Detailed stem cell therapy in rheumatology from rheumatology textbooks(Kelley and hochberg) and major journals
"stem cell therapy" AND rheumatic diseases
"hematopoietic stem cell transplantation" AND "systemic sclerosis"
"mesenchymal stem cell" AND "lupus" OR "rheumatoid arthritis"
"mesenchymal stem cell transplantation" AND "systemic lupus erythematosus"
PMID: 35285885
PMID: 39934871
PMID: 40353645
PMID: 40169165
PMID: 38737817
"CAR-T" OR "CAR T cell" AND "autoimmune" OR "rheumatology"
PMID: 37748491
Stem Cell Therapy in Rheumatology
Overview
1. Types of Stem Cells Used
Hematopoietic Stem Cells (HSCs)
- Myeloablative: uses high-dose chemotherapy ± total body irradiation (TBI) to completely ablate the marrow
- Non-myeloablative (immunoablative): less intensive conditioning, preserves some marrow function, lower treatment-related mortality (TRM)
Mesenchymal Stem Cells (MSCs)
- Suppression of T-cell proliferation and activation
- Promotion of regulatory T cell (Treg) differentiation
- Inhibition of Th17 cells
- Paracrine anti-inflammatory cytokine secretion (TGF-β, IL-10, PGE2)
- Direct cell-cell contact via PDL1 and Fas-FasL
- Differentiation potential into cartilage, bone, and fat
2. Autologous HSCT in Systemic Sclerosis (SSc) - The Landmark Data
ASTIS Trial (Autologous Stem Cell Transplantation International Scleroderma)
- Design: European multicenter RCT comparing autologous non-myeloablative HSCT vs. monthly IV cyclophosphamide (CYC) x12 months in early diffuse cutaneous SSc
- Key results: Despite higher early transplant-related mortality, HSCT showed superior long-term event-free and overall survival
- HSCT rapidly controlled skin disease (mRSS), stabilized lung function (FVC), and improved quality of life
ASSIST Trial (American Scleroderma Stem Cell versus Immune Suppression Trial)
- Design: Small, single-site US RCT comparing non-myeloablative HSCT vs. IV CYC x6 months
- Key results: Highly promising; confirmed improvement in skin and lung; limited by small size and short follow-up; included patients with milder disease
SCOT Trial (Scleroderma Cyclophosphamide Or Transplantation)
- Design: US multicenter RCT - myeloablative HSCT (n=36) vs. CYC (n=39); unique addition of total body irradiation (TBI) to conditioning; CYC was NOT used for stem cell mobilization
- Primary endpoint: Global Rank Composite Score (GRCS) - hierarchy of death, event-free survival, FVC, HAQ-DI, mRSS
- Results at 54 months: 67% of pairwise comparisons favored HSCT vs. 33% favoring CYC (p=0.01)
- At 72 months: Event-free survival 74% (HSCT) vs. 47% (CYC); overall survival 86% vs. 51% (p=0.03 and 0.02)
- TRM: 3% at 54 months, 6% at 72 months in transplant group; 0% in CYC group
Hochberg/Rheumatology 2022 Perspective
- Patient selection is "extremely challenging" - patients must be sick enough to need transplant yet well enough to tolerate TRM
- Long-term organ effects remain unclear
- A systematic review/meta-analysis concluded HSCT should only be performed at specialty centers in high-risk early-stage patients with lung and diffuse skin involvement
- Guidelines defining sequential order of treatments in SSc are still warranted
Meta-Analysis (Higashitani et al., 2023 - PMID 35285885)
- HSCT significantly improved skin thickness (mRSS) and lung function
- Kaplan-Meier analysis showed high 2-year post-transplant survival (log-rank p=0.004)
- Pooled transplant-related death rate: 6.30% (95% CI 4.21-8.38%) - but this has been declining over the past decade
- Conclusion: HSCT is effective for SSc; optimal indications must carefully balance risks
3. HSCT in Systemic Lupus Erythematosus (SLE)
Autologous HSCT
- Non-myeloablative or myeloablative conditioning followed by autologous HSC rescue
- Demonstrates complete clinical remission or reduction of disease activity in 30-70% of patients
- Decreases anti-dsDNA antibodies, ANA titers
- Improves Th1/Th2 ratio (favoring Th2) and Th17/Treg balance (favoring Treg)
- Complications: infection, secondary autoimmune disease, recurrence
Allogeneic MSC Transplantation in SLE
- Allogeneic MSCs derived from umbilical cord or bone marrow infused IV in refractory SLE
- Significant reduction in SLEDAI scores and anti-dsDNA
- Improved renal function in lupus nephritis
- Meta-analysis (Zeng et al., 2025; 42 RCTs, 2183 participants) confirmed: MSC transplantation significantly improved SLEDAI (SMD = -2.32; 95% CI -3.59 to -1.06; p=0.0003) without increasing adverse events (RR=0.83; p=0.76)
4. HSCT in Juvenile Idiopathic Arthritis (JIA) - Hochberg Textbook Data
- Autologous HSCT (Netherlands cohort - largest series): Used predominantly for systemic JIA
- Complete drug-free remission: ~50%
- Partial response (Pediatric ACR criteria): ~20%
- No improvement: ~20%
- Allogeneic HSCT (16 patients; systemic arthritis n=11, RF-negative polyarthritis n=5):
- 80% (11/14) achieved complete drug-free remission at last follow-up
- Long-term follow-up required
- Mortality: ~10% for either autologous or allogeneic SCT
- Viral infections post-SCT: high incidence
- Status: Still considered experimental; reserved for severe, unremitting disease despite all modern therapies including biologics (anti-IL-1, anti-IL-6)
5. HSCT in Osteonecrosis
Pathophysiology rationale
- Corticosteroids shift mesenchymal stem cell differentiation from osteogenesis toward adipogenesis in bone marrow
- Also reduce VEGF → decreased angiogenesis → bone death
- Alcohol has a similar effect on progenitor cell differentiation
Clinical evidence
-
Pilot study: Core decompression + autologous bone marrow cell implantation vs. core decompression alone
- At 24 months: 5/8 control hips progressed to stage 3 vs. only 1/10 treatment hips
- Greater improvement in pain and joint symptoms in treatment group
-
28-patient series (44 necrotic hips): Percutaneous decompression + autologous bone marrow mononuclear cell infusion
- Minimum 2-year follow-up
- Mean Harris Hip Score improved from 58 to 86
- Slowing of disease stage progression
-
2014 literature review: Core decompression + MSC infusion leads to improved pain and function, halts progression of osteonecrosis, potentially avoids total hip replacement
-
Updated evidence: Bone marrow MSC transplantation with core decompression lowered total hip replacement conversion rate vs. core decompression alone (though no impact on ARCO staging)
6. MSC Therapy in Rheumatoid Arthritis (RA)
- MSCs suppress synovial inflammation by inhibiting T-cell proliferation and inducing Treg expansion
- In animal models: reduction of joint swelling, bone erosion, and inflammatory cytokines
- Clinical trials have shown improvements in DAS28, VAS pain, and inflammatory markers
- Meta-analysis (Zeng 2025): MSC transplantation may improve spondyloarthritis and RA (systematic review; RCT evidence limited)
- Review (Hetta et al., 2025): MSC therapy in RA shows potential for symptom relief and disease progression delay; challenges include variability in response, optimal cell source/dosing, and long-term safety
7. MSC Therapy in Osteoarthritis (OA)
Cochrane Review (Whittle et al., 2025 - PMID 40169165)
- 25 RCTs (1341 participants) comparing stem cell injections vs. placebo, hyaluronic acid, PRP, and others
- vs. placebo (8 trials, 445 participants):
- Pain (0-10 scale): 1.2 points better with stem cells vs. placebo
- Function (0-100 scale): 14.2 points better with stem cells
- High heterogeneity (I² = 80-82%)
- Very low certainty evidence overall
- Most trials were small (6-252 participants); only 2 had >100 participants
- Placebo-controlled trials largely free from bias; open-label trials susceptible to performance bias
Meta-Analysis on MSCs in OA (Zeng 2025)
- Bone marrow MSC (SMD = -0.95; 95% CI -1.55 to -0.36; p=0.002) - VAS pain reduction
- Umbilical cord MSC (SMD = -1.25; 95% CI -2.04 to -0.46; p=0.002)
- Adipose-derived MSC (SMD = -1.26; 95% CI -1.99 to -0.52; p=0.0009)
- No increase in adverse events (RR=1.23; p=0.15)
8. MSC Therapy in Systemic Sclerosis (SSc)
