Parkinson disease with clinical
Reading File
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND diagnosis AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed clinical response on Parkinson's Disease.
Parkinson Disease - Clinical Overview
Definition & Epidemiology
Parkinson disease (PD) is the second most common progressive neurodegenerative disorder after Alzheimer disease, first described by James Parkinson in 1817 as "involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported; with a propensity to bend the trunk forward." It affects approximately 1% of the population over age 65 and 4-5% of those over 85. Onset typically occurs between 45 and 70 years, peaking in the sixth decade. Men are slightly more affected than women. About 1 million people are affected in North America.
- Adams and Victor's Principles of Neurology, 12th Edition, p. 1085
- Textbook of Family Medicine 9e, p. 1249
Pathophysiology
Dopaminergic Degeneration
PD results from the progressive loss of pigmented dopaminergic neurons in the substantia nigra pars compacta (SNpc), causing depletion of striatal dopamine. Neuronal loss also occurs in the locus coeruleus, dorsal raphe, nucleus basalis of Meynert, and enteric nervous system. The resulting dysfunction of the cortico-striato-thalamo-cortical circuit reduces thalamocortical drive, impairing facilitation of the motor cortex.
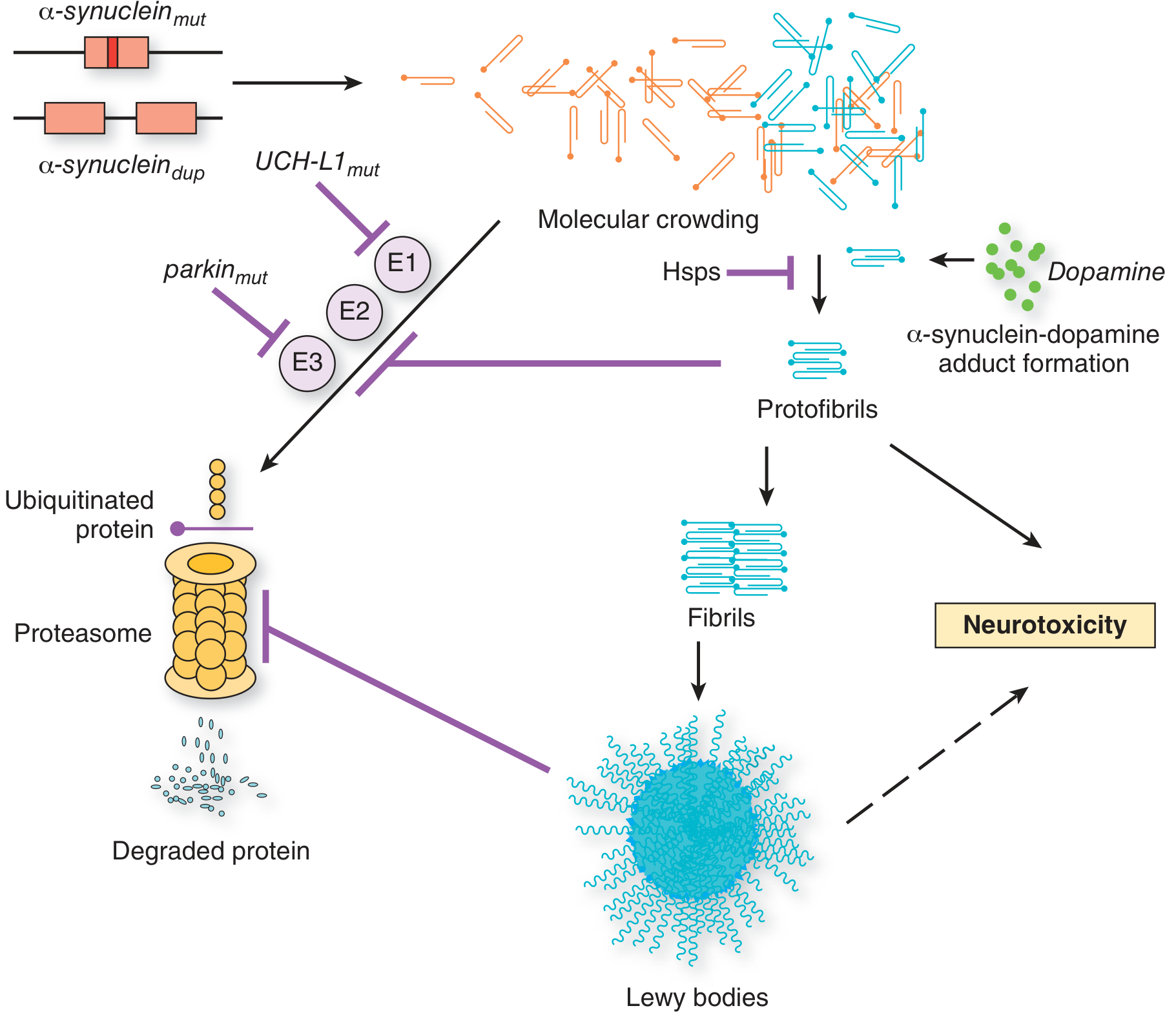
Lewy Bodies
The hallmark histopathological finding is eosinophilic intracytoplasmic inclusions called Lewy bodies, composed of aggregated alpha-synuclein protein. Excess alpha-synuclein (from gene duplication, point mutations, or failure of proteasomal degradation via parkin/UCH-L1 mutations) forms protofibrils, then fibrils, then Lewy bodies, leading to neurotoxicity.
