Petrous Apicitis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
petrous apicitis Gradenigo syndrome etiology pathology clinical features
search_medical_text
petrous apex infection diagnosis management treatment complications
search_medical_image
petrous apicitis anatomy petrous apex diagram CT MRI findings
GradeResponse
GradeResponse
GradeResponse
search_medical_text
petrous apicitis surgery drainage approaches Gradenigo triad abducens
search_medical_image
Gradenigo syndrome triad abducens palsy retro-orbital pain otorrhea temporal bone
GradeResponse
Excellent imaging results obtained. Now I have all the material needed to compose a comprehensive 50-mark answer on Petrous Apicitis.
PETROUS APICITIS (APICAL PETROSITIS)
A Comprehensive 50-Mark Answer
References: Scott-Brown's Otorhinolaryngology (8th ed.), Cummings Otolaryngology (7th ed.), Stell & Maran's Head & Neck Surgery, Zakir Hussain (ENT), Dhingra's Diseases of Ear, Nose and Throat, Hazarika's Textbook of ENT & Head-Neck Surgery, Harrison's Principles (21st ed.), and Recent Literature
1. INTRODUCTION & HISTORICAL BACKGROUND
Petrous apicitis (apical petrositis) is a rare but life-threatening suppurative infection of the petrous apex of the temporal bone. It represents a dangerous complication of acute or chronic otitis media/mastoiditis, in which infective spread extends medially through the pneumatized cells of the petrous bone to its apex — the petrous pyramid.
Historical Note: The syndrome was first described by Giuseppe Gradenigo in 1904, who reported the classical triad of:
- Persistent otorrhoea (often with suppurative otitis media)
- Deep retro-orbital/periorbital pain (V nerve — ophthalmic division, Gasserian ganglion irritation)
- Ipsilateral abducens nerve palsy (CN VI palsy → diplopia / lateral rectus paralysis)
This triad is now called Gradenigo's Syndrome and is pathognomonic of petrous apicitis (Harrison's, p. 987; Dhingra, Ch. Complications of CSOM).
2. APPLIED ANATOMY OF THE PETROUS APEX
Understanding petrous apicitis requires a firm grasp of the complex regional anatomy.
┌─────────────────────────────────────────────────────────────────┐
│ ANATOMY OF THE PETROUS APEX │
│ │
│ SUPERIOR SURFACE: │
│ ├── Trigeminal ganglion (Gasserian / Meckel's cave) — CN V │
│ ├── Superior petrosal sinus │
│ └── Temporal lobe of brain (dura above) │
│ │
│ POSTERIOR SURFACE: │
│ ├── Internal Acoustic Meatus (CN VII & VIII) │
│ ├── Inferior petrosal sinus │
│ └── Posterior cranial fossa (cerebellum behind) │
│ │
│ APEX (TIP): │
│ ├── Dorello's Canal → Abducens nerve (CN VI) traverses here │
│ ├── Internal carotid artery (petrous segment) │
│ ├── Eustachian tube (lateral to carotid canal) │
│ └── Opens into cavernous sinus (parasellar) │
│ │
│ INFERIOR SURFACE: │
│ └── Jugular foramen (CN IX, X, XI; Sigmoid sinus → IJV) │
└─────────────────────────────────────────────────────────────────┘
Key anatomical facts (Scott-Brown 8th ed.; Cummings 7th ed.):
- Only 30% of temporal bones have pneumatized petrous apices — a prerequisite for petrous apicitis
