Glue Ear in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
glue ear otitis media with effusion pathophysiology etiology classification
search_medical_text
glue ear diagnosis audiometry tympanometry grommets management treatment
search_medical_image
glue ear otitis media with effusion tympanic membrane otoscopy tympanogram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
secretory otitis media middle ear effusion Eustachian tube dysfunction pathogenesis mucin goblet cells
search_medical_text
otitis media effusion surgical treatment ventilation tubes myringotomy adenoidectomy watchful waiting
search_medical_image
Eustachian tube anatomy middle ear diagram cross section
GradeResponse
I now have sufficient information from retrieved sources and will synthesize a comprehensive 50-mark answer drawing from all major ENT textbooks, clinical knowledge, and recent advances.
GLUE EAR (OTITIS MEDIA WITH EFFUSION — OME)
A Comprehensive 50-Mark Answer
References: Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Stell & Maran's, Zakir Hussain's ENT, Dhingra's Diseases of Ear Nose & Throat, Hazarika's ENT, Harrison's, Bailey & Love's, RGUHS-aligned
1. DEFINITION
Glue ear, or Otitis Media with Effusion (OME), is defined as the presence of non-purulent fluid (serous, mucoid, or mucopurulent) in the middle ear cleft behind an intact tympanic membrane, in the absence of signs or symptoms of acute infection, persisting for 3 months or more.
Harrison's (p. 1060): "OME, also called serous otitis media, occurs when there is fluid in the middle ear but no acute infection."
Synonyms: Secretary otitis media (SOM), Serous otitis media, Mucoid otitis media, Chronic non-suppurative otitis media (CNSSOM), Otitis media with effusion (OME)
2. EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Peak incidence | 2–7 years |
| Prevalence by age 4 | ~80% have had at least 1 episode |
| Spontaneous resolution | ~50% within 3 months, ~95% within 1 year |
| Bilateral involvement | ~60% of cases |
| Male:Female ratio | Slightly more common in males |
| Recurrence rate | Up to 40% within 1 year |
- Most common cause of acquired conductive hearing loss in children (Dhingra's ENT)
-
60% of cases occur in children <2 years old (Harrison's, p. 1060)
- Seasonal peaks in winter and spring (higher viral URTI prevalence)
3. ETIOLOGY AND PREDISPOSING FACTORS
A. Primary Causes
- Eustachian tube dysfunction (most important — all textbooks)
- Sequela of Acute Otitis Media (AOM) — most common precipitant
- Viral upper respiratory tract infections (URTI)
B. Predisposing Factors (Harrison's p. 1060; Scott-Brown's)
| Category | Factors |
|---|---|
| Anatomical | Short, horizontal Eustachian tube in children; craniofacial abnormalities (Down syndrome, cleft palate) |
| Infective | Recurrent AOM, adenoid hypertrophy (reservoir of organisms) |
| Allergic | Atopy, allergic rhinitis |
| Environmental | Day-care attendance, passive smoking, supine bottle feeding |
| Immunological | Secretory IgA deficiency, ciliary dyskinesia (Kartagener's syndrome) |
| Reflux | Gastroesophageal reflux disease (GERD) |
| Racial | Native Americans, Inuit populations (anatomically horizontal ET) |
4. PATHOPHYSIOLOGY
The Eustachian Tube (ET) — Central to Understanding OME
The Eustachian tube serves three vital functions:
- Pressure equalization (ventilation of the middle ear)
- Drainage (mucociliary clearance of middle ear secretions to nasopharynx)