Genetics
Up to 15% of patients have a first- or second-degree relative with PD. Key genetic loci include:
| Locus | Gene (Protein) | Inheritance | Age of Onset | Lewy Bodies | Notes |
|---|---|---|---|---|---|
| Park1/4 | SCNA (alpha-synuclein) | AD | 30-40 yr | + | A53T, A30P mutations |
| Park2 | PARK2 (parkin) | AR | 20-40 yr | - | 50% of early-onset familial PD |
| Park5 | UCH-L1 (ubiquitin esterase) | AD/SNP | 50s | + | Reduces ubiquitin recycling |
| Park6 | PINK1 | AR | Variable | - | Mitochondrial gene |
| Park7 | DJ-1 | AR | 30s | ? | Oxidative stress response |
| Park8 | LRRK2 (leucine-rich repeat kinase 2) | AD/risk | Late | ± | Common in Ashkenazic Jews |
- Adams and Victor's Principles of Neurology, 12th Edition, p. 1091
Clinical Features
Cardinal Motor Features (the "TRAP" tetrad)
- Tremor - Resting "pill-rolling" tremor, ~4 Hz, typically begins in one hand; dampened by voluntary movement; asymmetric onset. Tremor is the presenting symptom in 70% of patients. A finer 7-8 Hz action tremor may also coexist.
- Rigidity - "Lead-pipe" resistance to passive movement throughout the range; when combined with tremor produces the characteristic "cogwheel" ratcheting quality (cog-wheel rigidity / Negro sign).
- Akinesia/Bradykinesia - Slowness and poverty of movement; patients describe "weakness" but strength testing is normal. Manifest as reduced arm swing, micrographia, hypomimia (masked facies).
- Postural instability - A late feature; results in falls and festinating (accelerating) gait.