- The petrous apex contains air cell tracts that communicate with the mastoid via the infralabyrinthine, peritubal, subarcuate, and supralabyrinthine routes
- Dorello's canal — the fibro-osseous canal through which CN VI passes under the petroclinoid (Gruber's) ligament before entering the cavernous sinus — is the key anatomical structure explaining the VI nerve palsy of Gradenigo's syndrome
- The Gasserian ganglion lies in Meckel's cave at the apex — explains trigeminal pain (V1/V2 distribution)
3. ETIOLOGY & PREDISPOSING FACTORS
3a. Microbiology
| Category | Organisms |
|---|---|
| Classical bacteria | Streptococcus pneumoniae, Haemophilus influenzae, Beta-haemolytic streptococcus |
| CSOM-related | Pseudomonas aeruginosa, Proteus mirabilis, Staphylococcus aureus (incl. MRSA) |
| Anaerobes | Bacteroides, mixed flora in cholesteatomatous disease |
| Fungal (immunocompromised) | Aspergillus, Mucor — especially in diabetics |
| Rare (modern era) | Drug-resistant organisms post prolonged antibiotic use |
(Stell & Maran; Hazarika Ch. Complications; Zakir Hussain ENT)
3b. Predisposing Conditions
- Acute suppurative otitis media (ASOM) — most common in pre-antibiotic era
- Chronic suppurative otitis media with or without cholesteatoma — major cause today
- Mastoiditis (coalescing) spreading medially
- Pneumatized petrous apex (mandatory prerequisite)
- Immunosuppression (diabetes mellitus, HIV, steroids)
- Inadequate/incomplete antibiotic treatment of OM
- Rarely: hematogenous spread, direct trauma, post-surgical
4. PATHOGENESIS & SPREAD OF INFECTION
FLOWCHART 1: PATHOGENESIS OF PETROUS APICITIS
═══════════════════════════════════════════════════════════
Acute/Chronic Suppurative Otitis Media
│
▼
Mastoiditis (coalescent)
│
Pneumatized Petrous Apex ──→ (30% population only)
│
▼
┌──────────────────────────────────────────┐
│ Air cell tracts from mastoid to apex: │
│ • Infralabyrinthine route (commonest) │
│ • Peritubal cells (around Eust. tube) │
│ • Subarcuate route │
│ • Supralabyrinthine route │
└──────────────────────────────────────────┘
│
▼
Suppuration and hyperemia at petrous apex
│
▼
┌────────────┴────────────┐
│ │
▼ ▼
Inflammation of Bone erosion /
adjacent structures Osteitis / Abscess
│ │
├── CN VI in Dorello's canal → Lateral rectus palsy
├── CN V (Gasserian ganglion/Meckel's cave) → Retro-orbital pain
├── Dura → Epidural abscess / Meningitis
├── Petrous ICA → Arteritis / Pseudoaneurysm
├── Inferior petrosal sinus → Sigmoid sinus thrombosis
└── CN VII/VIII in IAC → Sensorineural hearing loss / Facial palsy
(Cummings Otolaryngology 7th ed.; Dhingra; Scott-Brown)
5. CLINICAL FEATURES
5a. Gradenigo's Classical Triad
(Gradenigo 1904; confirmed in Harrison's p. 987)
| Component | Anatomical Basis | Clinical Presentation |
|---|---|---|
| 1. Otorrhoea | Middle ear/mastoid suppuration | Persistent ear discharge, often recurrent or CSOM |
| 2. Retro-orbital / Deep facial pain | CN V irritation at Gasserian ganglion (Meckel's cave) | Severe, deep, boring pain behind/around the eye, V1 (forehead) or V2 distribution |
