Blood supply and nerve supply of liver
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Blood Supply and Nerve Supply of the Liver
Blood Supply
The liver has a dual blood supply - one of its most distinctive anatomical features - but a single venous drainage system.
Arterial Supply (25% of blood flow)
The hepatic artery proper (a branch of the common hepatic artery, itself a branch of the celiac trunk) carries oxygenated blood to the liver. It travels in the hepatoduodenal ligament to the porta hepatis, where it divides into:
- Right hepatic artery - supplies the right lobe (larger branch)
- Left hepatic artery - supplies the left lobe
Variations (clinically important):
- The right hepatic artery may arise from the superior mesenteric artery (runs posterior to the bile duct, behind the pancreatic head) - this is the most common significant variant
- The left lobe artery may be augmented or replaced by a branch of the left gastric artery running in the lesser omentum
At the hilum, in the most common arrangement, the hepatic artery lies medially, the bile duct runs in the free edge of the hepatoduodenal ligament, and the portal vein lies posteriorly.
Portal Venous Supply (75-80% of blood flow)
The hepatic portal vein carries nutrient-rich but oxygen-depleted venous blood from the gastrointestinal tract, pancreas, and spleen. It is formed by the confluence of the splenic vein and superior mesenteric vein behind the neck of the pancreas.
The portal blood delivers:
- Nutrients and toxic materials absorbed from the intestine
- Blood cell breakdown products from the spleen
- Endocrine secretions (insulin, glucagon) from the pancreas and GI enteroendocrine cells
The portal vein divides at the porta hepatis into a right branch (to the right lobe) and a left branch (longer extrahepatic course, ~2 cm, to the left lobe).
Because blood from both sources mixes just before perfusing hepatocytes, liver cells are never exposed to fully oxygenated blood. - Histology: A Text and Atlas (Eroschenko)
Intrahepatic Microcirculation
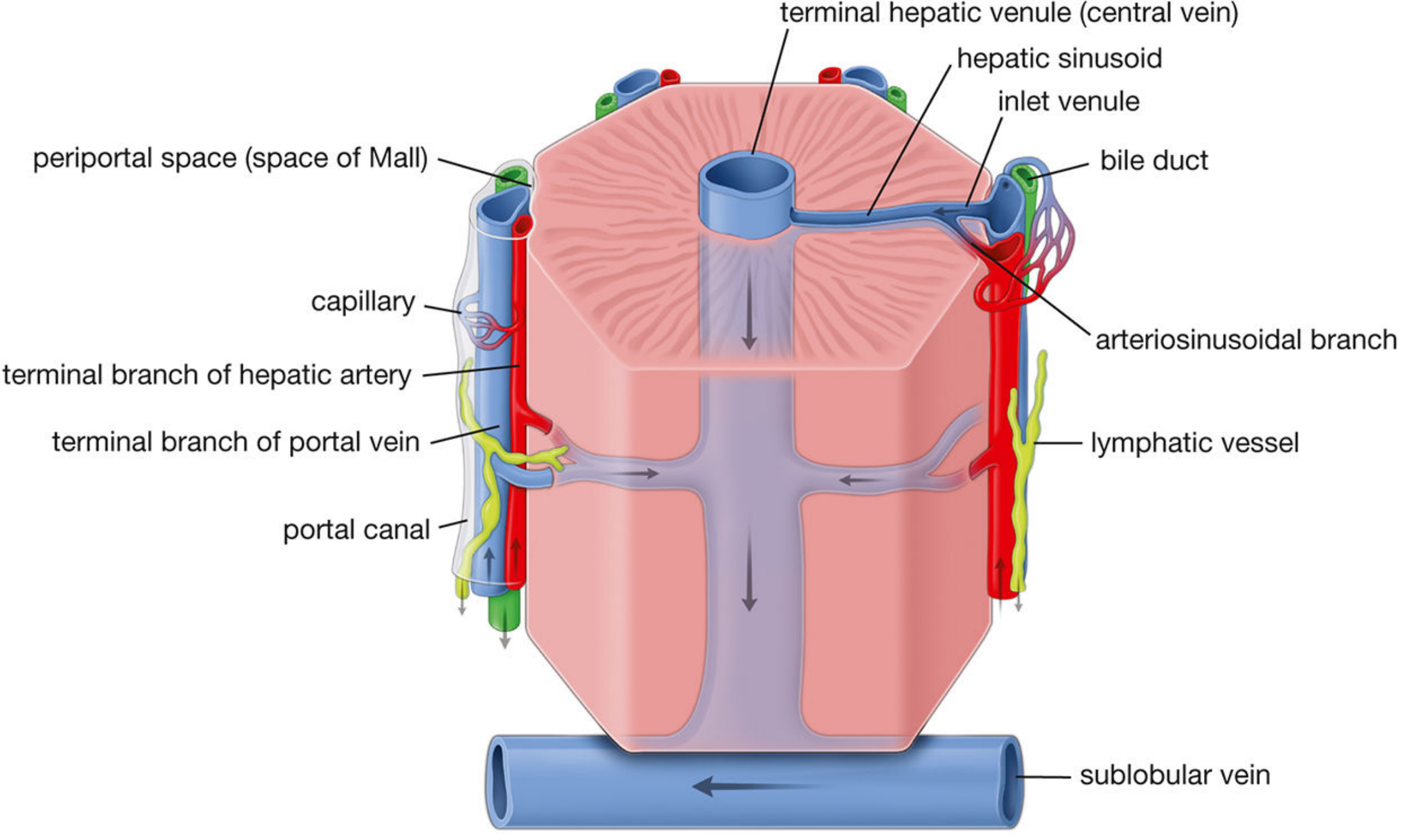
Within the liver, the terminal branches of the hepatic artery and portal vein supply the hepatic sinusoids, which are endothelium-lined blood-filled channels that bathe the hepatocytes. Blood flows from the portal triad through sinusoids toward the terminal hepatic venule (central vein):