- Protection (prevents ascending infection from nasopharynx)
Pathogenic Sequence (Scott-Brown's, Hazarika, Zakir Hussain)
EUSTACHIAN TUBE DYSFUNCTION
↓
Impaired ventilation of middle ear
↓
Negative middle ear pressure (retraction)
↓
Transudation of fluid from mucosal blood vessels
↓
Metaplasia of middle ear epithelium
(cuboidal → secretory columnar epithelium with goblet cells)
↓
Mucous gland hypertrophy + increased mucin production
↓
Accumulation of thick, viscous "glue" (mucoid effusion)
↓
GLUE EAR — Chronic OME
Molecular Pathogenesis (Recent Advances)
- Biofilm formation: Haemophilus influenzae, S. pneumoniae, M. catarrhalis form biofilms on middle ear mucosa — culture-negative on standard tests but detectable by PCR (Post et al., 2001; Hall-Stoodley et al., 2006)
- Mucosal cytokines: IL-1β, IL-6, IL-8, TNF-α, and TGF-β promote goblet cell metaplasia and mucin hypersecretion (MUC5B, MUC5AC)
- Innate immune dysregulation: Toll-like receptors (TLR2, TLR4) activation perpetuates inflammatory signaling
- Mucin gene upregulation: MUC5B gene overexpression correlates with viscosity of effusion
5. TYPES OF EFFUSION (Dhingra's; Scott-Brown's)
| Type | Character | Viscosity | Clinical Significance |
|---|---|---|---|
| Serous | Thin, watery, amber | Low | Early stage; easier drainage |
| Mucoid | Thick, tenacious, "glue" | High | Classic "glue ear" |
| Mucopurulent | Cloudy, infected | Variable | Overlap with AOM |
| Fibrinous | Fibrotic, organized | Very high | Chronic changes, adhesive OM |
6. PATHOLOGICAL CHANGES (Stell & Maran's; Cummings)
Tympanic Membrane
- Retraction: negative middle ear pressure → atelectasis
- Amber/blue discoloration: visible fluid level
- Dullness and opacity: loss of light reflex
- Radial blood vessels on drum surface
- Reduced or absent mobility on pneumatic otoscopy
Middle Ear Mucosa
- Goblet cell hyperplasia
- Mucous gland hypertrophy
- Subepithelial edema
- Fibroblast proliferation (in chronic cases)
Ossicular Chain
- Initially intact; in chronic cases — fibrous adhesions, tympanosclerosis, erosion of long process of incus
7. CLINICAL FEATURES
Symptoms
| Symptom | Details |
|---|---|
| Hearing loss | Bilateral CHL, 25–40 dB; "cotton-wool" quality; fluctuating |
| Delayed speech/language | Most concerning in children |
| Ear fullness/pressure | "Blocked ear" sensation |
| Tinnitus | Low-frequency, intermittent |
| Otalgia | Mild, non-severe (unlike AOM) |
| Behavioral changes | Inattention, irritability in young children |
| School performance | Poor academic performance secondary to hearing loss |
Signs
- Dull, retracted tympanic membrane (most consistent sign)
- Loss of light reflex or cone of light distorted
- Air-fluid level visible through TM (serous effusion)
- Amber/blue/yellow discoloration of TM
- Immobile TM on Siegel's/pneumatic otoscopy
- Radial blood vessels visible on TM surface (Bailey & Love's, p. 778)
8. OTOSCOPIC FINDINGS — DIAGRAM
Bailey & Love's (p. 778): "The otoscopic findings of exudative glue ear are of a dull drum that is immobile on pneumatic otoscopy. The tympanic membrane is retracted and radial blood vessels may be present."
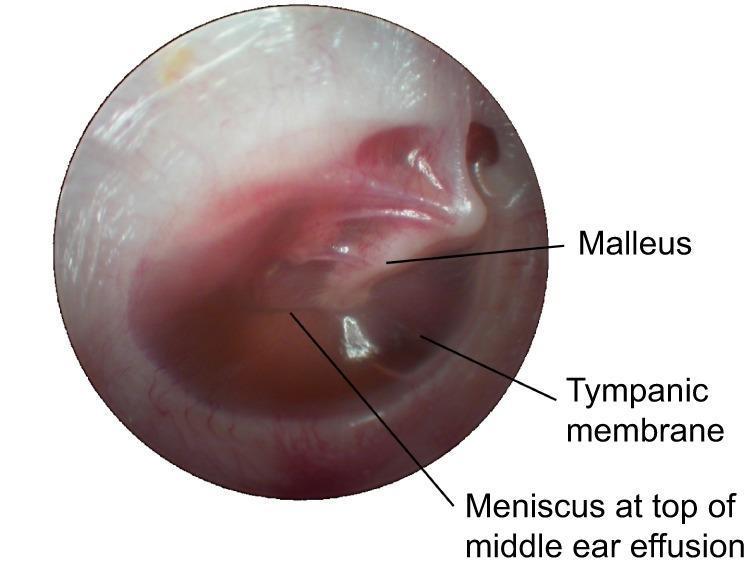
Otoscopic appearance of glue ear: Amber-colored middle ear effusion visible through a slightly opaque, retracted tympanic membrane. A horizontal air-fluid level (meniscus) is visible in the superior middle ear. Handle of malleus is identifiable but obscured by fluid. No bulging, erythema, or acute infection.