Initial Symptoms (Hoehn & Yahr, 1967)
| Symptom | Frequency |
|---|---|
| Tremor | 70% |
| Gait disturbance | 11% |
| Stiffness | 10% |
| Slowness | 10% |
| Muscle aches | 8% |
| Loss of dexterity | 7% |
| Handwriting disturbance | 5% |
| Depression/psychiatric | 4% |
| Speech disturbance | 3% |
Other Motor Signs
- Hypomimia (masked facies) - reduced facial expression
- Hypophonia - soft, monotonous speech
- Micrographia - small handwriting that gets progressively smaller
- Festinating gait - short, shuffling steps that accelerate; difficulty stopping or turning
- Reduced blink rate (normal 12-20/min reduced to 5-10/min) - causes characteristic "stare"
- Flexed posture - stooped stance with fingers adducted at metacarpophalangeal joints
- Freezing - sudden transient inability to move, especially through doorways
Non-Motor Features (frequently underrecognized)
-
Autonomic dysfunction: orthostatic hypotension, constipation, urinary urgency, seborrhea, sialorrhea (drooling)
-
Dysphagia: subjective in 35%, objective studies show ~82% prevalence; silent aspiration in 15-33%
-
Sleep disorders: REM sleep behavior disorder (can precede motor symptoms by years), excessive daytime sleepiness
-
Cognitive/psychiatric: depression (very common), anxiety, apathy, hallucinations (especially with advanced disease or dopamine agonists), and ultimately dementia (Parkinson disease dementia)
-
Anosmia: loss of smell, often an early premotor symptom
-
Pain: diffuse aching of back, neck, shoulders - often the first complaint
-
Adams and Victor's Principles of Neurology, 12th Edition, p. 1085-1087
-
Textbook of Family Medicine 9e, p. 1249
Diagnosis
PD is a clinical diagnosis - no confirmatory laboratory test or imaging exists for routine use. The UK Parkinson's Disease Society Brain Bank criteria require:
- Bradykinesia plus at least one of: rigidity, 4-6 Hz resting tremor, or postural instability
- Exclusion of other causes
- At least 3 supportive features (asymmetric onset, progressive course, levodopa responsiveness, rest tremor, etc.)
The MDS-UPDRS (Movement Disorder Society Unified Parkinson Disease Rating Scale) is the standard tool for rating severity and monitoring.
Differential Diagnosis: Parkinsonism-Plus Syndromes
Up to 20% of patients initially diagnosed with PD ultimately have an alternative diagnosis. Red flags ("atypical features") that suggest a Parkinsonism-plus syndrome:
| Feature | Suggested Diagnosis |
|---|---|
| Paralysis of vertical (esp. downward) gaze, early falls, axial rigidity | Progressive Supranuclear Palsy (PSP) |
| Early dementia + hallucinations, rigidity > tremor | Dementia with Lewy Bodies (DLB) |
| Autonomic failure + cerebellar signs + poor levodopa response | Multiple System Atrophy (MSA) |
| Step-wise progression, broad-based gait, basal ganglia infarcts on MRI | Vascular Parkinsonism |
| History of neuroleptic/antiemetic use; reversible | Drug-induced Parkinsonism |
Drugs causing drug-induced parkinsonism: Neuroleptics (typical and atypical), metoclopramide, prochlorperazine, amiodarone, valproic acid, lithium, methyldopa, reserpine.
The key differentiator in most cases is: failure to respond to levodopa suggests Parkinsonism-plus.
- Textbook of Family Medicine 9e, p. 1249-1250
Staging (Hoehn & Yahr Scale)
| Stage | Description |
|---|---|
| 1 | Unilateral involvement only |
| 2 | Bilateral involvement, no balance impairment |
| 3 | Bilateral + mild balance impairment; physically independent |
| 4 | Severe disability; can walk/stand unassisted |
| 5 | Wheelchair bound or bedridden |
Management
When to Start Treatment
Treatment should be initiated when symptoms cause functional impairment or pose a risk of physical injury. There is no evidence that delaying levodopa alters disease course.