Portal triad = terminal branch of hepatic artery + terminal branch of portal vein + bile duct (+ lymphatic vessel)
The portal blood flows centripetally through the sinusoids. Bile flows in the opposite direction, from hepatocytes into terminal canaliculi, then toward the bile ducts at the portal triad.
Venous Drainage
The liver drains via three large hepatic veins (right, middle, and left) that empty directly into the inferior vena cava (IVC) in a groove on the posterior surface of the liver, immediately below the diaphragm. Several smaller accessory hepatic veins may also drain directly into the IVC.
Nerve Supply
The liver receives exclusively autonomic innervation - there is no somatic motor supply.
Sympathetic Supply
- Preganglionic fibers: T5-T10 spinal cord segments
- Route: Via the greater splanchnic nerve → celiac ganglia (synapse) → post-ganglionic fibers via the hepatic plexus
- Hepatic plexus is a continuation/extension of the celiac plexus, the largest autonomic plexus in the abdomen
- Sympathetic fibers primarily supply the hepatic arteries (causing vasoconstriction) and travel along the vessel walls into the liver parenchyma
- Afferent sympathetic fibers carry visceral pain signals from the liver and biliary tract (T5-T10 via celiac plexus)
Parasympathetic Supply
- Source: The vagus nerve (CN X) - both left and right vagal trunks
- Vagal fibers travel via the hepatic branches of the anterior and posterior vagal trunks to the hepatic plexus
- Parasympathetic fibers innervate the gallbladder, extrahepatic bile ducts, and the liver parenchyma
- Afferent parasympathetic fibers carry sensations via the vagus nerve
| Component | Sympathetic | Parasympathetic |
|---|---|---|
| Source | T5-T10 spinal cord | Vagus nerve (CN X) |
| Route | Celiac plexus → Hepatic plexus | Hepatic branches → Hepatic plexus |
| Primary targets | Hepatic arteries | Bile ducts, gallbladder, parenchyma |
| Afferent role | Pain (T5-T10) | Satiety, nausea, distension |
Hepatic Plexus
The hepatic plexus is the final common pathway for liver innervation. It is a continuation of the celiac plexus, follows the hepatic artery and its branches, and enters the liver at the porta hepatis. Both sympathetic and parasympathetic fibers course together in this plexus.