- Zare Moghaddam et al. (2023): MSC therapy in SSc - showed potential for modulating fibroblast activation and reducing fibrosis in preclinical models
- The 2025 meta-analysis (Zeng): MSC transplantation may NOT improve symptoms of systemic sclerosis based on available RCT evidence - distinguishing it from HSCT where the evidence is strong
- MSCs in SSc remain investigational, with ongoing trials
9. MSC Therapy in Sjögren's Syndrome
- MSCs derived from umbilical cord administered IV to primary Sjögren's patients
- Results: improvement in dry eye/dry mouth symptoms, salivary flow rates, parotid biopsy lymphocytic foci
- Increased Treg cells, decreased Th17 cells
- Meta-analysis: MSC may improve primary Sjögren's syndrome
- 2024 review (Lu et al., PMID 39438246): Cell therapy offers opportunities but faces challenges in standardization and durability
10. CAR-T Cell Therapy - The Emerging Frontier
Rationale
- Autoreactive B cells are pathogenic in SLE, RA, and other autoimmune diseases
- Rituximab (anti-CD20) has poor efficacy in autoimmune disease because autoreactive B cells persist in lymphatic organs and inflamed tissues (inaccessible to antibody)
- CAR-T cells, engineered to express chimeric antigen receptors against B cell antigens, can traffic to these sites
CD19 CAR-T in Autoimmune Disease
- Anti-CD19 CAR-T cells (targeting all B cells) administered to patients with refractory SLE and dermatomyositis
- Results: rapid and sustained depletion of circulating B cells + complete clinical and serological remission
- Unlike in cancer (where CAR-T causes prolonged B-cell aplasia), immune reconstitution occurred with reappearance of "naive" non-autoreactive B cells post-depletion
- This "deep immune reset" mechanism parallels HSCT but with targeted B-cell elimination
Key Applications
- Refractory SLE (anti-dsDNA normalization, lupus nephritis remission)
- Dermatomyositis (muscle enzyme normalization)
- Early data in systemic sclerosis and RA
11. Mechanisms of Action Summary
| Mechanism | HSCT | MSC | CAR-T |
|---|---|---|---|
| Immune ablation/reset | ✓ (core) | - | Partial (B-cell) |
| Immunomodulation (Treg↑) | Secondary | ✓ (primary) | - |
| Th17 suppression | ✓ | ✓ | - |
| Anti-fibrotic | Indirect | ✓ Direct | - |
| Tissue regeneration | - | ✓ | - |
| B-cell depletion | ✓ (full) | - | ✓ (targeted) |
12. Patient Selection Criteria and Indications
HSCT (SSc) - Current Criteria from Textbooks
- Early diffuse cutaneous SSc (within 2-4 years of non-Raynaud onset)
- Rapidly progressive skin (mRSS >15) or significant internal organ involvement
- Contraindicated/high-risk: severe pulmonary hypertension, renal crisis, LVEF <45%, established end-organ damage
- Must be performed at specialty centers with HSCT expertise
- Patient must be "sick enough to need transplant yet well enough to tolerate TRM"
HSCT (JIA)
- Severe, unremitting disease despite all modern therapies including anti-IL-1, anti-IL-6
- Considered experimental
MSC therapy
- Refractory SLE after conventional immunosuppressives
- OA not responding to conventional management
- Generally investigational except in select programs
13. Risks and Complications
| Complication | HSCT | MSC |
|---|---|---|
| Transplant-related mortality | ~6% SSc (pooled); ~10% JIA | Very low |
| Infections (viral/fungal) | High (especially post-allogeneic) | Low |
| Secondary autoimmune disease | Reported | Rare |
| Disease recurrence | Yes | Yes |
| Graft failure | Yes (allogeneic) | N/A |
| Engraftment syndrome | Yes | - |
| Tumor risk | Rare (long-term) | Being monitored |
14. Current Status and Future Directions
- HSCT for SSc is the most evidence-supported stem cell therapy in rheumatology, backed by 3 large RCTs (ASTIS, ASSIST, SCOT), with long-term survival benefit demonstrated (Kelley/Firestein)
- MSC therapy for SLE and OA shows promising signal from multiple RCTs but evidence quality remains low-to-moderate
- CAR-T cell therapy represents the most transformative new approach - early human data is remarkable but follow-up is short and scale is small
- Ongoing challenges (Hetta 2025): variability in MSC sources (BM vs. adipose vs. umbilical), dosing protocols, timing, patient heterogeneity, regulatory hurdles
- The field is moving toward: combination strategies (e.g., HSCT followed by CAR-T), genetically modified MSCs, and extracellular vesicle (exosome)-based therapy as a cell-free alternative
Key References
- Firestein & Kelley's Textbook of Rheumatology (9780323935364) - Chapters on SSc management, osteonecrosis, autoinflammatory diseases
- Rheumatology, 2-Volume Set (Hochberg/Elsevier, 2022; 9780702081330) - Chapters on SSc skin, JIA, SLE
- Higashitani K et al. Benefits and risks of HSCT for systemic sclerosis: systematic review and meta-analysis. Mod Rheumatol 2023. [PMID: 35285885]
- Zeng L et al. Efficacy and safety of MSC transplantation in autoimmune/rheumatic diseases: systematic review and meta-analysis of 42 RCTs. Stem Cell Res Ther 2025. [PMID: 39934871]
- Whittle SL et al. Stem cell injections for osteoarthritis of the knee (Cochrane Review). Cochrane Database Syst Rev 2025. [PMID: 40169165]
- Schett G, Mackensen A, Mougiakakos D. CAR T-cell therapy in autoimmune diseases. Lancet 2023. [PMID: 37748491]
- Hetta HF et al. Clinical Progress in MSC Therapy: A Focus on Rheumatic Diseases. Immun Inflamm Dis 2025. [PMID: 40353645]
- Zare Moghaddam M et al. Stem cell-based therapy for SLE. J Transl Autoimmun 2024. [PMID: 38737817]
- Keyes-Elstein L et al. Clinical and Molecular Findings After Autologous SCT or CYC for Scleroderma (SCOT trial analysis). Arthritis Care Res 2023. [PMID: 34533286]
Bispecific T cell engagers in autoimmune diseases. From rheumatology textbooks(Kelley and hochberg) and major journals
"bispecific T cell engager" AND autoimmune
bispecific antibody AND "rheumatoid arthritis" OR "lupus" OR "systemic sclerosis"
PMID: 42002248
PMID: 41694371
PMID: 40746557
blinatumomab OR "CD19xCD3" OR "BCMA bispecific" AND "lupus" OR "myositis" OR "systemic sclerosis" OR "Sjogren"
"teclistamab" OR "mosunetuzumab" OR "odronextamab" AND autoimmune
"bispecific" AND "CD3" AND "CD19" AND "autoimmune" OR "lupus" OR "myositis"
PMID: 42002248
PMID: 38642912
PMID: 41951534
blinatumomab AND "lupus" OR "systemic sclerosis" OR "rheumatoid arthritis"
"BCMA" AND "bispecific" AND autoimmune OR "plasma cell" AND autoimmune
Bispecific T Cell Engagers (BiTEs) in Autoimmune Diseases
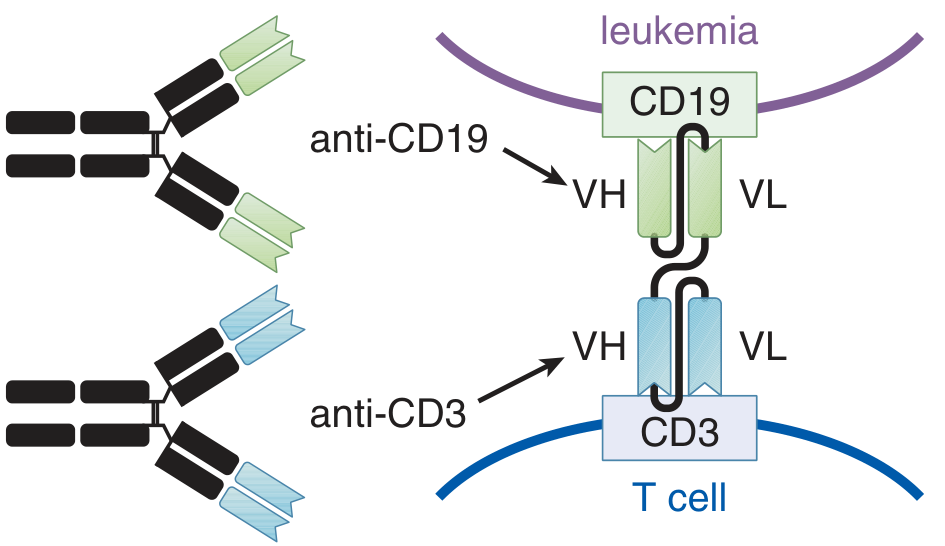
1. Definition and Molecular Architecture
2. Textbook Coverage - Hochberg/Elsevier Rheumatology 2022
The Rationale for Bispecific Approaches
- Limitation of anti-CD20 monotherapy (rituximab): After rituximab, B-cell depleting activity triggers a significant rise in B-cell activating factor (BAFF) in patients with RA and SLE - which drives B-cell repopulation and may facilitate tissue B-cell survival
- This creates a strong rationale for combination or bispecific approaches that simultaneously target B cells and their survival signals
- Phase 3 trials of rituximab + belimumab combination were ongoing in SLE at time of publication
Bispecific Antibody Formats Described
- Bispecific IgG: Each of the two Fab fragments carries different target specificity
- VH/VL fragment combinations (reviewed in Schmid and Neri)
- Fynomers: Antibody mimetics - Fyn SH3 domain modified to recognize a specific protein, linked to a conventional antibody
Bispecific in Rheumatology: Status at 2022
- COVA322: Bispecific TNF-α/IL-17 fusion protein (FynomAb) - well tolerated preclinically, but clinical trial in psoriasis terminated prematurely
- IL-6/IL-17 FynomAb: Under development (Lyman et al., 2018 - a bispecific antibody targeting both IL-6R and IL-17A for autoimmune/inflammatory diseases)
- Biological therapies have transformed rheumatic disease management; bispecific structures offer new opportunities to modulate pharmacokinetic and pharmacodynamic profiles
3. Mechanism of Action in Autoimmune Disease
Why target B cells in autoimmune disease?
- Production of autoantibodies (anti-dsDNA, anti-CCP, ANA, anti-Jo-1, etc.)
