent blood supply from four arteries, drains through three sets of veins, and is closely guarded by important nerves that control your voice. Four tiny parathyroid glands sit on its back surface. Surgeons must know every millimeter of this anatomy because the margins for error are tiny.
Sources: Guyton & Hall Textbook of Medical Physiology | Schwartz's Principles of Surgery, 11th Ed. | Mulholland and Greenfield's Surgery, 7th Ed. | Current Surgical Therapy, 14th Ed. | Sabiston Textbook of Surgery
Where are diagrams
Finding Sources
Searching Content
"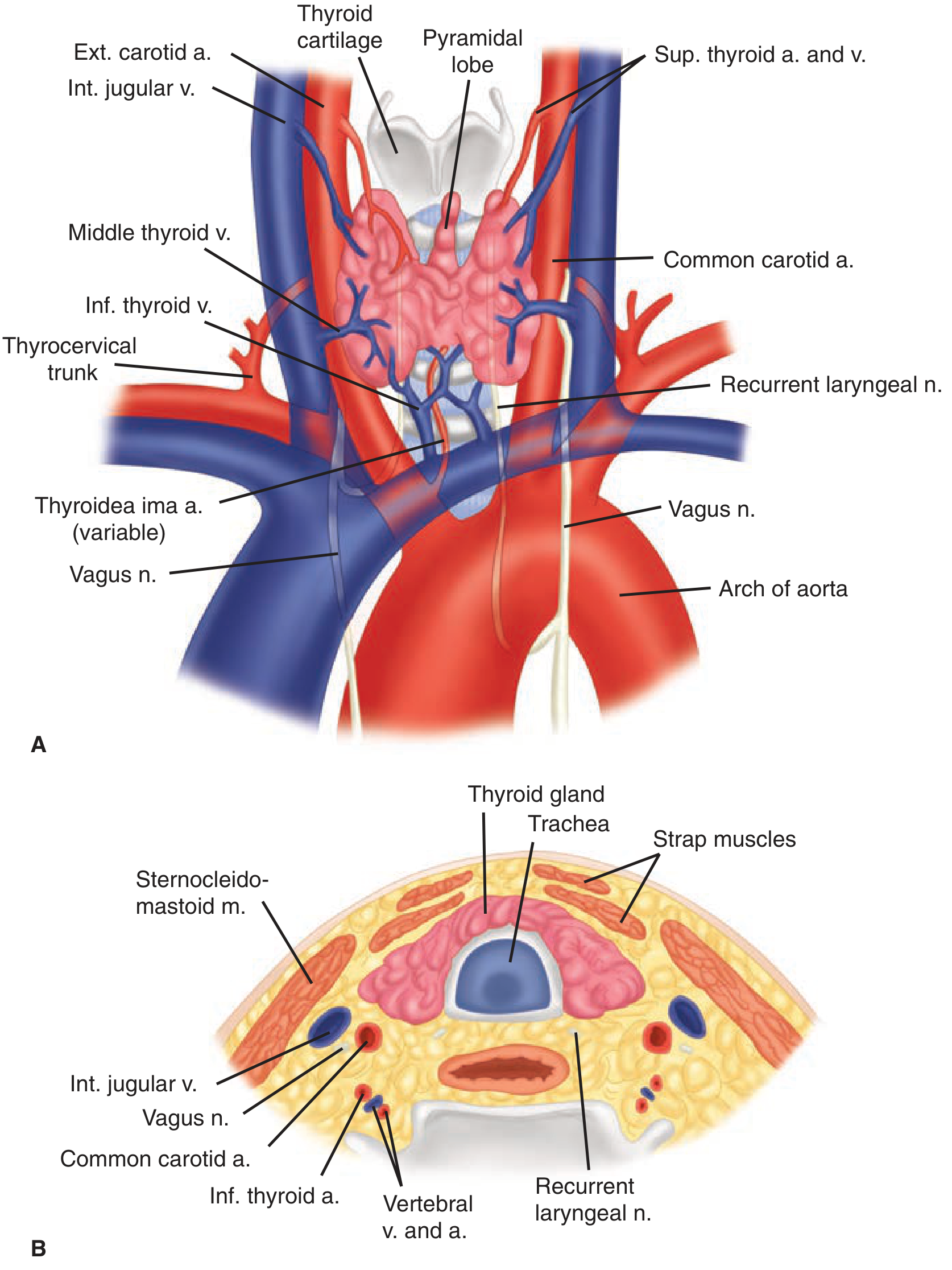
What this shows (top panel - anterior view):
- The pyramidal lobe projecting upward from the isthmus
- Superior thyroid artery and vein entering from the external carotid
- Inferior thyroid vein draining downward
- Thyrocervical trunk giving off the inferior thyroid artery