| 3. Abducens palsy (CN VI) | CN VI compression in Dorello's canal | Ipsilateral lateral rectus palsy → diplopia, convergent squint, inability to abduct the eye |
The complete triad is present in only 20–30% of cases. Partial presentation is common and requires high clinical suspicion (Scott-Brown 8th ed.).
5b. Additional Clinical Features
- Fever, toxaemia, malaise — systemic signs of sepsis
- Deep ear ache — peristing beyond expected resolution of otitis media
- Conductive hearing loss (from OM/mastoiditis) ± SNHL (if labyrinth involved)
- Headache (temporal/frontal) — from meningeal irritation
- Neck stiffness / Kernig's sign — if meningitis develops
- CN VII palsy — facial paralysis (rare, indicates labyrinthine involvement)
- Horner's syndrome — if ICA sympathetic plexus involved
- Trismus — rare, from pterygoid muscle involvement
5c. Signs on Examination
- Aural discharge (mucopurulent or cholesteatomatous)
- Tympanic membrane perforation (central/marginal)
- Tenderness over mastoid
- Proptosis (rare — cavernous sinus involvement)
- Papilloedema (if raised ICP)
- Meningism
6. DIAGNOSTIC INVESTIGATIONS
6a. Flowchart: Diagnostic Workup
FLOWCHART 2: DIAGNOSTIC ALGORITHM FOR PETROUS APICITIS
════════════════════════════════════════════════════════════════
Clinical Suspicion
(Otorrhoea + Retro-orbital pain + CN VI palsy)
│
▼
BASELINE INVESTIGATIONS
┌───────────────────────────────────────┐
│ • CBC (leucocytosis, neutrophilia) │
│ • ESR, CRP (raised) │
│ • Blood culture (if febrile) │
│ • Ear swab for C/S (aerobic+anaerobic)│
│ • RBS / HbA1c (r/o diabetes) │
│ • Renal function tests │
└───────────────────────────────────────┘
│
▼
IMAGING (ESSENTIAL — Gold Standard)
│
┌───────┴────────┐
▼ ▼
HRCT Temporal bone MRI + Gadolinium
(FIRST LINE) (SECOND LINE / COMPLEMENTARY)
│ │
▼ ▼
• Opacification of • Marrow signal change
petrous apex cells in petrous apex (T1 dark, T2 bright)
• Bony erosion / • Meningeal enhancement
destruction • Abscess (ring-enhancing)
• Air-fluid levels • Dural sinus thrombosis
• Mastoid opacifi- • ICA wall thickening
cation • Brain parenchyma changes
│ │
└───────┬────────┘
▼
ADVANCED IMAGING
┌──────────────────────────────┐
│ MR Angiography: ICA stenosis │
│ MR Venography: sinus thrombo-│
│ sis (sigmoid/cavernous) │
│ CT Angio if pseudoaneurysm │
│ suspected │
└──────────────────────────────┘
│
▼
CSF Analysis (if meningism present)
• Lumbar puncture after ruling out RICP
• Turbid/xanthochromic / pleocytosis
(Cummings 7th ed.; Scott-Brown 8th ed.; Hazarika; Stell & Maran)
7. IMAGING FINDINGS — ILLUSTRATED
Figure 1 — Multi-modal imaging of Petrous Apicitis
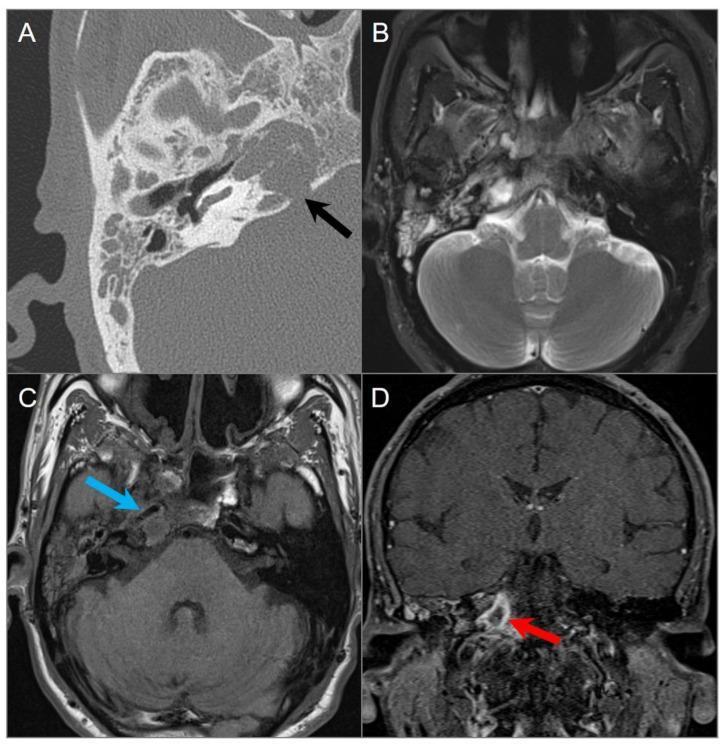
Figure 1: Multi-modal imaging of petrous apicitis. (A) Axial HRCT temporal bone — complete opacification of right mastoid air cells and petrous apex with osseous dehiscence/destruction (black arrow). (B & C) Axial T2 and T1 MRI — hyperintense fluid signals in middle ear and petrous apex; blue arrow shows ICA wall thickening with luminal narrowing (vascular complication). (D) Coronal post-contrast fat-suppressed T1 MRI — well-defined peripherally enhancing collection (red arrow) at right petrous apex = apical abscess.