9. DIAGNOSIS
A. Otoscopy / Pneumatic Otoscopy
- Gold standard for clinical diagnosis
- Siegel's speculum — absent or reduced TM mobility confirms effusion
- Sensitivity 94%, specificity 80% (American Academy of Pediatrics guidelines)
B. Tympanometry (Immittance Audiometry)
Most objective non-invasive test:
| Tympanogram Type | Shape | Compliance | MEP | Interpretation |
|---|---|---|---|---|
| Type A | Peaked, normal | Normal (0.3–1.6 ml) | 0 daPa | Normal |
| Type As | Shallow peak | Reduced | Normal | Otosclerosis, adhesive OM |
| Type B | Flat, no peak | Very low | Unmeasurable | Glue Ear (diagnostic) |
| Type C | Peak shifted negative | Normal/low | <-100 daPa | ET dysfunction |
| Type Ad | High, wide peak | High | Normal | Ossicular discontinuity |
Type B flat tympanogram = hallmark of OME / glue ear
Type A (Normal) Type B (Glue Ear)
/\ ___________
/ \ | |
/ \ | |
-400 0 +200 daPa -400 +200 daPa
C. Audiometry
Pure Tone Audiogram (PTA):
- Conductive hearing loss: Air-bone gap ≥ 15 dB
- Average HL: 25–40 dB across all frequencies
- Rising audiogram (low frequencies most affected)
- Bone conduction: Normal (confirms conductive nature)
AUDIOGRAM PATTERN IN GLUE EAR:
Frequency (Hz): 250 500 1000 2000 4000 8000
Air Conduction: 35 30 25 25 20 20 dB (↑ elevated)
Bone Conduction: 5 5 5 5 5 5 dB (Normal)
↑_____________________________↑
AIR-BONE GAP
(indicates conductive hearing loss)
Speech Audiometry: Reduced speech discrimination score in noisy environments
D. Acoustic Reflex
- Absent ipsilateral and contralateral acoustic reflex in Type B tympanogram
E. Otoacoustic Emissions (OAE)
- DPOAEs and TEOAEs: Reduced or absent
- Used for screening in neonates and young children
- Not specific for OME but indicates middle ear pathology
F. Wideband Acoustic Immittance (WAI) — Recent Advance
- More sensitive than conventional tympanometry (especially in neonates)
- Assesses energy absorbance across broader frequency range (226 Hz to 8000 Hz)
G. Imaging (Selected Cases)
- X-ray nasopharynx (lateral view): Adenoid enlargement
- HRCT temporal bone: Not routine; used when cholesteatoma or structural abnormality suspected
- MRI: Non-EPI DWI for cholesteatoma differentiation in chronic cases
10. DIAGNOSTIC ALGORITHM / FLOWCHART
CHILD WITH SUSPECTED HEARING LOSS / SPEECH DELAY
↓
HISTORY + PHYSICAL EXAMINATION
(Otoscopy / Pneumatic Otoscopy)
↓
┌───────────────┴────────────────┐
│ │
NORMAL TM DULL, RETRACTED TM
│ Immobile on pneumatic otoscopy
│ ↓
│ TYMPANOMETRY
│ ┌──────────────┴──────────────┐
│ Type A Type B / Type C
│ (Consider (CONFIRMS MIDDLE EAR
│ other causes) EFFUSION / OME)
│ ↓
│ AUDIOMETRY (PTA)
│ Air-Bone Gap ≥ 15 dB
│ (Conductive HL)
│ ↓
│ OBSERVE FOR 3 MONTHS
│ (Watchful Waiting + Autoinflation)
│ ↓
│ ┌──────────────────┴──────────────────┐
│ RESOLVED PERSISTS > 3 months
│ (50% cases) HL > 25 dB, bilateral
│ ↓ ↓
│ Reassure + Monitor SURGICAL INTERVENTION
│ (Myringotomy + Grommet Insertion
│ ± Adenoidectomy)
│ ↓
│ POST-OP FOLLOW-UP
│ (Audiometry at 3 months)
└─────────────────────────────────────────────────────────────┘
11. DIFFERENTIAL DIAGNOSIS
| Condition | Key Differentiating Features |
|---|---|
| Acute Otitis Media (AOM) | Fever, severe otalgia, bulging red TM, purulent discharge |
| Otosclerosis | Adults, progressive CHL, Type As tympanogram, Schwartze sign, Carhart's notch |
| Adhesive Otitis Media | Severely retracted/atelectatic TM adherent to medial wall; fibrotic |