- Thyroidea ima artery (variable) from the aorta
- Both recurrent laryngeal nerves (right and left)
- The vagus nerves flanking the trachea
- Arch of aorta at the bottom
What this shows (bottom panel - cross-section of neck):
- Thyroid gland sitting in front of the trachea
- Strap muscles covering the gland anteriorly
- Internal jugular vein and common carotid artery on each side
- Recurrent laryngeal nerve in the groove between trachea and esophagus
- Sternocleidomastoid muscle laterally
Diagram 3 - Blood Supply & Nerve Detail (Gray's Anatomy for Students)
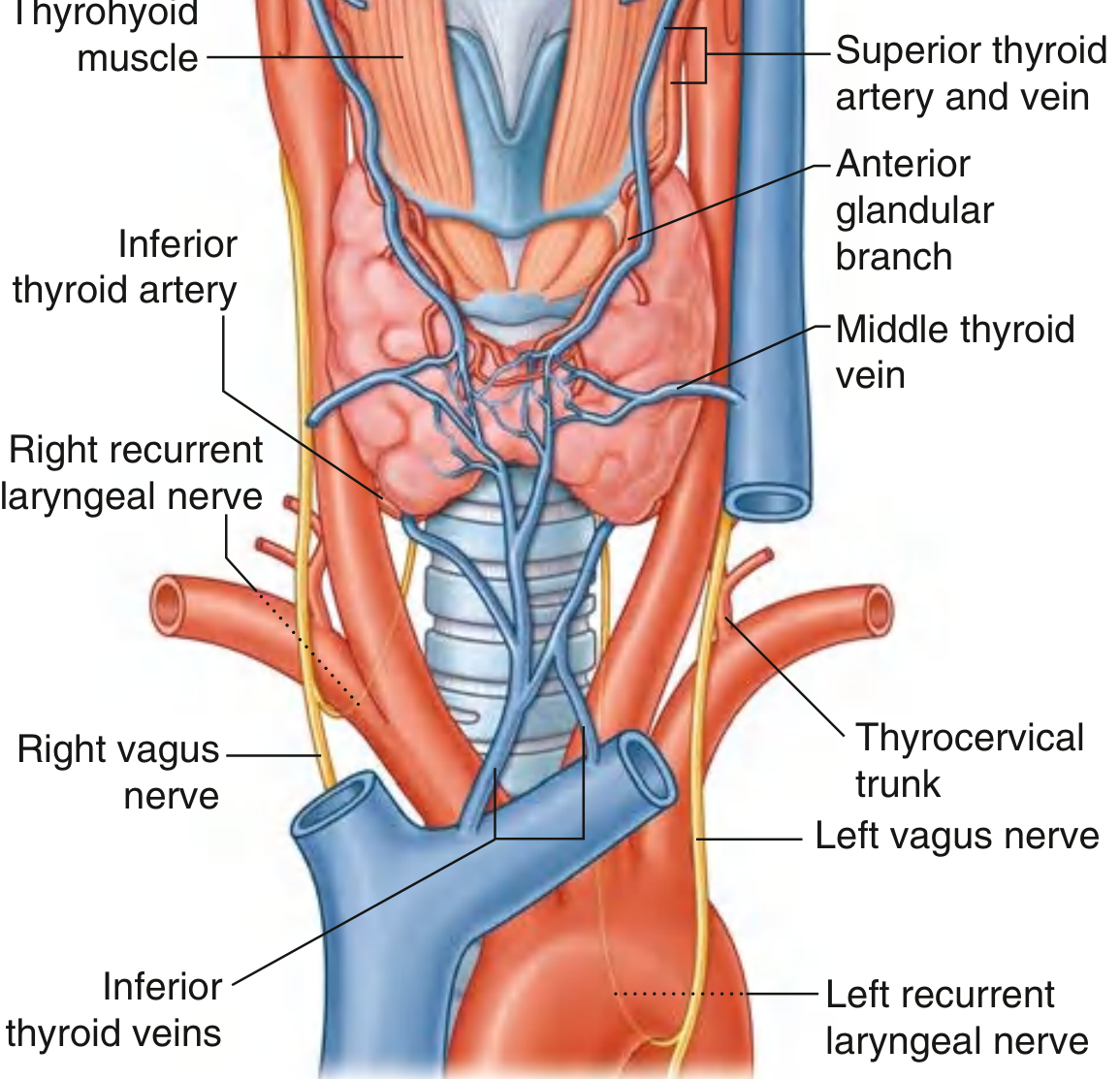
What this shows: Close-up of the thyroid's blood vessels - the superior thyroid artery and vein at the top, anterior glandular branch, middle thyroid vein draining laterally, inferior thyroid veins draining downward, the thyrocervical trunk, and both vagus nerves with the recurrent laryngeal nerves.