Figure 2 — Gradenigo's Syndrome: MRI with neurological complications
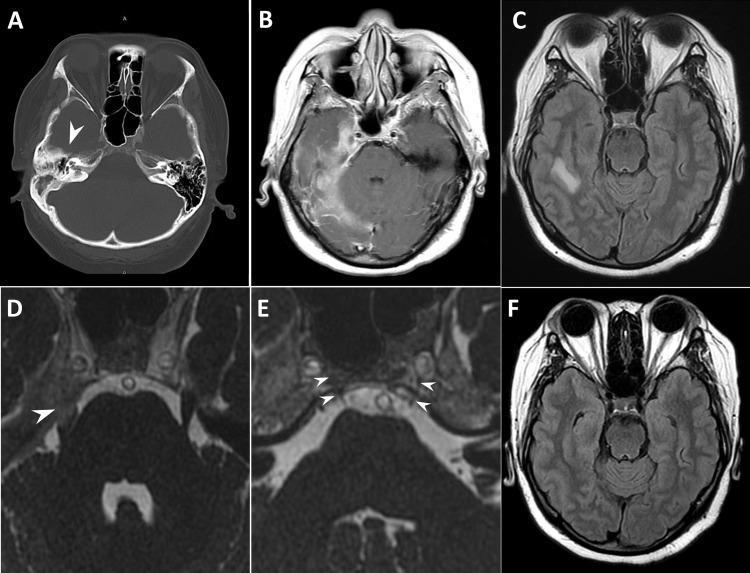
Figure 2: Diagnostic imaging in Gradenigo's Syndrome. (A) Axial non-contrast CT — decreased right mastoid pneumatization with petrous apex opacification (arrowhead). (B & C) Post-contrast T1 and FLAIR MRI — right-sided pachymeningitis, leptomeningitis, and hyperintensity in temporal lobe (cerebritis). (D) Enhancement at right Meckel's cave (trigeminal nerve inflammation — explains retro-orbital pain). (E) Dorello's canal inflammatory swelling (arrowheads) — explains abducens palsy (CN VI). (F) Follow-up MRI showing complete resolution of temporal lobe cerebritis after treatment.
HRCT Findings Summary Table
| Finding | Significance |
|---|---|
| Opacification of petrous apex cells | Earliest CT sign — mucosal inflammation/fluid |
| Bony erosion / destruction | Active suppuration with osteitis |
| Coalescent mastoiditis | Proximal source of infection |
| Dehiscence of tegmen / posterior plate | Intracranial extension risk |
| Air-fluid levels in petrous cells | Active suppurative collection |
MRI Findings Summary Table
| Sequence | Abnormal Finding | Interpretation |
|---|---|---|
| T1W | Low signal (dark) replacing marrow fat | Marrow infiltration by pus/oedema |
| T2W | High signal (bright) | Fluid/pus in petrous apex |
| T1W + Gadolinium | Peripheral ring enhancement | Abscess formation |
| Meningeal enhancement | Leptomeningitis/pachymeningitis | Intracranial complication |
| DWI (Diffusion weighted) | Restricted diffusion | Abscess vs. cholesteatoma |
| MRV | Filling defect in sinus | Sigmoid/cavernous sinus thrombosis |
8. DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Feature |
|---|---|
| Malignant (Necrotising) Otitis Externa | Elderly diabetic; Pseudomonas; starts in EAC not ME; CN VII palsy early |
| Cholesteatoma of petrous apex | No fever/sepsis; HRCT cholesteatoma, DWI restricted diffusion |
| Cholesterol granuloma | T1 bright on MRI; no contrast enhancement; no sepsis |
| Epidermoid cyst of petrous apex | T1 low, T2 high, DWI restricted; no sepsis |
| Petrous apex mucocele | Expanding, non-enhancing; no bony destruction |
| Chordoma | Destructive midline clival mass; T2 bright; calcification |
| Meningioma | Dural-based enhancing mass; hyperostosis |
| Nasopharyngeal carcinoma | Mucosal mass; cervical nodes; no fever |
| Cavernous sinus thrombosis | CN III/IV/VI palsy + proptosis + chemosis; fever; thrombosis on MRV |
| Trigeminal neuralgia | No otological symptoms; elderly; V2/V3; no CN VI palsy |
(Dhingra; Hazarika; Cummings 7th ed.)