- Antigen presentation to T cells
- Cytokine secretion (IL-6, IL-10, LT-α)
- Formation of ectopic lymphoid structures in inflamed tissues
Why conventional B cell depletion fails in some patients
- Rituximab (anti-CD20) fails in refractory AID due to persistence of:
- IgD-CD27+ switched memory B cells (rituximab-resistant)
- CD19+CD20- B cells (not targeted by anti-CD20)
- Long-lived plasma cells (CD20-negative; express CD19)
- B-T cell collaboration occurs predominantly in lymphoid tissues and inflamed sites (joint, kidney) where B-cell depletion by rituximab is inefficient due to poor effector cell access
How BiTEs overcome these limitations
- CD19-targeting BiTEs: Cover the full B cell lineage including memory B cells and plasmablasts (CD19 is expressed throughout B cell development, unlike CD20 which is lost at plasma cell stage)
- BCMA-targeting BiTEs: Target long-lived plasma cells - the source of persistent autoantibodies - which are CD20-negative but BCMA-positive
- CD20-targeting BiTEs (mosunetuzumab, glofitamab, epcoritamab): May provide deeper B-cell depletion than anti-CD20 monoclonal antibodies alone through T-cell mediated killing
4. BiTEs vs. CAR-T Cells: Key Differences
| Feature | BiTEs | CAR-T |
|---|---|---|
| Requires T cell engineering | No | Yes |
| Requires lymphodepletion | No | Yes |
| Off-the-shelf availability | Yes (allogeneic) | Limited (autologous usually) |
| Duration of action | Short (drug-dependent) | Long (months-years of persistence) |
| B cell depletion depth | Moderate-deep | Very deep |
| Plasma cell depletion | With BCMA-BiTE | With BCMA-CAR-T |
| Long-term immune reset | Less likely | More likely |
| Administration | IV infusion (often continuous) | Single infusion |
| Cost and accessibility | Lower | Higher |
| CRS risk | Yes (lower grade typically) | Yes (potentially higher grade) |
| Neurotoxicity | Rare in autoimmune use | Yes (ICANS) |
5. Key BiTE Agents and Their Targets
A. CD19 × CD3 BiTEs
- Approved 2014 for B-cell precursor ALL and minimal residual disease
- MW: ~54 kDa (much smaller than IgG ~150 kDa)
- Short half-life requires continuous IV infusion
- Targets CD19 on ALL blasts; in autoimmune use, targets autoreactive B cells
- Results in lysis of CD19+ cells, inflammatory cytokine release, T-cell proliferation
- Major adverse effects: cytokine release syndrome (CRS), neurological toxicities, neutropenic fever, sepsis
- From Goodman & Gilman's, block 19, line 4478; Katzung, line 1110
B. CD20 × CD3 BiTEs
- Mosunetuzumab, glofitamab, epcoritamab - approved in lymphoma, now being studied in autoimmune disease
- Cover CD20+ B cells including naive and memory B cells
- Do not reach plasma cells
C. BCMA × CD3 BiTEs
- Teclistamab (approved for multiple myeloma): One arm binds BCMA on plasma cells, other arm binds CD3 on T cells
- BCMA (B-cell maturation antigen) is expressed on long-lived plasma cells - the source of pathogenic autoantibodies in SLE, RA, SSc, and myositis
- Critical for diseases driven by persistent plasma cell-derived autoantibodies
- Other BCMA-directed BiTEs: elranatamab, linvoseltamab (oncology-approved)
- Katzung's Basic and Clinical Pharmacology, line 1058
D. Dual-cytokine targeting BiTEs (non-TCE)
- COVA322 (TNF-α/IL-17 FynomAb): Terminated in psoriasis trial
- IL-6R/IL-17A bispecific (Lyman 2018): Still in development
- These are not T-cell engagers per se, but bispecific cytokine/receptor targeting molecules
- Rheumatology (Hochberg 2022), block 8, lines 5523-5526
6. Clinical Evidence in Rheumatic Diseases
| Disease | n (patients) | Common TCE used |
|---|---|---|
| SLE | 33 | Blinatumomab, mosunetuzumab |
| RA | 22 | Blinatumomab |
| SSc | 14 | Blinatumomab, teclistamab |
| IIM (myositis) | 6 | Various |
| Primary Sjögren's | 2 | Various |
| Other | 3 | Various |
Clinical Outcomes
- Early signs of clinical improvement observed: rapid disease activity reduction, improvement in organ-specific manifestations, normalization of serologic biomarkers
- However: persistent or recurrent disease activity after treatment discontinuation in many patients
- Substantial heterogeneity in dosing strategies
- Lower cumulative exposure and shorter treatment duration vs. oncology regimens suggests potential undertreatment contributing to disease recurrence
Safety Profile (from 80 patients)
- CRS: 46% overall
- Grade 1: 33%
- Grade 2: 12%
- Grade 3: 1%
- No neurotoxicity (ICANS) reported in any autoimmune patient
- No deaths reported related to TCE treatment
- Notably safer profile than CAR-T cells in this population
7. Disease-Specific Evidence
Systemic Lupus Erythematosus (SLE)
-
Blinatumomab in SLE: Case reports and small series showing:
- Rapid reduction in anti-dsDNA titers
- Improvement in SLEDAI scores
- Improvement in proteinuria in lupus nephritis
- B-cell depletion more complete and durable than rituximab in some patients
-
Rationale for BCMA BiTEs in SLE: Long-lived plasma cells in bone marrow persist despite rituximab and sustain anti-dsDNA production. Teclistamab-type BCMA-directed BiTEs can target these cells, potentially providing more durable autoantibody reduction.
-
Ongoing trials: Multiple phase I/II studies evaluating TCEs in refractory SLE (ClinicalTrials.gov)
Rheumatoid Arthritis (RA)
- Anti-CCP (ACPA) and RF produced by synovial plasma cells
- Rituximab resistance in RA partly due to synovial tissue B-cell and plasma cell persistence
- TCEs can potentially access the synovium where conventional B-cell depleting antibodies have limited penetration
- Early results suggest DAS28 reduction and normalization of ACPA in some patients
Systemic Sclerosis (SSc)
- SSc is driven by autoantibodies (anti-topoisomerase I, anti-centromere, anti-RNA polymerase III) and fibroblast activation
- CD19+ B cells and plasmablasts in SSc promote TGF-β-mediated fibrosis
- BiTE therapy may address the B-cell/plasma cell axis without requiring HSCT
- Initial reports: skin score improvement, stabilization of pulmonary fibrosis
Idiopathic Inflammatory Myopathies (IIM)
- MSAs (anti-Jo-1, anti-Mi-2, anti-MDA5, anti-SRP) are pathogenic autoantibodies from plasma cells
- Rituximab has variable efficacy (limited by plasma cell persistence)
- Groener and Paik (Front Immunol, 2025 [PMID: 40746557]) highlight BCMA-targeted BiTEs as promising given that both plasmablasts and plasma cells contribute to MSA production
- CD19 CAR-T in myositis/SSc (Cell, 2024 [PMID: 39013470]): Allogeneic CD19-directed CAR-T in severe myositis and SSc demonstrated efficacy - data extrapolated to BiTE strategy
Primary Sjögren's Syndrome (pSS)
- Anti-Ro/SSA and anti-La/SSB autoantibodies
- Ectopic lymphoid structures (germinal center-like structures in salivary glands) are sites of local B-cell activation resistant to systemic therapies
- TCEs might better access these sites via T-cell trafficking
8. Comparison with Other B-Cell Targeting Strategies
| Strategy | Target | Plasma cells | Tissue access | Reversibility |
|---|---|---|---|---|
| Rituximab (anti-CD20) | CD20+ B cells | No | Limited | Yes |
| Belimumab (anti-BAFF) | BAFF ligand | Partial | Systemic | Yes |
| Obinutuzumab (anti-CD20) | CD20+ B cells | No | Better than rituximab | Yes |
| BiTE (CD19xCD3) | CD19+ B cells + plasmablasts | Partial | T cell-mediated | Yes (on drug) |
| BiTE (BCMAxCD3) | Plasma cells | Yes (BCMA+) | T cell-mediated | Yes (on drug) |
| CAR-T (anti-CD19) | CD19+ B lineage | Partial | Deep | No (persists) |
| CAR-T (anti-BCMA) | Plasma cells | Yes | Deep | No (persists) |
| HSCT | Full immune reset | Yes | N/A | No |
9. Advantages and Challenges
Advantages of BiTEs over CAR-T in autoimmune disease
- No need for T-cell engineering: Off-the-shelf availability; faster access
- No lymphodepletion required: Avoids chemotherapy-related toxicity and prolonged cytopenias
- Lower cost: Significant cost reduction compared to individualized CAR-T manufacturing
- Controllability: Short half-life means effects are reversible when drug is stopped (unlike persistent CAR-T cells)
- Comparable B/plasma cell depletion depth in early data
- Lower neurotoxicity: No ICANS reported in autoimmune BiTE use to date
Challenges and Limitations
- Shorter exposure and possible undertreatment: Optimal dosing for autoimmune disease (vs. higher cancer doses) not yet defined
- Disease recurrence after discontinuation: Without long-term immune reset, B cells may reconstitute with autoreactive repertoire
- CRS risk: 46% overall; requires monitoring and management protocols
- No established dosing protocols for autoimmune indications
- Very small patient numbers in current evidence (total n=80 patients across all autoimmune diseases)
- Short follow-up: Durability of response unclear
- Access to tissue-resident plasma cells: Long-lived plasma cells in bone marrow niches may not be fully eliminated
- Regulatory status: Not approved for any autoimmune indication as of 2026; all use is investigational or compassionate
- CRS management requires corticosteroids + IL-6 blockade, which further increases infection risk (Harrison's 22e, block 8, line 2212)