Clinical Relevance - Referred Pain
- Acute distension of the liver capsule (e.g., hepatitis, congestive hepatopathy, rapidly enlarging abscess) causes right upper quadrant pain referred to the right shoulder, via phrenic nerve innervation of the diaphragmatic peritoneum overlying the liver - Sabiston Textbook of Surgery
- The hepatic arteries receive sympathetic fibers; the gallbladder and extrahepatic bile ducts receive both sympathetic and parasympathetic fibers
- The clinical significance of hepatic autonomic nerves is not fully understood, but they modulate glucose metabolism and portal blood flow
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Ch. 69: Blood supply and hilum of the liver
- Sabiston Textbook of Surgery - Ch. 89: Functional anatomy and innervation
- Histology: A Text and Atlas (Eroschenko) - Ch. 18: Blood supply to the liver
- Color Atlas of Human Anatomy, Vol. 2 - Vessels, nerves, and lymphatic drainage
- Miller's Anesthesia, 10th Ed. - Table 14.1: Visceral innervation of abdominal organs
Also tell me about its lymphatic drainage
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, detailed content from multiple authoritative sources. Here is the full answer:
Lymphatic Drainage of the Liver
The liver is one of the most prolific lymph-producing organs in the body - it accounts for a significant proportion of the total thoracic duct lymph flow. Lymphatic drainage occurs via two distinct systems: superficial (subcapsular) and deep (parenchymal).
Origin of Hepatic Lymph
Most hepatic lymph is formed in the perisinusoidal space of Disse - the narrow space between hepatocytes and the sinusoidal endothelium. This lymph is protein-rich filtrate. A smaller fraction (~10%) is a protein-poor filtrate from peribiliary capillary leakage.
From the space of Disse, lymph travels into the portal tract lymphatic vessels. The exact mechanism is debated - one proposed pathway involves "endothelial massaging" where circulating intrasinusoidal leukocytes create a pulsatile effect that moves lymph along toward the portal lymphatics. Terminal lymphatic branches form plexuses around the hepatic arterioles in smaller portal structures, with additional branches near portal veins and bile ducts in larger tracts. Small branches also run along the hepatic veins.
The Glisson capsule lymphatic plexus communicates with intrahepatic lymphatics through anastomotic channels. In conditions of impaired venous drainage (e.g., venous outflow obstruction or cirrhosis), lymphatic drainage becomes prominent through the Glisson capsule. - Yamada's Textbook of Gastroenterology, 7th ed.
Superficial Lymphatics
Found in the subperitoneal fibrous capsule (Glisson's capsule), these lymphatics drain in multiple directions depending on the surface of origin:
| Surface | Drainage |
|---|---|
| Anterior diaphragmatic surface (along falciform ligament) | Parasternal (internal mammary) nodes |
| Posterior diaphragmatic & visceral surfaces (bare area) | Phrenic lymph nodes or joins deep lymphatics → posterior mediastinal nodes via IVC |
| Posterior surface of left lobe (near esophageal hiatus) | Left gastric nodes |
| General visceral/diaphragmatic surfaces | Hepatic nodes in the lesser omentum |
Deep Lymphatics
Found in the connective tissue accompanying the portal triads and hepatic veins, the deep lymphatics travel in two directions:
- With the portal vein - course with portal vein and its tributaries to the hilum, then drain into the hepatic nodes at the porta hepatis
- With the hepatic veins - follow the hepatic veins converging on the IVC, pass through the diaphragmatic hiatus, and drain into the posterior mediastinal lymph nodes
Efferent Pathway (Summary)
Space of Disse
↓
Portal tract lymphatics
↓
Hepatic nodes (porta hepatis / hepatoduodenal ligament)
↓
Celiac lymph nodes (along the hepatic artery)
↓
Cisterna chyli → Thoracic duct
A secondary pathway runs:
Hepatic veins → posterior mediastinal nodes → thoracic duct
And a minor pathway:
Anterior surface → parasternal nodes
Posterior left lobe → left gastric nodes
Key Lymph Node Groups
- Hepatic nodes - lie along the porta hepatis and hepatic vessels in the lesser omentum; the primary first-echelon nodes. Their efferents drain to the celiac nodes.