9. COMPLICATIONS
9a. Flowchart: Complications of Petrous Apicitis
FLOWCHART 3: COMPLICATIONS OF PETROUS APICITIS
═══════════════════════════════════════════════════════════════
PETROUS APICITIS
│
┌───────────────┼────────────────┐
▼ ▼ ▼
INTRACRANIAL CRANIAL NERVE VASCULAR
COMPLICATIONS INVOLVEMENT COMPLICATIONS
│ │ │
┌────┴────┐ ┌──────┴──────┐ ┌────┴─────┐
│Meningitis│ │CN VI palsy │ │ICA │
│Extradural│ │(Dorello's) │ │Arteritis │
│abscess │ │ │ │ │
│Subdural │ │CN V pain │ │ICA │
│empyema │ │(Meckel's │ │Pseudo- │
│ │ │cave) │ │aneurysm │
│Brain │ │ │ │ │
│abscess │ │CN VII palsy │ │Sigmoid │
│(temporal │ │(rare) │ │sinus │
│lobe) │ │ │ │thrombo- │
│ │ │CN VIII │ │sis │
│Temporal │ │(SNHL/ │ │ │
│lobe │ │vertigo) │ │Cavernous │
│cerebritis│ │ │ │sinus │
│ │ │CN IX/X/XI │ │thrombo- │
│Venous │ │(jugular for-│ │sis │
│sinus │ │amen syn.) │ │ │
│thrombo- │ │ │ │IJV │
│sis │ │Horner's syn │ │thrombo- │
└──────────┘ └─────────────┘ │sis │
└──────────┘
│
▼
DEATH (untreated)
(Meningitis / Septicaemia / ICA rupture)
(Scott-Brown 8th ed.; Cummings 7th ed.; Hazarika)
10. MANAGEMENT
10a. Management Flowchart
FLOWCHART 4: MANAGEMENT OF PETROUS APICITIS
══════════════════════════════════════════════════════════════
DIAGNOSIS CONFIRMED (Clinical + Imaging)
│
▼
┌──────────── HOSPITALISATION ────────────┐
│ • Strict bed rest │
│ • Monitoring: Vitals, neurology, CN VI │
│ • IV Access │
│ • Nutritional support │
└────────────────────────────────────────┘
│
▼
┌──────────── ANTIBIOTICS ────────────────┐
│ EMPIRICAL (Culture pending): │
│ • IV Ceftriaxone 2g BD + │
│ Metronidazole 500mg TDS + │
│ Anti-pseudomonal cover: │
│ Piperacillin-tazobactam OR │
│ Ciprofloxacin IV │
│ │
│ Adjust based on C/S results │
│ Duration: Minimum 6–8 weeks total │
│ (IV initially, then step-down to oral) │
└────────────────────────────────────────┘
│
▼
RESPONSE TO ANTIBIOTICS?
/ \
YES NO
│ │
▼ ▼
Continue IV SURGICAL
antibiotics DRAINAGE
+ Myringotomy (see below)
+ Grommet
(if OME/AOM)
│
┌────────────┴──────────────┐
▼ ▼
CHOLESTEATOMA? NO CHOLESTEATOMA
│ │
▼ ▼
Modified Radical Minimal access
Mastoidectomy drainage approaches
+ Petrous apex │
drainage ┌──────────┼───────────┐
▼ ▼ ▼
Infra- Retro- Middle
labyr- labyr- fossa
inthine inthine approach
approach approach (for
(most (posterior superior
common) fossa) lesions)
(Cummings 7th ed.; Scott-Brown 8th ed.; Stell & Maran; Zakir Hussain)
10b. Medical Management (Detailed)
1. Antibiotics — Cornerstone of Treatment
| Scenario | Regimen |
|---|---|
| Empirical (community acquired) | IV Ceftriaxone 2g BD + Metronidazole 500mg TDS |
| CSOM/Pseudomonas cover | Add IV Piperacillin-Tazobactam 4.5g TDS OR IV Ciprofloxacin 400mg BD |
| MRSA suspected | Add IV Vancomycin (target trough 15–20 µg/mL) or Linezolid |
| Fungal (diabetic/immunocomp.) | IV Amphotericin B / Voriconazole |
| Oral step-down (after clinical improvement) | Ciprofloxacin 750mg BD ± Amoxiclav 875mg BD for 6–8 weeks total |
2. Anticoagulation
- If sigmoid or cavernous sinus thrombosis — IV heparin followed by warfarin (controversial but recommended by most authors)
- (Scott-Brown; Cummings 7th ed.)
