Cholicystectomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
cholecystectomy laparoscopic outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from both Bailey & Love and Schwartz's Principles of Surgery. Let me compose the full answer.
Cholecystectomy
Cholecystectomy is surgical removal of the gallbladder. It is one of the most common abdominal operations performed worldwide - over 750,000 per year in the United States alone.
History
- 1882 - Carl Langenbuch performed the first successful open cholecystectomy
- 1987 - Philippe Mouret (France) introduced laparoscopic cholecystectomy, which rapidly replaced the open approach and rendered non-surgical gallstone therapies (e.g., lithotripsy, bile salt dissolution) largely obsolete
Indications
- Symptomatic gallstones (biliary colic)
- Acute cholecystitis
- Chronic cholecystitis
- Empyema or gangrene of the gallbladder
- Gallstone pancreatitis
- Biliary dyskinesia (acalculous)
- Gallbladder polyps >1 cm (malignancy risk)
- Porcelain gallbladder (selected cases)
Preoperative Preparation
(Bailey & Love's Short Practice of Surgery, 28th Ed.)
- Full history (jaundice, previous biliary events) and fitness assessment
- Investigations: FBC, renal and liver function tests, prothrombin time; ECG/CXR if medically indicated
- Antibiotic prophylaxis: second-generation cephalosporin at induction of anaesthesia
- VTE prophylaxis: subcutaneous heparin + antiembolic stockings
- Informed consent (procedure, alternatives, specific risks)
- Bladder emptied before the operating room (avoids need for catheterisation)
Risk Stratification for CBD Stones
| CBD Stone Risk | History | LFTs | CBD diameter (USG) | Action |
|---|---|---|---|---|
| Low (2-3%) | No cholangitis/pancreatitis | Normal | ≤6 mm | None |
| Medium (20-40%) | Present | 2× normal | 8-10 mm | MRCP ± ERCP |
| High (50-80%) | Present + jaundice | 2× normal | ≥10 mm | MRCP ± ERCP |
Laparoscopic Cholecystectomy (Gold Standard)
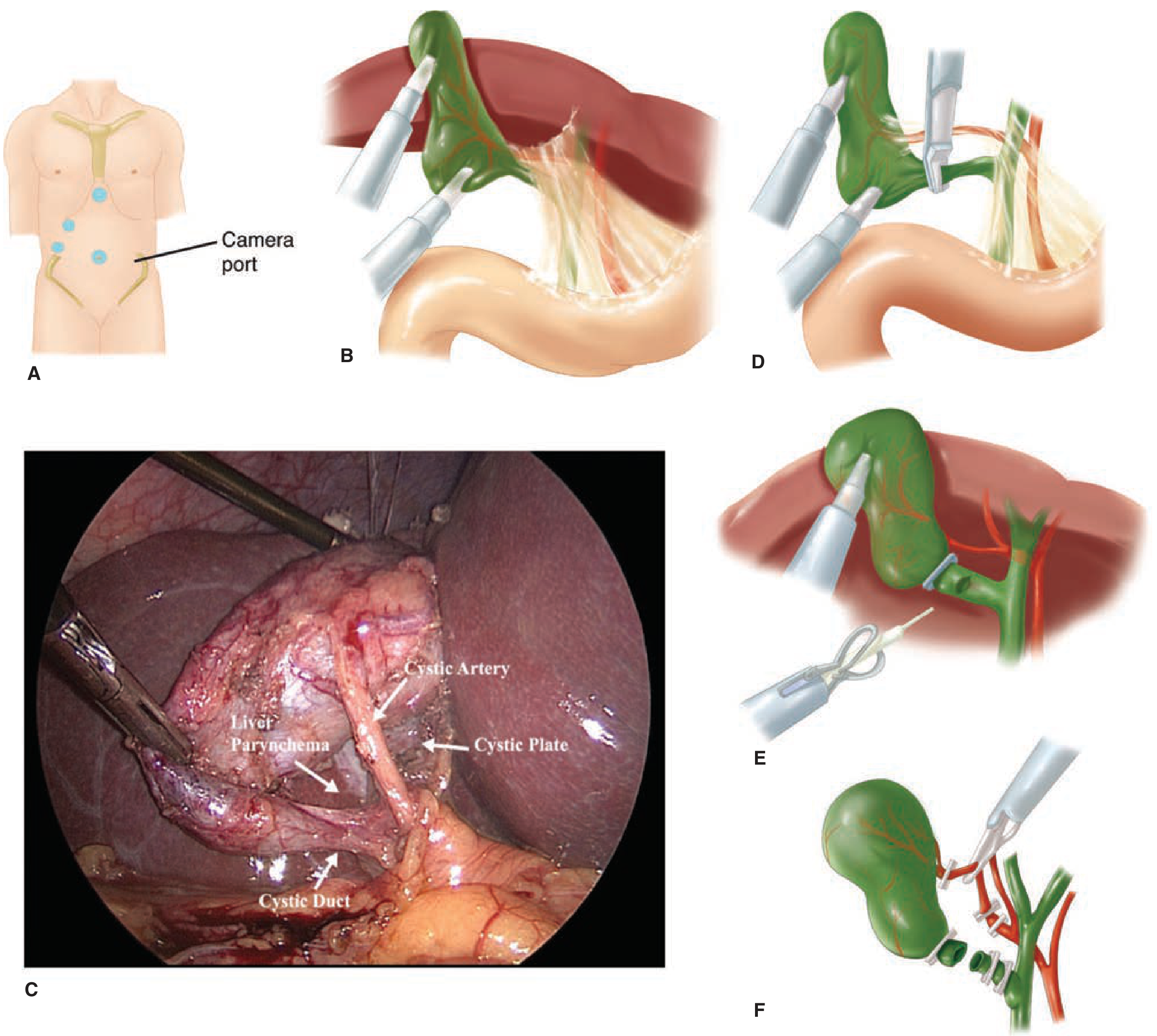
Figure: (A) Trocar placement - camera port at umbilicus, epigastric 10/12mm port, right midclavicular 5mm, right flank 5mm. (B) Fundus retracted cephalad. (C) Intraoperative "Critical View of Safety" showing cystic artery, cystic duct, cystic plate, and liver parenchyma. (D-F) Clipping and division of structures. (Schwartz's Principles of Surgery, 11th Ed.)
Patient Positioning & Access