- Celiac nodes - receive efferents from the hepatic nodes; drain into the cisterna chyli
- Phrenic nodes - receive drainage from the posterior bare area
- Posterior mediastinal nodes - receive drainage via the hepatic veins/IVC route through the diaphragm
- Parasternal nodes - receive drainage from the anterior surface via the falciform ligament
Clinical Significance
- Portal hypertension / cirrhosis: Impaired sinusoidal flow increases lymph production dramatically; the Glisson's capsule pathway becomes a dominant overflow route, contributing to ascites formation when lymphatic capacity is overwhelmed
- Hepatocellular carcinoma / cholangiocarcinoma: Spread follows these lymphatic routes - hepatic nodes → celiac nodes; also to posterior mediastinal nodes and parasternal nodes in advanced disease
- Liver congestion (e.g., right heart failure): Increased hepatic lymph production contributes to chylous effusions and ascites
Sources:
- Fischer's Mastery of Surgery, 8th ed. - Ch. 173: Lymphatic Drainage (Fig. 173.10)
- Yamada's Textbook of Gastroenterology, 7th ed. - Vascular and lymphatic network
- Sabiston Textbook of Surgery - Ch. 89: Functional anatomy, lymphatics
- Color Atlas of Human Anatomy, Vol. 2 - Regional lymph nodes of the liver
Also, here is the innervation diagram from Fischer's (which complements the nerve supply discussed earlier):
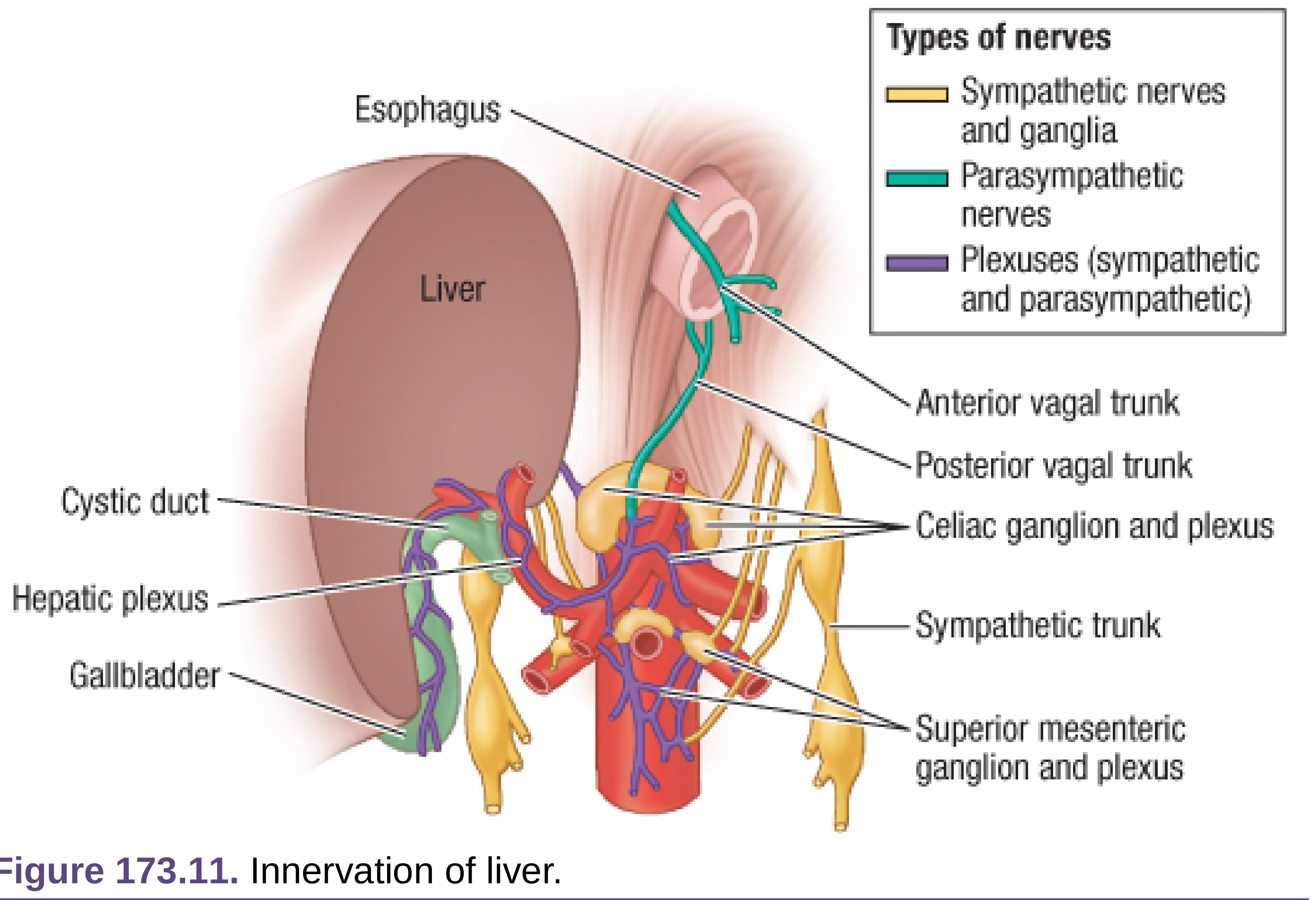
This is a shared conversation. Sign in to Orris to start your own chat.