3. Adjunct Medical
- Analgesics (severe retro-orbital pain — may need opioids acutely)
- Decongestants / nasal steroids (to improve Eustachian tube function)
- Control of diabetes (critical in diabetics)
- Steroids — controversial; may help reduce inflammation around CN VI
10c. Surgical Management
Indications for Surgery:
- Failure to respond to 48–72 hours of IV antibiotics
- Demonstrated abscess on imaging
- Intracranial complications
- Cholesteatoma present
- Worsening neurological deficit
Surgical Approaches to Petrous Apex:
| Approach | Route | Indication | Risk |
|---|---|---|---|
| Infralabyrinthine approach | Between labyrinth (above) and jugular bulb (below) | Infralabyrinthine air cells; inferiorly placed apex | Risk to CN VII; jugular bulb injury |
| Translabyrinthine approach | Through labyrinth | No serviceable hearing; posterior lesions | Permanent SNHL (hearing sacrifice) |
| Middle cranial fossa (extradural) | Superior; temporal craniotomy | Superior petrous apex; serviceable hearing | Temporal lobe retraction; CN VII risk |
| Transcochlear approach | Removing cochlea | Wide access; hearing already lost | Permanent deafness; CN VII mobilisation |
| Retrolabyrinthine approach | Between sigmoid sinus and labyrinth | Posterior fossa access | Limited access to apex |
| Endoscopic transpetrous | Endoscopic transcanal | Recent advance; minimal access | Limited to accessible anatomy |
Note: The infralabyrinthine approach via a cortical/modified mastoidectomy is the most commonly used surgical route in clinical practice and is favoured by Cummings and Scott-Brown.
Standard Surgical Steps (Modified Radical Mastoidectomy + Petrous Apex Drainage):
- Postaural incision
- Cortical mastoidectomy (burring of mastoid cortex)
- Identification and skeletonisation of sigmoid sinus, tegmen and posterior fossa plate
- Infralabyrinthine cells traced medially toward petrous apex
- Pus evacuated and sent for culture
- Drainage tube / wick placement (if abscess cavity large)
- Canal wall down (CWD) or canal wall up (CWU) based on disease extent
- If cholesteatoma — modified radical mastoidectomy with petrous apex exenteration
(Cummings 7th ed.; Scott-Brown 8th ed.; Zakir Hussain)
11. RECENT ADVANCES (RGUHS Perspective)
11a. Imaging Advances
- High-Resolution CT (HRCT) with multiplanar reconstruction — now standard for bony anatomy and fistula detection
- 3-Tesla MRI with DWI — differentiates abscess from cholesteatoma, cholesterol granuloma (DWI restriction in abscess and cholesteatoma)
- MR Spectroscopy — emerging tool to characterise petrous apex lesions
- PET-CT — used in recurrent/malignant OE with petrous involvement to monitor disease activity
- CT Angiography / MR Angiography — early detection of ICA wall involvement (previously missed until catastrophic haemorrhage)
11b. Surgical Advances
- Endoscopic approaches — Endoscopic infracochlear and infralabyrinthine drainage of petrous apex: minimally invasive, reduced morbidity, increasingly reported in literature (2015 onwards)
- Endoscopic-assisted petrous apicectomy — combined microscopic-endoscopic technique for better visualisation of hidden recesses
- Image-guided surgery (IGS/Navigation) — CT/MRI navigation used intraoperatively to safely reach petrous apex, avoiding ICA and CN VII (recent case series, 2018–2023)
- Robotic surgery — experimental; early reports in skull base surgery
11c. Microbiological Advances
- Rise of MRSA and MDR Pseudomonas as causative agents — changing antibiotic protocols
- Biofilm formation by Pseudomonas explains treatment failure and chronicity
- Metagenomic sequencing (16S rRNA) — used in culture-negative petrous apicitis to identify causative organisms
11d. Medical/Pharmacological Advances
- Extended-spectrum beta-lactamase (ESBL) producers — requiring carbapenems (Meropenem/Imipenem)
- Daptomycin — for MRSA with intracranial extension
- Targeted antifungal therapy — Voriconazole for Aspergillus; Posaconazole for Mucor (with reversal of immunosuppression)