- Supine; surgeon stands at patient's left (or between legs in split-leg position)
- Pneumoperitoneum with CO₂ via Veress needle (closed) or Hasson technique (open); typical pressure 12-15 mmHg
- Port placement:
- Supraumbilical (camera, 5- or 10-mm, 30° scope)
- Epigastric (10-12 mm, working port)
- Right midclavicular line (5 mm)
- Right flank (5 mm)
Step-by-Step Technique
- Retraction: Assistant grasps gallbladder fundus and retracts it cephalad over the liver edge toward the right shoulder
- Infundibulum exposure: Surgeon retracts gallbladder infundibulum posterolaterally to expose the hepatocystic triangle (triangle of Calot)
- Dissection: Peritoneum, fat, and areolar tissue around the cystic duct-gallbladder junction are dissected off. The cystic duct and cystic artery are carefully defined
- Critical View of Safety (CVS) - mandatory before any clipping:
- Hepatocystic triangle cleared of fat and fibrous tissue
- Lower one-third of gallbladder separated from liver to expose the cystic plate
- Only two structures seen entering the gallbladder (cystic duct and cystic artery)
- Cholangiogram (selective or routine): catheter inserted into cystic duct to image biliary tree
- ICG fluorescence cholangiography (modern): real-time imaging with indocyanine green for better bile duct visualisation
- Clipping and division: Two clips at the base, one on the gallbladder side for both cystic duct and cystic artery; then divide. For dilated cystic ducts - endoloop, laparoscopic stapler, or suture
- Dissection from liver bed: Electrocautery; watch for aberrant posterior bile ducts or vessels
- Final inspection: Check for bile leak, bleeding, clip placement
- Specimen retrieval: Usually through epigastric port, in retrieval bag; port may need enlargement for large stones
- Drain (optional): placed if severe inflammation, gangrene, or expected bile/blood accumulation
Safe Zones and Landmarks
Bailey & Love describes the B-SAFE method with five anatomical landmarks to orient the surgeon during dissection:
- B - Bile duct
- S - Sulcus of Rouvière (safe zone is cephalad to line from Rouvière's sulcus to umbilical fissure = R4U line)
- A - Hepatic artery
- F - Umbilical fissure
- E - Enteric (duodenum)
Calot's triangle (hepatocystic triangle) is bounded by the cystic duct, common hepatic duct, and the inferior surface of the liver. The cystic artery typically runs within it.