10. Key Mechanistic Distinction: BiTEs vs. Rituximab
- BAFF rises significantly in RA and SLE patients
- This drives B-cell repopulation
- Hence combination (rituximab + belimumab) or bispecific strategies are theoretically superior
- Depleting B cells and plasmablasts (via CD19)
- Depleting long-lived plasma cells (via BCMA)
- Not being dependent on ADCC or complement (which are blocked in hypogammaglobulinemic patients)
- Accessing tissue sites of B-T cell collaboration via T-cell homing
11. Ongoing and Future Directions
- Dedicated autoimmune BiTE trials: Phase I/II studies of blinatumomab, mosunetuzumab, and teclistamab in SLE, SSc, and myositis are enrolling
- Optimal dosing strategy: Lower doses than oncology? Continuous vs. intermittent? Subcutaneous formulations being developed
- Combination approaches: BiTEs + BAFF/APRIL inhibition to prevent B-cell reconstitution
- Treg-engaging bispecifics: CD3 × CD25 constructs to expand regulatory T cells rather than deplete B cells
- FcRn-directed bispecifics: To enhance clearance of circulating autoantibodies
- Tri-specific engagers: Simultaneously targeting T cells, B cells, and a third immunomodulatory target
- Non-T cell engagers: IL-6/IL-17 bispecifics (Lyman 2018 concept) for inflammatory/fibrotic rheumatic disease
Summary
Key References
- Rheumatology, 2-Volume Set (Hochberg/Elsevier, 2022) - "Using Multiple Antibodies and Bispecific Molecules" (Ch. 8)
- Goodman & Gilman's Pharmacological Basis of Therapeutics - "Bispecific Antibodies: CD19 and CD3" (Ch. 72, Fig. 72-5)
- Katzung's Basic and Clinical Pharmacology, 16e - Bispecific T cell engagers/Teclistamab
- Harrison's Principles of Internal Medicine 22e - Bispecific antibodies, CRS management
- Nordmann-Gomes A et al. T-cell engagers in rheumatology. Best Pract Res Clin Rheumatol 2026. [PMID: 41951534] - 80-patient multicenter analysis
- Larue M et al. Bispecific T-cell engagers in autoimmune diseases: mechanisms, clinical evidence, challenges. Autoimmun Rev 2026. [PMID: 42002248] - Comprehensive mechanistic review
- Shah K et al. Disrupting B and T-cell collaboration: T-cell engagers vs. CAR-T in autoimmune disease. Clin Exp Immunol 2024. [PMID: 38642912]
- Li J et al. CAR-T and BiTE: new horizons in treatment of rheumatic autoimmune diseases. Front Immunol 2026. [PMID: 41694371]
- Groener M, Paik JJ. Emerging B and plasma cell-targeting immune therapies in IIM. Front Immunol 2025. [PMID: 40746557]
Write a detailed notes on neonatal lupus
"neonatal lupus" AND management
"neonatal lupus" AND "congenital heart block"
PMID: 40066690
PMID: 33470961
PMID: 41233007
PMID: 39022488
"neonatal lupus" AND hydroxychloroquine prevention
PMID: 41439852
PMID: 41879307
Neonatal Lupus Erythematosus (NLE) - Detailed Notes
1. Definition and Concept
2. Epidemiology
- Incidence: Affects approximately 1 in 10,000-20,000 live births; rare but increasingly recognized
- No sex predilection in the neonate; however the maternal autoimmune disease burden falls predominantly on women
- Ethnic distribution: Differential distribution of clinical features across ethnic groups exists (Sun et al., 2025)
- Skin involvement: Occurs in approximately 25% of babies born to anti-SSA/SS-B-positive mothers (Kelley/Firestein) - or up to 10% by some estimates (Hochberg)
- Cardiac involvement (CHB): Occurs in approximately 2% of babies born to mothers who are positive for anti-Ro/SS-A and/or anti-La/SS-B antibodies
- Recurrence risk:
- After a baby with complete heart block: recurrence risk in next pregnancy ~17-18%
- After a baby with cutaneous NLE (without heart block): risk for heart block in subsequent pregnancy ~18%
- HCQ treatment reduces this recurrence - from 18% to 7.4% in one trial (Buzzell et al., 2026 [PMID: 41439852])
3. Maternal Background
- SLE (most classic setting)
- Primary Sjögren's syndrome (anti-Ro/La-positive)
- Undifferentiated connective tissue disease (UCTD)
- Asymptomatic mothers - critically, in approximately 50% of cases, the mother is asymptomatic and has no known autoimmune diagnosis. This is a major reason for diagnostic delay and highlights the importance of universal antibody screening.
- Isolated anti-Ro or anti-La positivity without a clinical syndrome
4. Autoantibodies Involved
- Anti-Ro/SS-A (most important; almost 100% of cases with skin or cardiac NLE have this)
- Anti-La/SS-B (almost always accompanied by anti-Ro; anti-La alone has uncertain clinical significance)
- Anti-U1-RNP (rare; can cause NLE without cardiac involvement)
Anti-Ro/SS-A System
- Ro antigens are RNA-binding proteins present in the cell nucleus and cytoplasm
- The 52 kDa Ro (Ro52/TRIM21) antigen is the most pathogenic for cardiac NLE
- Anti-Ro antibodies are IgG class and cross the placenta via the FcRn (neonatal Fc receptor) transporter, achieving concentrations in fetal blood close to maternal levels
Anti-La/SS-B
- Anti-La amplifies the risk when present alongside anti-Ro
- Presence of both anti-Ro and anti-La with coexistent maternal hypothyroidism further increases CHB risk
5. Pathogenesis
5a. Cardiac Pathogenesis (Congenital Heart Block)
- Local complement activation
- Macrophage and TGF-β-mediated inflammatory cascade
- Calcium channel dysregulation in cardiomyocytes (L-type calcium channels are cross-reactive targets)
- Increased type I interferon (IFN) expression
5b. Skin and Other Organ Pathogenesis
- SCLE-like NLE skin lesions are histologically identical to SCLE in adults
- Anti-Ro antibodies on keratinocytes (which also express Ro on their surface after UV exposure) trigger a similar inflammatory cascade
- Photosensitivity is very common but sun exposure is NOT required - lesions can be present at birth
- Hepatobiliary and hematologic involvement result from antibody binding to hepatocytes and blood cell precursors respectively
6. Clinical Manifestations
6a. Cutaneous (Most Common - ~25% of exposed infants)
- Erythematous, annular plaques - ring-like, often with central clearing
- Resemble the annular form of subacute cutaneous lupus erythematosus (SCLE) in adults
- Individual lesions: erythematous annular papules or plaques
- Periorbital region - "raccoon eyes" or "erythematous mask" appearance (confluent periorbital erythema) - diagnostically very helpful and characteristic
- Scalp and face (most prominent)
- Trunk and extremities (less intense)

- Self-limiting - resolve spontaneously by 6 months of age (correlating with clearance of maternal antibodies)
- Usually leave NO permanent residuum
- However, in 1/4 to 1/3 of affected infants: persistent telangiectasias, dyspigmentation, and/or atrophic scarring
- Atrophic scarring more likely if lesions began in utero
6b. Cardiac (Most Serious - ~2% of exposed infants)
- First-degree heart block: prolonged PR interval
- Second-degree heart block: Wenckebach or Mobitz type
- Third-degree (complete) heart block: complete AV dissociation - the most feared complication
- Cardiomyopathy: occurs concurrently in a small percentage; may not become apparent until several months after birth
- Other structural defects: patent ductus arteriosus (PDA), ventricular septal defect (VSD), atrial septal defect (ASD), patent foramen ovale (PFO)
- Myocarditis and pericarditis also described
- Neonatal mortality: approximately 20% from CHB
- ~80% survival at 1 year (Hochberg textbook)
- ~2/3 of survivors require permanent pacemaker (Dermatology 5e; Harriet Lane Handbook)
- Survivors remain at continued risk for cardiac dysfunction later in life
- Fetal hydrops: can develop with severe CHB in utero
- Complete heart block, once established, is irreversible even with treatment
6c. Hepatobiliary (10-25% of cases)
- Often subclinical / asymptomatic but detected on routine blood tests
- Asymptomatic transaminitis - most common hepatic finding
- Conjugated hyperbilirubinemia (jaundice) in early weeks of life
- Hepatomegaly
- Hepatitis
- Cholestasis
- Liver failure (rare; can occur during gestation or neonatal period)
- Cirrhosis (rare, severe)
- Natural history: Hepatic abnormalities typically dissipate soon after delivery; routine screening is performed but not uniformly recommended by all guidelines
6d. Hematologic (10-25% of cases)
- Thrombocytopenia - most common; present at birth or in first months of life
- Autoimmune hemolytic anemia (AIHA)
- Leukopenia / Neutropenia
- Typically self-limiting as maternal antibodies clear
- Routine screening not universally recommended if infant is asymptomatic
- Rare: disseminated intravascular coagulation (DIC), microangiopathic hemolytic anemia
6e. Neurologic (Rare)
- Myelopathy
- Seizures
- Aseptic meningitis
- Hydrocephalus (rare reports)
- May contribute to neuropsychiatric disorders and developmental delays as sequelae
6f. Endocrinologic
- Case reports of endocrine involvement; not well characterized
- Maternal hypothyroidism (in mother) amplifies CHB risk
7. Diagnosis
7a. In the Mother
- Serologic testing for anti-Ro/SS-A, anti-La/SS-B (and anti-U1-RNP)
- Testing should be offered to ALL pregnant women (especially those with connective tissue disease symptoms)