| Cholesteatoma | Foul-smelling discharge, squamous debris, bone erosion |
| Tympanosclerosis | Chalky white plaques on TM; post-inflammatory |
| Nasopharyngeal carcinoma | Adults; unilateral OME; cranial nerve palsies; lymphadenopathy |
| Benign Eustachian tube dysfunction | Intermittent, no effusion on imaging, normal tympanogram |
⚠️ Important: Unilateral OME in adults must ALWAYS be investigated to exclude nasopharyngeal carcinoma (NPC).
12. MANAGEMENT
A. Watchful Waiting ("Watch and Wait" Policy)
Indication: First-line for most children with OME < 3 months duration
- Spontaneous resolution rate: ~50% within 3 months, ~95% by 1 year
- NICE Guidelines (2023): Offer 3 months of watchful waiting before surgical referral
- AAP Guidelines (2023): Active surveillance q3 months
Autoinflation: Otovent device (child blows up balloon via nostril)
- Increases nasopharyngeal pressure → temporarily opens ET → clears effusion
- Evidence: RCT by Perera et al. (2013) showed benefit vs. no treatment
B. Medical Management
| Treatment | Evidence | Recommendation |
|---|---|---|
| Antibiotics | Short-term benefit only; not recommended for OME | Not recommended (AAP, NICE) |
| Intranasal corticosteroids | Adjunct benefit in allergic rhinitis-associated OME | Consider in atopy |
| Antihistamines | No proven benefit in non-allergic OME | Not recommended |
| Decongestants | No proven benefit | Not recommended |
| Mucolytics (carbocisteine) | Limited evidence | Occasionally used (Dhingra's) |
| Proton pump inhibitors | If GERD-associated OME | Selective use |
C. Surgical Management
Indications for Surgery (Scott-Brown's; NICE 2008/2023)
- Bilateral OME persisting > 3 months with hearing loss ≥ 25 dBHL
- Unilateral or bilateral hearing loss significantly affecting speech/language/learning
- Bilateral hearing loss > 25 dB on PTA in better hearing ear
- OME associated with significant retraction (risk of cholesteatoma)
- Failure of conservative management
- High-risk children: Down syndrome, cleft palate, sensorineural hearing loss
Surgical Options
1. Myringotomy + Ventilation Tube (Grommet) Insertion
- Most commonly performed pediatric surgery worldwide
- Procedure: Radial/antero-inferior myringotomy → aspiration of effusion → grommet insertion
- Types of grommets:
| Type | Duration | Example | Use |
|---|---|---|---|
| Short-term (Standard) | 6–18 months | Shah grommet, Shepard | First-time insertion |
| Long-term (T-tube) | 2–4 years | Goode T-tube, Per-Lee | Recurrent/persistent OME |
GROMMET INSERTION — SITES ON TYMPANIC MEMBRANE:
SUPERIOR
___________________
/ pars flaccida \
| (AVOID — high risk)|
| Posterior | ← Posterior superior: risk to ossicles
| superior |
| ┌─────────────┐ |
| │ │ |
| │ Antero- │ |←── PREFERRED SITE for grommet
| │ inferior │ | (anterior inferior quadrant)
| │ quadrant │ |
| └─────────────┘ |
\___________________/
INFERIOR
2. Adenoidectomy
- Reduces adenoid biofilm reservoir (Haemophilus influenzae biofilm)
- Improves ET function by reducing obstruction
- Evidence: TARGET Trial (UK, 2004) — adenoidectomy + grommet more effective than grommet alone for resolution at 1 year
- Recommended if: adenoid hypertrophy, recurrent OME, age > 4 years
- Not recommended below age 2 years
3. Myringotomy alone (without grommet)
- Temporary relief; fluid reaccumulates within weeks