Diagram 4 - RLN Course & Origin (Current Surgical Therapy)
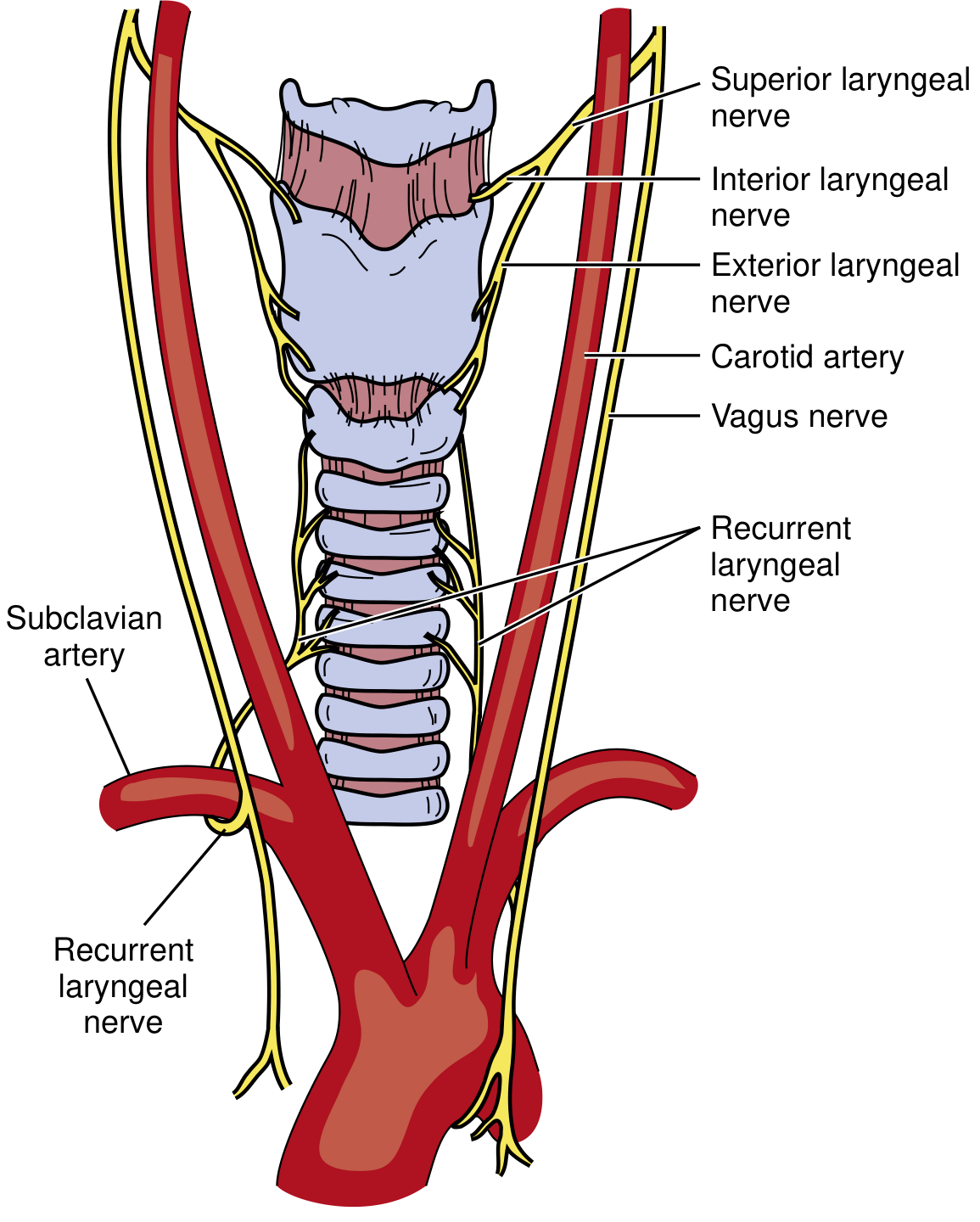
What this shows: How the recurrent laryngeal nerve (yellow) originates from the vagus nerve, loops under the subclavian artery on the right side, and the superior laryngeal nerve (interior and exterior branches) at the top.