- Anti-nuclear antibody (ANA) screening as initial screen
- Important: Maternal antibody titer matters - higher anti-Ro52 titers correlate with higher fetal risk
- Maternal thyroid function tests (hypothyroidism amplifies risk)
- Any pregnant woman with a sibling born with CHB should be tested
7b. In the Fetus/Neonate
- Clinical presentation (characteristic skin lesions, bradycardia, hydrops)
- Presence of anti-Ro/SS-A and/or anti-La/SS-B in mother's serum AND/OR infant's serum (passively transferred; disappear by 6 months)
- Fetal echocardiography starting at 16 weeks of gestation in all at-risk mothers (anti-Ro/La-positive)
- The ACR conditionally recommends serial fetal echo during 18-24 weeks
- Limitation: Standard weekly echo can miss the rapid evolution of first-degree to complete heart block (which can occur within days)
- Emerging: In-home fetal Doppler by the pregnant woman to monitor fetal heart rate between clinic visits - promising but not yet standard of care
- Warning signs during fetal monitoring: premature atrial contractions and moderate pericardial effusion should be taken seriously as potential harbingers of CHB
- Electrocardiogram (ECG) +/- echocardiogram
- Complete blood count with differential and platelet count
- Liver function tests
- If tests initially normal and infant asymptomatic: repeat every 2-3 months x 2-3 times
- History, physical examination, and monitoring of growth and head circumference
- Family counseling
7c. Differential Diagnosis of Skin Lesions
- Tinea corporis: annular but with scale; NLE lesions have little or no scale
- Reactive erythema
- Drug eruption
- Erythema multiforme
- Urticaria
- Bullous impetigo: if intense basal cell damage with crusting occurs
- Langerhans cell histiocytosis
- Seborrhoeic dermatitis
8. Management
8a. Antenatal Prevention
- HCQ is associated with reduced risk of cardiac NLE in anti-Ro-positive pregnancies
- Mechanism: HCQ inhibits endosomal Toll-like receptor (TLR7/TLR9) signaling, reducing type I interferon production triggered by anti-Ro/La-RNA immune complexes; also reduces placental transfer of autoantibodies
- A prospective open-label trial of HCQ dosing through pregnancy in women with a prior infant with Ro-antibody related CHB: significant decrease in CHB incidence (OR 0.44; p=0.02) (Hochberg textbook, block 19, line 270-273)
- Buzzell et al. (2026, Lupus [PMID: 41439852]): HCQ reduced CHB recurrence from 18% to 7.4% in one registered clinical trial
- Zhang (2026, Aust NZ J Obstet Gynaecol [PMID: 41879307]): Evidence supports HCQ for overall and secondary prevention (recurrence); data on primary prevention (first occurrence) is still limited
- HCQ is safe in pregnancy (no documented teratogenicity) and is another key reason it should be continued throughout SLE pregnancy
8b. Management of First- or Second-Degree Heart Block
- Dexamethasone (or betamethasone) is the treatment of choice
- Fluorinated glucocorticoids preferred because they cross the placenta and enter the fetal circulation (unlike non-fluorinated steroids like prednisolone which are inactivated by placental 11β-HSD2)
- Some small case series describe reversal of early (1st/2nd degree) heart block with dexamethasone
- Treatment of incomplete fetal heart block remains controversial - benefits not clearly delineated
- Fetal side effects: intrauterine growth retardation (IUGR), oligohydramnios, adrenal suppression
- First- or second-degree block may or may not reverse with treatment
- Complete heart block does not reverse with treatment - it is irreversible
8c. Management of Complete (Third-Degree) Heart Block
- Permanent cardiac pacemaker: Required in approximately 2/3 of survivors
- Often implanted at or shortly after delivery
- Most effective intervention to maintain cardiac function
- Survivors with pacemakers remain at risk for cardiac dysfunction long-term
- Emerging technologies: new pacing systems and fetal pacing under investigation
8d. Management of Cutaneous NLE
- Sun avoidance and sun protection (UVA/UVB blocking sunscreen, protective clothing)
- Mild topical corticosteroids for symptomatic lesions
- No systemic treatment required for skin involvement alone
- Lesions resolve spontaneously by 6 months in most cases
8e. Management of Hematologic and Hepatic NLE
- Usually self-limiting and require only monitoring
- Severe thrombocytopenia may require corticosteroids or IVIG
- Liver failure (rare) requires intensive supportive management
- Routine neonatal screening: ECG, CBC, LFTs (Dermatology 5e monitoring protocol)
8f. Treatment Summary (Harriet Lane Handbook)
- Treatment is dependent on presenting symptoms and cardiac involvement
- May include: steroids, cardiac pacing, and IVIG
- Other inflammatory features resolve as maternal antibodies clear - usually within 6 months
9. Prognosis and Long-Term Outcomes
For Cardiac NLE:
- 20% neonatal mortality from CHB
- 80% survival to 1 year
- ~2/3 survivors require permanent pacemaker
- Continued risk of cardiac dysfunction in pacemaker-dependent children
- Dilated cardiomyopathy may develop months after birth in a subset
- CHB that develops in utero but is detected late may have worse outcomes (hydrops)
For Non-Cardiac NLE:
- Excellent prognosis - all manifestations resolve by 6 months
- Skin: resolve completely in 2/3-3/4; remainder have telangiectasias, dyspigmentation, or mild atrophic scarring
- Hematologic and hepatic: dissipate soon after delivery
Long-Term Risk for the Child:
- Children who have had NLE are at increased risk for autoimmune disease later in childhood (Kelley/Firestein)
- Risk for neuropsychiatric disorders and developmental delays as sequelae (Sun et al., 2025)
- Mothers who have had a baby with cutaneous NLE have increased likelihood of subsequent pregnancy complications including cardiac NLE
Subsequent Pregnancies:
- High-risk for recurrence: ~17-18% for CHB in next pregnancy after an affected child
- These women should be cared for by a perinatologist with specialized training in high-risk prenatal care
- HCQ should be continued/initiated throughout all future pregnancies
- Serial fetal echocardiography every 1-2 weeks from 16-26 weeks gestation in subsequent pregnancies
10. Monitoring Protocol Summary
| Timing | Monitoring |
|---|---|
| Pre-conception | Test all women with SLE/Sjögren/UCTD for anti-Ro, anti-La; counsel on risks |
| 16-26 weeks gestation | Serial fetal echocardiography every 1-2 weeks in anti-Ro/La-positive mothers |
| Fetal heart rate monitoring | Home Doppler (emerging, not yet standard) |
| At birth | ECG, echocardiogram, CBC with diff and platelets, LFTs |
| 0-9 months (neonate) | Repeat CBC + LFTs every 2-3 months x2-3 if initially normal; more frequently if abnormal |
| Growth monitoring | Head circumference and growth parameters at each visit |
| Long-term | Monitor for delayed autoimmune disease in childhood |
11. Genetic and Immunologic Context
- Maternal antibodies are necessary but NOT sufficient to cause NLE - only ~2% of exposed fetuses develop CHB
- Genetic susceptibility of the fetus modulates risk (specific HLA alleles under study)
- Fetal sex: no significant sex predilection in NLE itself (unlike SLE in adults)
- The autoantibody titer matters: high anti-Ro52 titers (>200 U/mL in some studies) are associated with higher CHB risk
- Both the transplacental antibody load and the fetal inflammatory response determine outcome
12. Key Points Summary
- NLE is a passively acquired autoimmune disease - NOT true lupus in the infant
- Caused by transplacental transfer of maternal anti-Ro/SS-A, anti-La/SS-B, or anti-U1-RNP antibodies
- Mother may be asymptomatic in 50% of cases - universal antibody screening in pregnancy is important
- Cutaneous NLE: ~25% of exposed infants; annular erythematous periorbital and facial plaques; photosensitive; self-limiting by 6 months; treat with sun protection and mild topical steroids
- Cardiac NLE (CHB): ~2% of exposed infants; most serious; 20% mortality; 2/3 require pacemaker; irreversible once complete; vulnerable period 16-24 weeks gestation
- Hepatic and hematologic: transient; usually subclinical; monitor and treat symptomatically
- Pathogenesis: fetal cardiocyte apoptosis → surface Ro/La expression → antibody binding → AV node inflammation → fibrosis → heart block
- Fetal echocardiography from 16 weeks is the monitoring standard in high-risk pregnancies
- Hydroxychloroquine is the key preventive agent - reduces CHB recurrence by >50%; should be maintained throughout pregnancy
- Dexamethasone (fluorinated steroid) is the treatment for early (1st/2nd degree) heart block - benefits are uncertain and complete block is irreversible
- IVIG has NOT been proven effective for prevention
- Prophylactic steroids are NOT recommended due to fetal side effects
- Recurrence risk after affected sibling: ~17-18% for CHB
Key References
- Firestein & Kelley's Textbook of Rheumatology - "Neonatal Lupus" section (block 20, lines 5769-5832) and SLE skin manifestations (block 10)