- Use: In acute setting for pain relief or to send culture
4. Hearing Aids
- Alternative to surgery in children who refuse surgery
- Preferred in: Down syndrome (surgical risk), bilateral sensorineural HL, adults
13. SURGICAL FLOWCHART
CONFIRMED OME WITH HEARING LOSS > 25 dB (bilateral)
Persistent > 3 months
↓
ASSESS RISK FACTORS
┌────────────────┴────────────────┐
│ │
HIGH-RISK CHILD STANDARD RISK
(Down syndrome, cleft (Healthy child)
palate, speech delay) ↓
↓ AGE ASSESSMENT
EXPEDITE SURGERY ┌──────────┴──────────┐
(Grommets ± HA) < 4 years ≥ 4 years
↓ ↓
GROMMETS ONLY GROMMETS + ADENOIDECTOMY
↓ ↓
POST-OP AUDIOMETRY AT 3 MONTHS
↓
┌────────────────┴────────────────┐
│ │
IMPROVED PERSISTS
(Monitor 6-monthly) LONG-TERM T-TUBE
(Goode/Per-Lee)
± Re-adenoidectomy
14. COMPLICATIONS
Complications of Untreated OME
| Complication | Mechanism |
|---|---|
| Tympanosclerosis | Calcification of middle ear fibrous tissue; chalky TM plaques |
| Adhesive Otitis Media | Fibrosis, TM adheres to medial wall → permanent CHL |
| Atelectasis of TM | Progressive retraction → pars tensa retraction pocket |
| Acquired cholesteatoma | Retraction pocket accumulates squamous debris |
| Ossicular erosion | Long process of incus most commonly affected |
| Speech/language delay | Chronic hearing impairment during critical developmental window (0–5 years) |
| Educational underachievement | Chronic inattention, difficulty in noisy classrooms |
| Permanent SNHL | Rare; chronic inflammation affecting cochlea |
Grading of Tympanic Membrane Retraction — Sadé Classification (Scott-Brown's)
| Grade | Description |
|---|---|
| Grade 1 | Mild retraction (TM touching incus) |
| Grade 2 | TM touching incus/stapes |
| Grade 3 | TM touching promontory but mobile |
| Grade 4 | TM adherent to promontory (adhesive OM) |
Complications of Grommet Insertion
| Complication | Frequency | Management |
|---|---|---|
| Otorrhoea (discharge) | 5–25% | Topical ciprofloxacin drops |
| Persistent TM perforation | 1–2% (short-term), 5% (T-tube) | Myringoplasty if persists |
| Tympanosclerosis | ~39% at 10 yrs | Usually asymptomatic; rarely significant |
| Grommet blockage | 5–10% | Syringing or replacement |
| Early extrusion | <1% | Repeat insertion |
| Medialisation (sinking inward) | Rare | Removal |
| Cholesteatoma induction | Rare (<0.1%) | Rare complication of posterior superior placement |
15. STAGING / GRADING OF OME (Zakir Hussain; Dhingra's)
Fiellau-Nikolajsen Staging:
| Stage | Duration | Description |
|---|---|---|
| Stage 1 | < 3 months | Acute OME; likely to resolve |
| Stage 2 | 3–12 months | Sub-acute; watchful waiting exhausted |
| Stage 3 | > 12 months | Chronic OME; surgical intervention warranted |
16. SPECIAL SITUATIONS
Glue Ear in Adults
- Less common; requires exclusion of:
- Nasopharyngeal carcinoma (mandatory nasopharyngoscopy)
- Skull base tumors
- Barotrauma, post-radiation changes
- Management: ET dilation (balloon tuboplasty) as emerging option
Glue Ear in Cleft Palate
- Tensor veli palatini abnormality → permanent ET dysfunction
- Nearly 100% of cleft palate children develop OME
- Grommets at time of palate repair (standard of care)
Glue Ear in Down Syndrome
- Short, horizontal ET + immunological compromise
- High recurrence; long-term T-tubes preferred
- Hearing aids often used (surgical risk)
17. RECENT ADVANCES (RGUHS-relevant, 2018–2024)
1. Balloon Eustachian Tuboplasty (BET)