Diagram 5 - RLN vs. Inferior Thyroid Artery Relationship
(Schwartz's Principles of Surgery - Fig. 38-3)
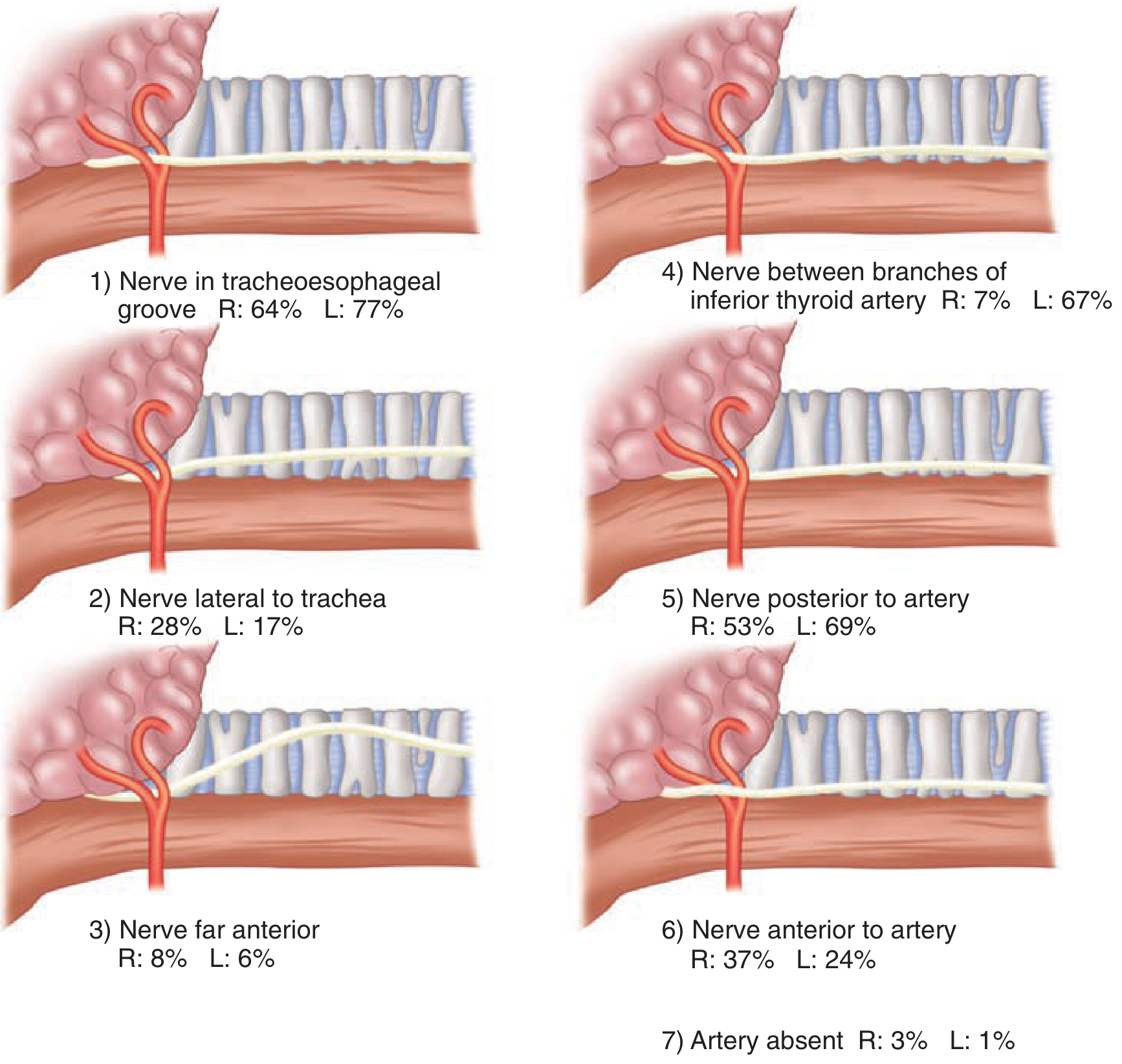
What this shows: The 6 possible ways the recurrent laryngeal nerve (RLN) can relate to the inferior thyroid artery - with the percentage frequency for right (R) and left (L) sides. This is critical surgical knowledge because the nerve can be:
- In the tracheoesophageal groove (most common)
- Lateral to the trachea
- Far anterior
- Between branches of the artery
- Posterior to the artery
- Anterior to the artery
This variability is exactly why surgeons must always visually identify the nerve before cutting the artery.
All five diagrams together cover every major aspect of thyroid anatomy - position, lobes, cross-section, blood supply, venous drainage, and nerve relationships. Sources: Guyton & Hall | Schwartz's Surgery | Gray's Anatomy for Students | Current Surgical Therapy.
This is a shared conversation. Sign in to Orris to start your own chat.