- Rheumatology, 2-Volume Set (Hochberg/Elsevier, 2022) - "Neonatal Lupus" (block 19, lines 223-276)
- Dermatology, 2-Volume Set 5e - "Neonatal lupus erythematosus" (block 9, lines 2661-2690) - comprehensive management table
- Harriet Lane Handbook (Johns Hopkins, 23e) - "Neonatal SLE" (block 4, lines 6679-6693)
- Creasy & Resnik's Maternal-Fetal Medicine - "Fetal-Neonatal Outcomes in Lupus Pregnancy" (block 17)
- Sun W et al. Neonatal lupus erythematosus: an acquired autoimmune disease to be taken seriously. Ann Med 2025. [PMID: 40066690]
- Jimenez E et al. Congenital Heart Block. Clin Perinatol 2025. [PMID: 41233007]
- Buzzell A et al. Current and future interventions for neonatal lupus: review of NLM clinical trials database. Lupus 2026. [PMID: 41439852] - HCQ reduces CHB recurrence 18% → 7.4%
- Zhang SH. Role of hydroxychloroquine in prevention of CHB in anti-Ro/La-positive pregnancies. Aust NZ J Obstet Gynaecol 2026. [PMID: 41879307]
- Derdulska JM et al. Neonatal lupus erythematosus - practical guidelines. J Perinat Med 2021. [PMID: 33470961]
- Nagliya D et al. Sjogren's Antibodies and Neonatal Lupus: A Scoping Review. Cureus 2024. [PMID: 39022488]
- Makadia L, Izmirly P, Buyon JP. Autoimmune Congenital Complete Heart Block: How Late Can It Occur? AJP Rep 2023. [PMID: 37168107]
Detailed notes on JIA. Subtypes of Juvenile idiopathic arthritis (JIA). Write in detail about the management of systemic JIA and its complications. Mainly from rheumatology textbooks and journals
"juvenile idiopathic arthritis" AND classification AND subtypes
"systemic JIA" AND "macrophage activation syndrome" AND treatment
PMID: 35233986
PMID: 37487610
"systemic JIA" AND "lung disease" OR "ILD" AND anakinra OR canakinumab OR tocilizumab
"systemic juvenile idiopathic arthritis" AND "interstitial lung disease" OR "pulmonary"
"macrophage activation syndrome" AND "2-18" criteria diagnosis
"macrophage activation syndrome" AND "sJIA" AND diagnosis criteria
"sJIA" AND "lung disease" AND IL-18 OR emapalumab
PMID: 37923864
PMID: 39317415
PMID: 39058514
Juvenile Idiopathic Arthritis (JIA) - Detailed Notes
1. Definition
- Previously known as Juvenile Rheumatoid Arthritis (JRA) in the US and Juvenile Chronic Arthritis (JCA) in Europe
- Reclassified under the umbrella term JIA by the International League of Associations for Rheumatology (ILAR) in 1995, revised 1997 and 2001
- PRINTO (Pediatric Rheumatology International Trials Organization) proposed a revised classification in 2019 (still not universally adopted)
2. ILAR Classification - Seven Subtypes
Table: ILAR Classification of JIA (from Firestein & Kelley, Table 109.1)
| Subtype | Definition | Key Features |
|---|---|---|
| 1. Oligoarticular JIA | ≤4 joints in first 6 months | Most common (~50%); ANA+; uveitis risk |
| 2. RF-negative Polyarticular JIA | ≥5 joints, RF negative | 25-40% of JIA; heterogeneous |
| 3. RF-positive Polyarticular JIA | ≥5 joints, RF+ (×2, ≥3 months apart) | Resembles adult RA; ACPA+ |
| 4. Systemic JIA (sJIA) | Arthritis + quotidian fever (≥2 weeks) + rash, adenopathy, HSM, or serositis | 10-20% of JIA; innate immune |
| 5. Psoriatic Arthritis | Arthritis + psoriasis, or 2 of: dactylitis, nail pitting, family history psoriasis | Dactylitis distinctive |
| 6. Enthesitis-Related Arthritis (ERA) | Arthritis + enthesitis, or arthritis/enthesitis + HLA-B27 features | Axial involvement; male predominance |
| 7. Undifferentiated JIA | Meets criteria for >1 category or none | Residual category |
PRINTO 2019 Proposed Categories (newer, not yet universally adopted):
- Systemic JIA
- RF-positive JIA
- Enthesitis/spondylitis-related JIA
- Early-onset ANA-positive JIA
- Other JIA
- Unclassified JIA (Also proposes extending age cutoff to <18 years)
3. Individual JIA Subtypes - Key Characteristics
3a. Oligoarticular JIA (Persistent and Extended)
- Most common subtype: accounts for ≥50% of JIA cases
- Two subcategories:
- Persistent: ≤4 joints throughout disease course
- Extended: Starts oligoarticular but involves >4 joints after first 6 months (worse prognosis)
- Demographics: Young girls, peak onset 2-4 years
- Joints: Asymmetric, large joints - especially knee, ankle; hip rarely affected
- ANA positive: 60-80% (predicts uveitis risk)
- Uveitis: Asymptomatic, chronic anterior uveitis in 20-30%; major cause of visual loss; slit-lamp examination mandatory every 3-6 months
- RF and HLA-B27: Typically negative
- Prognosis: Good for persistent type; extended type has worse joint outcomes
- Radiographic changes: Bony overgrowth (limb length discrepancy at knee); less erosive than RA
3b. RF-Negative Polyarticular JIA
- 5 or more joints in first 6 months; RF negative
- Demographics: Bimodal age distribution - early childhood and adolescence
- Joints: Symmetric; small and large joints; cervical spine, temporomandibular joints (TMJ)
- ANA positive: ~25%
- Uveitis: ~5-10%
- Prognosis: Variable; some go into remission, others have persistent active disease
3c. RF-Positive Polyarticular JIA
- Clinically most resembles adult rheumatoid arthritis
- Demographics: Predominantly adolescent girls
- RF positive on ≥2 occasions, ≥3 months apart; often ACPA (anti-CCP) positive
- Joints: Symmetric small joints (MCPs, PIPs, wrists); erosive arthritis
- Nodules, vasculitis: Can occur
- Uveitis: Less common
- Prognosis: Often most destructive JIA subtype; rarely remits off medication
3d. Psoriatic Arthritis JIA
- Arthritis + psoriasis (often follows arthritis by years), or arthritis + ≥2 of:
- Dactylitis ("sausage digit")
- Nail pitting / onycholysis
- Family history of psoriasis in first-degree relative
- Joint involvement: Asymmetric; DIP joints commonly involved (unlike other JIA)
- Dactylitis: Characteristic feature
- Uveitis: Asymptomatic, chronic anterior
- HLA-B27: Can be positive in older children with axial involvement
3e. Enthesitis-Related Arthritis (ERA)
- Arthritis + enthesitis (inflammation at ligament/tendon insertions), OR arthritis/enthesitis plus ≥2 of:
- Sacroiliac tenderness / inflammatory lumbosacral pain
- HLA-B27 positivity
- Family history of HLA-B27-associated disease
- Anterior uveitis (acute, symptomatic)
- Onset in a boy after age 6
- Demographics: Predominantly adolescent boys; HLA-B27 strong association
- Joints: Lower extremity large joints (knees, ankles, hips); entheses (Achilles, patellar, plantar fascia)
- Spine/sacroiliac: Often develops over years; may evolve to ankylosing spondylitis
- Uveitis: Acute anterior, symptomatic (red, painful eye) - unlike silent uveitis of oligoarticular JIA
- IBD association: Must consider if GI symptoms, poor growth, or delayed puberty
- Diagnosis challenge: Full picture may not emerge until adulthood; SEA (seronegative enthesopathy and arthropathy) syndrome is a related entity
- Hip disease: Major morbidity feature requiring early total hip replacement in some
3f. Undifferentiated JIA
- ~15% of JIA cases (Scandinavian epidemiologic data)
- Meets criteria for >1 category OR for no category due to exclusion criteria
- Most commonly derived from oligoarticular or ERA phenotypes
- Main reason for exclusion: first-degree relative with psoriasis, or meeting >1 category criteria
4. Systemic JIA (sJIA) - In Detail
4a. Epidemiology and Demographics
- Proportion: 10-20% of all JIA
- Age: Any age; tendency toward 1-5 years of age, peaking ~2 years
- Sex: No sex difference (unlike other JIA subtypes)
- Rare in adults: Called Adult-Onset Still's Disease (AOSD) when it starts in adults
- sJIA and AOSD are now considered a continuum (Hinze et al., Nat Rev Rheumatol, 2023)
4b. Immunopathogenesis
- Early/active systemic phase: Dominated by innate immune activation - neutrophils, monocytes, macrophages; S100 proteins (S100A8/A9/A12) markedly elevated; cytokines: IL-1β, IL-6, IL-18, IL-8, TNF, MIF all elevated
- Chronic arthritic phase: Adaptive immune features emerge - autoimmune T cells; HLA class II association
- Key cytokines:
- IL-6: Correlates with fever, joint involvement, laboratory features; targetable with tocilizumab
- IL-1β: Drives systemic inflammation; targetable with anakinra/canakinumab
- IL-18: Markedly elevated; contributes to MAS and sJIA-LD; emerging therapeutic target
- IFN-γ: Central to MAS pathogenesis; targetable with emapalumab
- ~50% of patients respond dramatically to IL-1 blockade; ~50% have incomplete response → heterogeneity within sJIA
4c. Clinical Manifestations of sJIA
Fever
- Quotidian (daily) spiking fevers reaching ≥39°C
- Occur once or twice daily; return to normal (or subnormal) between spikes
- Child appears ill and irritable during fever, recovers well when afebrile (diagnostic clue)
- Must persist for ≥2 weeks to meet diagnostic criteria
Rash (Pathognomonic)
- Present in ~80% of patients
- Salmon-pink, evanescent, migratory, macular rash (1-5 mm flat or slightly raised macules)
- Typically spares the face; can be scattered or diffuse; often subtle
- Can be difficult to identify in dark-skinned individuals
- Koebner phenomenon: Rash can be elicited by stroking/scratching the skin - diagnostically helpful
- Appears and disappears with fever spikes ("evanescent")