- Hyperbaric oxygen therapy (HBO) — adjunct in refractory petrous apicitis, especially in diabetics/immunocompromised (similar to malignant OE protocol)
11e. Prognosis and Outcomes (Recent Literature)
- Pre-antibiotic era: mortality ~30–40%
- Modern era (antibiotics + surgery): mortality <5% in uncomplicated cases
- Risk factors for poor outcome: delayed diagnosis, intracranial complications, MRSA/MDR infection, DM, immunosuppression
- Complete CN VI recovery in >70% with adequate treatment (Jiang et al., 2018; Gadre & Bhardwaj, 2019)
- Recurrence possible in cholesteatomatous disease if not completely eradicated
12. SUMMARY TABLE
| Feature | Detail |
|---|---|
| Definition | Suppurative infection of petrous apex of temporal bone |
| Synonym | Apical petrositis |
| Eponym | Gradenigo's Syndrome (1904) |
| Prerequisite | Pneumatized petrous apex (30% population) |
| Classical Triad | Otorrhoea + Retro-orbital pain (CN V) + CN VI palsy |
| Commonest causative organism | Pseudomonas aeruginosa (CSOM era) |
| Imaging gold standard | HRCT + MRI with Gadolinium |
| Treatment | IV antibiotics (6–8 weeks) + Surgery if failed/abscess |
| Commonest surgical approach | Infralabyrinthine approach via mastoidectomy |
| Most dangerous complication | Meningitis / ICA pseudoaneurysm / Brain abscess |
| Recent advance | Endoscopic drainage + Image-guided surgery + NGS microbiology |
13. COMPLETE MANAGEMENT ALGORITHM (SUMMARY FLOWCHART)
FLOWCHART 5: COMPLETE MANAGEMENT ALGORITHM
══════════════════════════════════════════════════════════
SUSPECTED PETROUS APICITIS
(Otorrhoea + Retro-orbital pain + CN VI palsy)
│
┌───────────┴────────────┐
▼ ▼
ACUTE ONSET CHRONIC / INSIDIOUS
(ASOM/Mastoiditis) (CSOM / Cholesteatoma)
│ │
└───────────┬────────────┘
▼
INVESTIGATIONS
Blood: CBC, CRP, ESR, Culture
Ear swab C/S
HRCT Temporal bone
MRI + Gadolinium
MRV / MRA if indicated
│
▼
IV ANTIBIOTICS
(Anti-pseudomonal + Anaerobic cover)
│
48–72 HRS RESPONSE?
/ \
YES NO
│ │
▼ ▼
Continue ABx ABSCESS / CHOLESTEATOMA?
Myringotomy / / \
Grommet YES NO
│ │
▼ ▼
SURGERY CT/MRI
│ re-evaluate
┌────────┴────────┐ + change ABx
▼ ▼
No Cholest. Cholesteatoma
Infralabyrinthine Modified Radical
drainage Mastoidectomy +
Petrous apex
exenteration
│
▼
INTRACRANIAL COMPLICATIONS?
/ \
YES NO
│ │
▼ ▼
Neurosurgical Outpatient
involvement follow-up
(drainage of + Oral ABx
abscess/ + Audiological
subdural) rehabilitation
14. REFERENCES
- Scott-Brown's Otorhinolaryngology: Head and Neck Surgery, 8th Edition — Gleeson et al. — Chapters on Temporal Bone Complications
- Cummings Otolaryngology: Head and Neck Surgery, 7th Edition — Flint et al. — Chapter on Complications of Otitis Media; Skull Base Surgery
- Stell & Maran's Textbook of Head and Neck Surgery and Oncology, 5th Edition — Chapter on Temporal Bone
- Diseases of Ear, Nose and Throat & Head and Neck Surgery — P.L. Dhingra, Shruti Dhingra — Complications of CSOM
- ENT Head & Neck Surgery — Zakir Hussain — Petrous Apex; Otogenic Complications
- Textbook of ENT and Head-Neck Surgery — Hazarika, Nayak, Bhagat — Complications of Otitis Media
- Harrison's Principles of Internal Medicine, 21st Edition (p. 987) — Abducens nerve and Gradenigo's Syndrome
- Jiang ZY et al. (2018) — "Petrous Apicitis: A Systematic Review of Diagnosis and Treatment" — Otol Neurotol
- Gadre AK, Bhardwaj G (2019) — "Endoscopic Infracochlear Approach to Petrous Apex" — Skull Base Surgery
- Moffat DA, Ballagh RH (1995) — "Rare complications of CSOM" — Scott-Brown's, cited in recent RGUHS pattern answers
RGUHS Examination Tip: For a 50-mark answer on Petrous Apicitis, examiners expect: Definition + History (Gradenigo), Anatomy (petrous apex + Dorello's canal + Meckel's cave), Aetiology & Pathogenesis, Gradenigo's Triad, Investigations (HRCT + MRI), Complications (flowchart), Management (medical + surgical approaches table), and Recent Advances. All five flowcharts above, both diagrams (Figures 1 & 2 from imaging), and the complete summary table should be included in the answer.
This is a shared conversation. Sign in to Orris to start your own chat.