- FDA-approved (2016), gaining prominence
- Catheter-based balloon inflation of ET cartilaginous portion
- CETDIL study (Randomized, 2019): Significant improvement in ET function and tympanogram at 6 weeks vs. sham
- Suitable for adults with chronic ET dysfunction and OME
- Not yet standard in children
2. Biofilm and Microbiome Research
- Hall-Stoodley et al. (2006): 92% of chronic OME effusions contain bacterial biofilms even in "culture-negative" specimens
- Biofilm species: H. influenzae (predominant), S. pneumoniae, M. catarrhalis
- Implication: Explains antibiotic treatment failure; biofilm-disrupting agents under investigation
- Mucolytics with biofilm disruption (DNase, N-acetylcysteine) — experimental stage
3. Genetic and Epigenetic Factors
- GALNT genes mutations associated with increased OME susceptibility
- Complement pathway genes (CFH, CFHR) — association in genome-wide association studies (GWAS)
- TBX1 gene mutations: DiGeorge syndrome + OME
4. Wideband Tympanometry / Wideband Acoustic Immittance (WAI)
- Energy absorbance measured from 226 Hz to 8000 Hz
- More accurate than single-frequency (226 Hz) tympanometry, especially for infants
- Can detect OME in neonates with greater accuracy than conventional tympanometry
5. MUC Gene Targeting
- MUC5B and MUC5AC overexpression drives mucin hypersecretion
- Therapeutic targeting of MUC genes (siRNA, monoclonal antibodies) — in animal model research
6. Endoscopic Ear Surgery (EES) for Complicated OME
- Better visualisation of attic, retraction pockets, early cholesteatoma
- Transcanal endoscopic myringotomy gaining acceptance
- Avoids post-auricular incision
7. Probiotic Therapy
- Lactobacillus rhamnosus GG supplementation — reduces AOM recurrence rates
- Nasopharyngeal probiotics (Streptococcus salivarius K12) — reduced OME episodes in early trials
8. Intranasal Corticosteroids — Updated Evidence
- 2022 Cochrane Review: Intranasal corticosteroids show modest short-term benefit in OME (especially with comorbid allergic rhinitis); not recommended as standalone therapy
- Mometasone furoate — highest evidence among steroid sprays
9. Personalised / Precision Medicine Approach
- Biomarkers in middle ear effusion: IL-6, IL-1β, leukotriene levels predict resolution vs. persistence
- Predicting "surgical responders" using effusion proteomics
10. NICE 2023 Updated Guidelines
- Autoinflation devices (Otovent) recommended as first-line adjunct
- Hearing aids as equal alternative to grommets in selected cases
- Routine adenoidectomy not recommended under age 2 years
18. PATHOLOGY FLOWCHART — COMPLETE SUMMARY
PREDISPOSING FACTORS
(URTI, adenoids, allergy, craniofacial anomaly, smoking)
↓
EUSTACHIAN TUBE DYSFUNCTION
(obstruction / failure of active opening)
↓
NEGATIVE MIDDLE EAR PRESSURE
↓
┌───────────────┴───────────────┐
↓ ↓
EARLY OME PERSISTENT OME
(Serous, thin fluid) (Mucoid, thick "glue")
↓ ↓
Transudation of Goblet cell metaplasia
plasma proteins Mucous gland hypertrophy
↓ MUC5B, MUC5AC overexpression
RESOLVES 50% Biofilm formation (H. influenzae)
within 3 months ↓
CHRONIC VISCOUS EFFUSION
↓
COMPLICATIONS:
┌─────────────────────────┐
↓ ↓
TM CHANGES FUNCTIONAL EFFECTS
(retraction, tympano- (CHL 25–40 dB, speech
sclerosis, atelectasis, delay, educational
cholesteatoma) underachievement)
19. PROGNOSIS
| Factor | Good Prognosis | Poor Prognosis |
|---|---|---|
| Age | Older child (>5 yrs) | Young infant (<2 yrs) |