Pharmacological Treatment
1. Levodopa / Carbidopa (Gold Standard)
- Levodopa (dopamine precursor) + carbidopa (peripheral decarboxylase inhibitor to reduce peripheral side effects)
- Most effective symptomatic treatment
- Initial response: sustained benefit throughout the day
- Long-term complications (within 2-5 years in ~50% of patients):
- Wearing-off / end-of-dose akinesia - symptoms worsen before next dose
- On-off fluctuations - unpredictable switching between good control ("on") and poor control ("off")
- Dyskinesias - involuntary choreiform movements at peak dose
- Even after 20+ years, most classic motor features continue to respond
- Newer formulations: controlled-release, fast-acting inhaled levodopa (works within 10 min for "off" states), continuous duodenal infusion
2. Dopamine Agonists (Pramipexole, Ropinirole, Rotigotine)
- Preferred initial therapy in patients under 65 who are cognitively intact
- Delay onset of motor complications compared to levodopa, but with less overall benefit
- Older patients and those with cognitive dysfunction should receive levodopa first
- Side effects: hallucinations, excessive sleeping, leg edema, impulse control disorders (pathological gambling, hypersexuality, binge eating) in ~1 in 6 patients
3. MAO-B Inhibitors (Selegiline, Rasagiline, Safinamide)
- Block dopamine metabolism; used as adjuncts to extend levodopa action
- Manage wearing-off fluctuations
4. COMT Inhibitors (Entacapone, Opicapone, Tolcapone)
- Block peripheral/central catabolism of levodopa; prolong its action
- Used when motor fluctuations develop
5. Anticholinergics (Trihexyphenidyl, Benztropine)
- Helpful for tremor and drooling
- Should be avoided in older patients due to cognitive side effects
6. Amantadine
- Weak dopaminergic and NMDA antagonist
- Used for dyskinesias and mild early symptoms
Managing motor fluctuations: Increase dose frequency, switch to controlled-release formulation, add COMT inhibitor or MAO-B inhibitor, consider dopamine agonist addition, or consider surgical intervention.
- Goldman-Cecil Medicine, International Edition, p. (block54)
- Adams and Victor's Principles of Neurology, 12th Edition, p. 1091+
Surgical Treatment: Deep Brain Stimulation (DBS)
Indicated in select patients with advanced PD who have inadequate symptom control with medication or significant motor complications.
Targets:
- Subthalamic nucleus (STN) DBS: Slightly better benefit in medication-off state; allows larger medication reduction; may have higher neuropsychiatric risk
- Globus pallidus internus (GPi) DBS: Better dyskinesia suppression; more flexible long-term; preferred for "brittle" dyskinesia (at low medication doses); relatively safer neuropsychiatric profile
Both STN and GPi DBS show similar overall motor outcomes but differ in specific benefits and risk profiles.
Other Therapies
- rTMS (repetitive transcranial magnetic stimulation): Investigational; rationale is to increase motor cortex excitability and normalize oscillatory beta-activity in the basal ganglia circuit; results of RCTs remain inconclusive
- Exercise and physiotherapy: Improve gait, balance, and quality of life
- Speech therapy: For hypophonia and dysphagia
- Occupational therapy: Adaptive strategies for ADLs
Complications
- Aspiration pneumonia: Leading cause of death; silent aspiration present in 15-33%; 9.75-fold increased risk with daily drooling + silent aspiration
- Falls and fractures
- Dementia (Parkinson disease dementia): Risk increases significantly after 10+ years of disease
- Depression and anxiety: Very common; require active management
- Psychosis/hallucinations: More common with dopamine agonists; risk increases in older patients
Prognosis
PD is relentlessly progressive but its pace varies widely. With modern dopaminergic therapy, life expectancy has improved significantly. Tremor-predominant PD tends to progress more slowly than the akinetic-rigid form. The main causes of disability and death are falls, aspiration pneumonia, and dementia.
Key Sources:
- Adams and Victor's Principles of Neurology, 12th Edition - Parkinson Disease section
- Goldman-Cecil Medicine (International Edition) - Chapter 378
- Textbook of Family Medicine, 9th Edition - p. 1249-1250
- Bradley and Daroff's Neurology in Clinical Practice - DBS and neuromodulation chapters
- Recent PubMed evidence: Telerehabilitation meta-analysis (Phys Ther 2025) confirms exercise-based rehabilitation benefit (PMID: 41065729); Anxiety management in PD meta-analysis (Mov Disord Clin Pract 2025, PMID: 40568748) highlights the importance of treating non-motor symptoms.
This is a shared conversation. Sign in to Orris to start your own chat.