Arthritis
- Variable: from minimal to oligoarticular to polyarticular
- Arthritis may NOT be present at onset - can appear weeks to months after systemic symptoms begin
- Arthralgias and myalgias are almost universally present at onset even without frank arthritis
- Arthritis severity typically does not correlate with severity of systemic manifestations
- Tenosynovitis and synovial cyst formation can occur
Other Systemic Features
- Lymphadenopathy: Generalized
- Hepatosplenomegaly: Common
- Serositis: Pleuritis, pericarditis, peritonitis/abdominal pain
- Pericardial involvement (clinical + subclinical) in up to 36% of patients
- Poor growth: Due to systemic inflammation and corticosteroid use
Laboratory Features (No Diagnostic Test - Characteristic Pattern)
- Very high inflammatory markers: ESR, CRP markedly elevated
- Significant leukocytosis with neutrophilia and bandemia
- Thrombocytosis (reactive)
- Anemia (chronic disease)
- Liver transaminases, aldolase, ferritin, fibrin split products may be elevated
- Ferritin elevation: Very useful marker; extreme elevation (>10,000 ng/mL) raises concern for MAS
- ANA, RF: Rarely positive (important negative finding)
- S100A8/S100A9 and S100A12 proteins: highly elevated, useful disease activity markers
4d. Diagnosis of sJIA - Exclusion Approach
- Infections: Blood/urine cultures, viral studies (EBV, CMV, parvovirus)
- Malignancy: Especially leukemia and neuroblastoma - bone marrow aspiration and biopsy often needed
- Periodic fever syndromes: (PFAPA, FMF, TRAPS, CAPS, HIDS) - distinguished by characteristic fever periodicity
- Other rheumatic diseases: Kawasaki disease (young children), systemic lupus, AOSD
4e. Course and Prognosis of sJIA (Pre-biologic Era)
- Monocyclic: Single episode with remission within 2 years (~1/3 of patients)
- Polycyclic (relapsing): Flares of systemic features with mild-moderate arthritis (~30%)
- Persistent: Continuous active disease; often destructive arthritis in ~40%; most morbidity
-
50% of patients historically received corticosteroids and multiple DMARDs
- Long-term joint destruction in up to 1/3 of patients (pre-biologic era)
- Amyloidosis: Previously a major cause of death; now rare due to aggressive therapy
5. Management of Systemic JIA
- JADAS (Juvenile Arthritis Disease Activity Score)
- ACR Pediatric 30/50/70 response criteria
5a. Step-Up Treatment Framework (ACR 2021 Guideline - PMID 35233986)
Mild sJIA (Mild systemic symptoms + synovitis, no organ involvement)
- NSAIDs as monotherapy: First line for mild disease
- Naproxen (10-20 mg/kg/day ÷ 2 doses)
- Ibuprofen (40 mg/kg/day ÷ 4 doses)
- Indomethacin: Particularly useful for fever control and serositis
- May control symptoms in a minority; most will require escalation
- Intraarticular corticosteroids (IAS): If only a few large joints involved; triamcinolone hexacetonide preferred
- If no response or worsening: proceed to IL-1 or IL-6 inhibitors directly
Moderate-Severe sJIA (More severe systemic symptoms, absence of MAS)
- Systemic corticosteroids (for rapid control of severe symptoms):
- Oral prednisone: 60 mg/day (daily high dose), OR
- IV methylprednisolone: 30 mg/kg/dose (maximum 1 g/day) for up to 3 days, followed by tapering oral prednisone
- Caution: Prolonged high-dose steroids cause growth delay, osteoporosis, cushingoid features, adrenal suppression
- Biologic DMARDs - IL-1 or IL-6 inhibitors: Should be added early to facilitate corticosteroid taper; now considered first-line disease-modifying therapy
5b. Biologic DMARDs - The Key Agents
IL-1 Inhibitors
| Agent | Type | Dosing | Evidence |
|---|---|---|---|
| Anakinra (Kineret) | IL-1Ra (recombinant IL-1 receptor antagonist; blocks IL-1α and IL-1β) | 1-2 mg/kg/day SC (max 100 mg/day); daily injection | RCT: significantly higher responders vs. placebo at 1 month; also effective in MAS |
| Canakinumab (Ilaris) | Anti-IL-1β monoclonal antibody | 4 mg/kg SC every 4 weeks (max 300 mg) | Two phase III RCTs: significant benefit vs. placebo on ACR30 and flare rates; FDA-approved for sJIA; long-acting (every 4 weeks) |
| Rilonacept | IL-1 Trap (soluble decoy receptor) | SC weekly | Less effective than canakinumab (OR=0.10 for response; p<0.001) in meta-analysis |
IL-6 Inhibitors
| Agent | Type | Dosing | Evidence |
|---|---|---|---|
| Tocilizumab (Actemra) | Anti-IL-6R monoclonal antibody | <30 kg: 12 mg/kg IV q2wk; ≥30 kg: 8 mg/kg IV q2wk; SC formulation available | Phase III RCT (TENDER): demonstrated efficacy in sJIA; FDA-approved for sJIA; serum IL-6 correlates with fever, joints, labs |
| Sarilumab | Anti-IL-6R | Less studied in sJIA | Emerging data |
5c. Conventional DMARDs
- MTX and TNF inhibitors (TNFis): Less helpful for controlling systemic symptoms of sJIA
- May be useful if disease progresses to chronic arthritis with few systemic features
- Cyclosporine: Pre-biologic era, showed benefit for systemic symptoms and steroid-sparing; now mainly used in MAS treatment
- Monthly IV immunoglobulin (IVIG): Some benefit for systemic symptoms in pre-biologic era studies; steroid-sparing effect
5d. Targeted Synthetic DMARDs (tsDMARDs)
- Tofacitinib (JAK1/3 inhibitor): FDA approved for polyarticular course JIA (2020); effective in active sJIA and AOSD in small studies; may be helpful in sJIA-LD if IL-1/IL-6 inhibitors are discontinued
- Baricitinib (JAK1/2 inhibitor): Currently in clinical trials for sJIA (NCT04088396, age 1-18 years)
5e. Tapering and Discontinuation
- In inactive sJIA: Conditional recommendation to taper and attempt discontinuation of biologic therapy
- Long-term discontinuation is possible in only a minority of patients
- Some level of cytokine blockade needed for most patients long-term
- Tapering should be gradual with close monitoring for flare
5f. Stem Cell Transplantation (SCT)
- Reserved for very severe, refractory cases
- Both autologous and allogeneic approaches performed
- Some cases show benefit (see previous SCT discussion)
- Still considered experimental in sJIA; ~10% mortality
- The Hochberg textbook reports ~50% complete drug-free remission in autologous SCT series; 80% drug-free remission in allogeneic series
6. Complications of Systemic JIA
6a. Macrophage Activation Syndrome (MAS) - The Most Life-Threatening Complication
Definition and Epidemiology
- MAS is a form of secondary/acquired hemophagocytic lymphohistiocytosis (HLH) occurring in the setting of rheumatic disease
- Overt MAS: Develops in approximately 10% of sJIA patients
- Subclinical/mild MAS: Develops in as many as 30% of sJIA patients; can evolve to full-blown MAS if undertreated
- Mortality: 6-30%; accounted for the majority of JIA mortality prior to 2001; now ~5-8% with improved recognition and treatment
- Triggers (Firestein & Kelley):
- Active sJIA disease: 50% of cases
- Infectious triggers (especially Epstein-Barr virus EBV): 1/3 of cases
- Medication exposures: Minority
- Unknown: Minority
- Both IL-1 and IL-6 inhibitors did NOT prevent MAS in RCTs; cases of MAS have been reported in well-controlled sJIA on canakinumab
Pathophysiology
- Cytokine storm with excessive production of:
- IFN-γ (central driver - markedly elevated)
- IL-18 (also markedly elevated; correlates with MAS severity)
- IL-6, IL-1, TNF, IL-10
- NK cell and CD8 T-cell cytolytic dysfunction: Failure to clear antigen-presenting cells leads to sustained activation and hyperferritinemia
- Macrophage activation: Activated macrophages engulf red cells, white cells, platelets (hemophagocytosis)
- Elevated CXCL9, CXCL10 (IFN-γ-inducible chemokines), soluble IL-2RA, and soluble CD163: useful monitoring markers
Clinical Features of MAS
- Unrelenting high fevers (change in fever pattern from quotidian - fever becomes continuous)
- Hepatosplenomegaly (progressive enlargement)
- Lymphadenopathy (generalized)
- Severe cytopenias: Falling WBC, falling platelet count (paradoxically - previously high in sJIA)
- Liver dysfunction: Rising transaminases, elevated bilirubin
- CNS involvement: Seizures, coma, encephalopathy
- Coagulopathy and bleeding: DIC; elevated D-dimers
- Hyperferritinemia: Ferritin often >10,000 ng/mL (very high; in sJIA baseline may already be elevated)
- Falling platelet count (from thrombocytosis to normal/low)
- Falling ESR (paradoxical - as fibrinogen is consumed)
- Liver dysfunction (rising AST/ALT)
- Hyperferritinemia (extreme)
- Elevated D-dimers (DIC)
Diagnosis - EULAR/ACR/PRINTO 2016 MAS Classification Criteria (Ravelli et al.)
A febrile patient with known or suspected systemic JIA is classified as having MAS if the following criteria are met:Ferritin >684 μg/L (684 ng/mL)AND any 2 of the following:
- Platelet count ≤181 × 10⁹/L
- Aspartate aminotransferase (AST) >48 units/L (0.8 μkat/L)
- Triglycerides >1.56 g/L (156 mg/dL)
- Fibrinogen ≤3.6 g/L (360 mg/dL)
(Laboratory abnormalities should not be otherwise explained by concomitant immune-mediated thrombocytopenia, infectious hepatitis, visceral leishmaniasis, or familial hyperlipidemia)From Ravelli A et al. Ann Rheum Dis 2016; Arthritis Rheumatol 2016.