Contraindications to Laparoscopic Approach
Absolute:
- Haemodynamic instability
- Uncontrolled coagulopathy
- Frank peritonitis
- Severe COPD or heart failure (EF <20%) - unable to tolerate pneumoperitoneum
Relative / Risk factors for difficult cholecystectomy:
- Male, >65 years, acute cholecystitis >72-96 hours, prior upper abdominal surgery, morbid obesity, cirrhosis, pregnancy, thick-walled gallbladder (>4-5 mm), empyema, Mirizzi syndrome
Open Cholecystectomy
- Right subcostal (Kocher) incision or midline laparotomy
- Dissection usually begins at fundus, working toward the hepatocystic triangle
- Same surgical principles apply - CVS, cystic duct and artery identification, ligation, division
- "Fundus-first" (retrograde) approach useful when severe adhesions prevent antegrade dissection
- Indicated when laparoscopic approach fails or is contraindicated
Conversion to Open
- Elective setting: ~5% conversion rate
- Emergent/complicated: 10-30% conversion rate
- Not a failure - always discussed preoperatively
- Indications: inability to tolerate pneumoperitoneum, uncontrolled intraoperative complication, inability to identify anatomy, no progress after set time period
Intraoperative Cholangiogram (IOC)
- Performed selectively when biliary anatomy is unclear, or when CBD stones are suspected
- Catheter inserted into cystic duct before division; fluoroscopic imaging of biliary tree
- Identifies unsuspected CBD stones and confirms anatomy to prevent bile duct injury
Complications
(Schwartz's Principles of Surgery, 11th Ed.)
| Complication | Notes |
|---|---|
| Bile duct injury | Most feared - 0.3-0.5% (laparoscopic); decreasing with better technique and CVS adoption |
| Bile leak | From cystic duct stump, liver bed, or duct of Luschka |
| Haemorrhage | Cystic artery injury; port site |
| Wound/port site infection | Less common than open surgery |
| Retained CBD stones | Missed stones causing post-op jaundice/cholangitis |
| Bowel injury | Rare; thermal or mechanical |
| Port site hernia | Fascial defects >10mm should be closed |
| Spilled gallstones | Intra-abdominal abscess; must be retrieved if possible |
| Deep vein thrombosis/PE | Reduced by VTE prophylaxis |
| Postcholecystectomy syndrome | Persistent symptoms post-op (bile salt diarrhoea, retained stones, biliary dyskinesia) |
Mortality: ~0.1% for laparoscopic cholecystectomy.
Difficult Cholecystectomy: Safety Steps
(Bailey & Love)
- "Dome-down" (fundus-first) technique - when severe adhesions at Calot's triangle; start at fundus and work down
- Partial/subtotal cholecystectomy - leave gallbladder base when complete removal is dangerous; oversew the remnant
- Cholecystostomy - tube drainage as temporising measure in high-risk patients
- Time-out concept - procedural pause when disoriented to recall and apply safety measures
- Convert early - conversion to open is not a failure; hesitation increases risk
Post-operative Care
- Day-case or overnight stay for elective laparoscopic cases
- Early ambulation
- Diet resumed when tolerating oral intake
- Analgesics (paracetamol + NSAIDs; opioids if needed)
- Discharge instructions: wound care, activity restrictions, when to seek review
Recent Evidence
A 2025 meta-analysis (Qadri et al., J Robot Surg, PMID 41354898) comparing robotic vs. laparoscopic cholecystectomy found comparable outcomes, with robotic approaches offering some ergonomic advantages. A 2024 meta-analysis (Edebo et al., Surg Endosc, PMID 39020122) evaluated laparoscopic ultrasonography vs. intraoperative cholangiography, finding similar diagnostic accuracy for bile duct injuries.
Sources: Schwartz's Principles of Surgery, 11th Ed., p. 1438-1439 | Bailey & Love's Short Practice of Surgery, 28th Ed., p. 1270-1272 | Sleisenger & Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.