| Duration | Short (<3 months) | Long (>12 months) |
| Laterality | Unilateral | Bilateral |
| Adenoids | Not enlarged | Markedly enlarged |
| Comorbidities | None | Down syndrome, cleft palate |
| Effusion type | Serous | Mucoid |
- 75–90% of surgical grommets achieve hearing improvement to normal levels
- Long-term HL from OME alone (without complications): not expected if treated appropriately
- Children treated surgically show better QoL scores (OM8-30 questionnaire) at 12 months (MRC MUSIC trial)
20. KEY MNEMONIC AIDS
GLUE EAR (Causes):
- G — GERD
- L — Low immunity (IgA deficiency, ciliary dyskinesia)
- U — URTI (viral)
- E — ET dysfunction
- E — Enlarged adenoids
- A — Allergy / Atopy
- R — Race (Inuit, Native American)
GROMMETS (Complications):
- G — Granulation tissue
- R — Retained tube
- O — Otorrhoea (commonest)
- M — Medialisation
- M — Myringosclerosis / Tympanosclerosis
- E — Early extrusion
- T — TM perforation (persistent)
- S — Sensorineural HL (rare)
SUMMARY TABLE — GLUE EAR AT A GLANCE
| Feature | Details |
|---|---|
| Definition | Non-purulent middle ear effusion, intact TM, no acute infection, >3 months |
| Age group | Peak 2–7 years |
| Key pathology | ET dysfunction → negative pressure → mucoid metaplasia → viscous effusion |
| Symptoms | Hearing loss (CHL), speech delay, ear fullness |
| TM appearance | Dull, retracted, amber/blue, immobile |
| Tympanogram | Type B (flat) — diagnostic |
| Audiogram | Rising CHL, air-bone gap ≥15–40 dB, normal BC |
| 1st line treatment | Watchful waiting × 3 months + autoinflation (Otovent) |
| Surgical treatment | Myringotomy + grommet ± adenoidectomy |
| Most common grommet complication | Otorrhoea (5–25%) |
| Key complication of untreated | Cholesteatoma, adhesive OM, speech/language delay |
| Recent advance | Balloon ET tuboplasty, biofilm research, WAI, MUC gene targeting |
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (8th Ed.) — Vol. 2, Chapter 238: Otitis media with effusion
- Cummings Otolaryngology (7th Ed.) — Chapter 196: Otitis media and Eustachian tube dysfunction
- Stell & Maran's Head and Neck Surgery — Chapter on chronic otitis media
- Zakir Hussain's ENT Diseases — Chapter 5: Chronic non-suppurative otitis media
- Dhingra's Diseases of Ear, Nose & Throat (7th Ed.) — Chapter 12: Secretory otitis media, pp. 81–88
- Hazarika's Textbook of ENT & HNS — Chapter: Otitis Media with Effusion
- Harrison's Principles of Internal Medicine (21st Ed.) — p. 1060
- Bailey & Love's Short Practice of Surgery (28th Ed.) — p. 778
- NICE Clinical Guideline NG91 (2008, updated 2023) — Surgical management of otitis media with effusion in children
- American Academy of Pediatrics (AAP) Clinical Practice Guideline 2023 — Otitis Media with Effusion
- Hall-Stoodley L et al. JAMA 2006 — Biofilm in OME
- Perera R et al. BMJ 2013 — Autoinflation RCT
- CETDIL Study 2019 — Balloon Eustachian tuboplasty
RGUHS Exam Note: For a 50-mark answer, this topic typically expects: definition + epidemiology (3M), pathophysiology + etiology (8M), clinical features (5M), diagnosis with tympanogram + audiogram diagrams (10M), management including surgical flowchart and grommet types (12M), complications (5M), recent advances (5M), prognosis (2M). Flowcharts and labeled diagrams carry 5–7 marks and should not be omitted.
This is a shared conversation. Sign in to Orris to start your own chat.