Treatment of MAS
- IV methylprednisolone pulse: 30 mg/kg/dose (maximum 1 g) daily for 3 days
- Followed by high-dose oral prednisone with gradual tapering
- Used in virtually all patients; methylprednisolone and prednisolone most common (90% of patients in literature)
- Dexamethasone used in ~7%
- Cyclosporine A: 2-7 mg/kg/day in 2 divided doses
- Inhibits T-cell activation and IFN-γ production
- Widely used in combination with high-dose steroids
- Anakinra: 4-8 mg/kg/day IV or SC (escalating doses in severe cases; some protocols use up to 10 mg/kg/day)
- Used in 179 MAS patients in literature; favorable outcome in 83% of sJIA-MAS (Baldo et al. 2025)
- Particularly effective when IL-18-driven hyperinflammation; preferred over canakinumab in MAS setting
- Results of RCT (NCT02780583: high-dose anakinra in sJIA-MAS) expected
- Emapalumab: Anti-IFN-γ monoclonal antibody
- Phase II trial in sJIA-MAS unresponsive to corticosteroids: complete response 93% (Baldo 2025; Bindoli 2024)
- FDA-approved for familial HLH; being adopted for sJIA-related MAS
- Targets the central cytokine driver (IFN-γ) of MAS
- "Emapalumab holds significant promise for patients with MAS associated with sJIA" (Firestein & Kelley, block 27, line 7401)
- Simultaneously identify and treat the hyperinflammation AND the underlying trigger
- Prompt recognition critical; can rapidly progress
- Multidisciplinary expert management essential
- Monitor closely for progression/complications
- 6 overarching statements + 24 specific points to consider
6b. sJIA-Associated Lung Disease (sJIA-LD) - Emerging Complication
Background
- A serious, chronic, life-threatening pulmonary complication of sJIA, first fully described in 2013
- Newly recognized and increasingly important
- Exposure to IL-1 and/or IL-6 inhibitors increased prevalence by up to fivefold since 2002
Epidemiology and Risk Factors
- Age at onset: Younger onset (<2 years) is a major risk factor
- History of MAS: Strong association
- Lymphadenopathy and hepatosplenomegaly: Associated features
- Clubbing: High incidence of erythematous clubbing at onset (pathognomonic sign)
- Trisomy 21 (Down syndrome): Over-represented in sJIA-LD cohort
- Eosinophilia: Frequent association
- Hyperferritinemia and elevated IL-18: Common
- Prominent IFN-γ gene signature
Clinical Features
- Symptoms often initially mild: chronic cough, tachypnea, and dyspnea (may be subtle)
- Most patients had active systemic inflammation at time of lung disease
- Progressive respiratory failure in severe cases
Radiology and Pathology
- CT chest: Patchy ground-glass opacities and septal thickening without prominent fibrosis
- Pathology: Unique inflammatory form of pulmonary alveolar proteinosis (PAP)-like disease
- No characteristic genetic associations with PAP identified
Mortality
- >30% mortality in affected patients - makes this a critical complication
Potential Pathomechanisms (Under Investigation)
- Cytokine imbalances: IL-1/IL-6 inhibition may cause shifts in IL-18 levels and type I/II interferons, creating immune dysregulation favoring lung inflammation
- Drug-related hypersensitivity (DRESS): Drug Reaction with Eosinophilia and Systemic Symptoms - associated with HLA-DRB1*15 allele; suggests delayed hypersensitivity reaction
- Complex immunologic milieu: Multiple interacting factors
- IL-1/IL-6 inhibitors act as antigens causing direct hypersensitization
- Biologic effects of IL-1/IL-6 inhibition set the stage for hypersensitivity via cytokine plasticity hypothesis
Management of sJIA-LD
- No established management guidelines - evaluated case-by-case
- IL-1 and IL-6 inhibitors remain first-line sJIA therapy but role in sJIA-LD is uncertain
- Decision on whether to discontinue IL-1/IL-6 inhibitors must be individualized
- JAK/STAT inhibitors may be effective in sJIA-LD as alternative agents if IL-1/IL-6 inhibitors discontinued
- Active multicenter international research ongoing
- Consider HLA-DRB1*15 typing for DRESS susceptibility
6c. Uveitis in JIA
- Chronic anterior uveitis (CAU): Most frequent extra-articular manifestation of JIA
- Incidence: 2.8% per year in first 5 years (large prospective cohort)
- Silent: Asymptomatic - no red eye, no pain in most cases (except ERA-associated uveitis which is acute and symptomatic)
- Highest risk: Young girls, ANA-positive, oligoarticular JIA (20-30% develop uveitis)
- Complications: Band keratopathy, posterior synechiae, cataracts, glaucoma, macular edema, visual loss/blindness
- Screening: Slit-lamp examination every 3-4 months for high-risk; every 6-12 months for lower risk
- Treatment: Topical steroids → methotrexate → TNFi (adalimumab preferred)
- ERA uveitis: Acute, symptomatic (red eye) - treated differently (topical steroids + NSAIDs)
6d. Growth Disturbance
- Generalized growth retardation: Due to chronic inflammation (IL-6 suppresses IGF-1) AND corticosteroid use
- Local overgrowth: Affected limb may be longer due to hyperemia stimulating epiphyseal growth
- Micrognathia: Temporomandibular joint involvement (especially polyarticular RF+ and oligoarticular) → jaw undergrowth
- Cervical spine: Atlantoaxial subluxation (especially RF+ polyarticular); C2-3 fusion can occur
- IL-1 and IL-6 biologic therapy: Significantly reduced growth delay by decreasing inflammation and corticosteroid use
6e. Amyloidosis (Pre-biologic Era Complication)
- Previously a major cause of death in sJIA
- Secondary (AA) amyloidosis from prolonged, uncontrolled systemic inflammation
- Now rare due to aggressive anti-cytokine therapy
- Kidneys and other organs affected
7. Outcomes - Impact of Biologic Therapy
Pre-biologic vs. Post-biologic Era Comparison
| Parameter | Pre-biologic Era | Post-biologic Era |
|---|---|---|
| Joint destruction | Up to 1/3 of patients | Greatly decreased |
| Growth delay | Severe, common | Significantly decreased |
| Amyloidosis | Major cause of death | Now rare |
| MAS mortality | ~22% | ~5-8% |
| CID achievement | Low | 30-50% in RCTs |
- Pediatric ACR70 improvement: 50-90%
- Clinically Inactive Disease (CID): 30-50%
- Corticosteroid discontinuation: 30-50%
8. Disease Activity Monitoring Tools
| Tool | Components |
|---|---|
| JADAS-10 | Physician global assessment (0-10) + parent/patient global assessment (0-10) + active joint count (0-10) + ESR normalized to 0-10 |
| ACR Ped 30/50/70 | 30%/50%/70% improvement in ≥3 of 6 core variables |
| Clinically Inactive Disease (CID) | No active arthritis, no fever/rash/serositis/adenopathy/HSM, normal CRP, physician global assessment = 0 |
| Minimal Disease Activity | Validated lower threshold of disease activity |
9. Key Points Summary
- JIA = arthritis of unknown etiology, onset <16 years, lasting ≥6 weeks, other conditions excluded
- 7 ILAR subtypes: Oligoarticular (most common), RF-negative poly, RF-positive poly, systemic, psoriatic, ERA, undifferentiated
- sJIA (10-20%): Unique - innate immune-driven, no sex predilection, quotidian fever + salmon rash + arthritis + systemic features
- IL-6 and IL-1 are central cytokines in sJIA; TNFi and MTX are NOT effective for systemic symptoms
- First-line sJIA: NSAIDs (mild) → IL-1 or IL-6 inhibitors (moderate-severe); corticosteroids used short-term for severe systemic features
- Canakinumab (anti-IL-1β) and tocilizumab (anti-IL-6R) are both FDA-approved and evidence-based for sJIA
- MAS: 10% overt, 30% subclinical; life-threatening secondary HLH; ferritin >684 + 2 of 4 criteria (platelets, AST, TG, fibrinogen) = 2016 EULAR/ACR MAS criteria
- MAS treatment: High-dose IV methylprednisolone + cyclosporine + anakinra; emapalumab (anti-IFN-γ) for refractory MAS (93% complete response)
- sJIA-LD: Emerging serious complication; >30% mortality; associated with IL-1/IL-6 inhibitor use, young onset, MAS history, clubbing, eosinophilia
- Uveitis: Silent chronic anterior uveitis in oligoarticular ANA+ JIA; regular slit-lamp screening mandatory
- JAK inhibitors (tofacitinib, baricitinib): Emerging role in sJIA and sJIA-LD
- Target: Clinically Inactive Disease (CID); treat-to-target paradigm now standard
Key References
- Firestein & Kelley's Textbook of Rheumatology (9780323935364) - Chapter 109 "Systemic JIA" (block 27), Chapter "JIA Skin" (block 10)
- Rheumatology, 2-Volume Set (Hochberg/Elsevier, 2022; 9780702081330) - Chapters 104 (JIA overview), Chapter 105 (sJIA), Chapter 68 (IL-1 inhibition)
- Harriet Lane Handbook (Johns Hopkins Hospital, 23e) - Pediatric rheumatology section
- Onel KB et al. 2021 ACR Guideline for Treatment of JIA (oligoarthritis, TMJ, systemic JIA). Arthritis Care Res 2022. [PMID: 35233986] - Primary clinical practice guideline
- Hinze CH, Foell D, Kessel C. Treatment of systemic juvenile idiopathic arthritis. Nat Rev Rheumatol 2023. [PMID: 37923864] - Comprehensive treatment review including sJIA-LD, JAK inhibitors, IL-18 targeting
- Bindoli S et al. Efficacy and safety of therapies for Still's disease and MAS: systematic review (EULAR/PReS guidelines). Ann Rheum Dis 2024. [PMID: 39317415] - OR ~6-8 for ACR50 with IL-1i and IL-6i; emapalumab 93% CR in MAS
- Baldo F et al. Current treatment in MAS worldwide: systematic review (METAPHOR project). Rheumatology (Oxford) 2025. [PMID: 39058514] - Anakinra favorable in 83% sJIA-MAS; emapalumab 93% MAS remission
- Shakoory B et al. 2022 EULAR/ACR Points to Consider for HLH/MAS. Ann Rheum Dis 2023. [PMID: 37487610] - 24 points for early management of HLH/MAS
- Ravelli A et al. 2016 EULAR/ACR/PRINTO Classification Criteria for MAS in sJIA. Ann Rheum Dis / Arthritis Rheumatol 2016. (Ferritin >684 + 2 of 4 criteria)