Staging of stomach cancer and types
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gastric cancer" AND staging
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Stomach (Gastric) Cancer - Types and Staging
Overview
Gastric cancer is among the most common malignancies globally, with approximately 1.693 million combined esophageal, gastroesophageal junction (GEJ), and gastric cancer cases diagnosed in 2020. The incidence of body and distal gastric cancers has steadily declined in Western countries since the 1920s, while GEJ adenocarcinomas have markedly increased.
- Harrison's Principles of Internal Medicine, 22E
- Bailey and Love's Short Practice of Surgery, 28th Ed.
TYPES OF GASTRIC CANCER
1. By Histology
Adenocarcinoma (most common - >95%)
The vast majority of gastric cancers are adenocarcinomas. These are further subclassified by two major classification systems:
Lauren Classification (histological)
| Type | Features | Behaviour |
|---|---|---|
| Intestinal type | Cohesive cells forming gland-like structures; often well-differentiated; associated with H. pylori, atrophic gastritis, intestinal metaplasia | Tends to form a discrete mass; haematogenous spread; better prognosis |
| Diffuse type | Poorly cohesive cells (signet ring cells); lack of cell adhesion molecules (e-cadherin/CDH1); infiltrates widely | Spreads via submucosal and subserosal lymphatics; penetrates gastric wall early; worse prognosis; associated with CDH1 germline mutation |
The diffuse type spreads differently from intestinal type - it infiltrates via the submucosal and subserosal lymphatic plexus and penetrates the gastric wall at an early stage.
Signet Ring Cell Carcinoma
A subtype of the diffuse type; cells appear with a large mucin vacuole pushing the nucleus to the periphery. CDH1 (e-cadherin) germline mutations markedly increase risk.
Other Rare Types
- MALT lymphoma (Mucosa-Associated Lymphoid Tissue) - linked to H. pylori infection
- Gastrointestinal Stromal Tumours (GISTs) - arise from interstitial cells of Cajal
- Carcinoid tumours (NETs) - from neuroendocrine cells
- Squamous cell carcinoma - very rare in the stomach
2. By Macroscopic/Endoscopic Pattern
Early Gastric Cancer (EGC) - Japanese Classification
Cancer limited to mucosa or submucosa (regardless of lymph node status):
| Type | Description |
|---|---|
| Type I | Protruded / polypoid |
| Type IIa | Superficial elevated |
| Type IIb | Flat |
| Type IIc | Superficial depressed |
| Type III | Excavated / ulcerated |
Advanced Gastric Cancer - Borrmann Classification
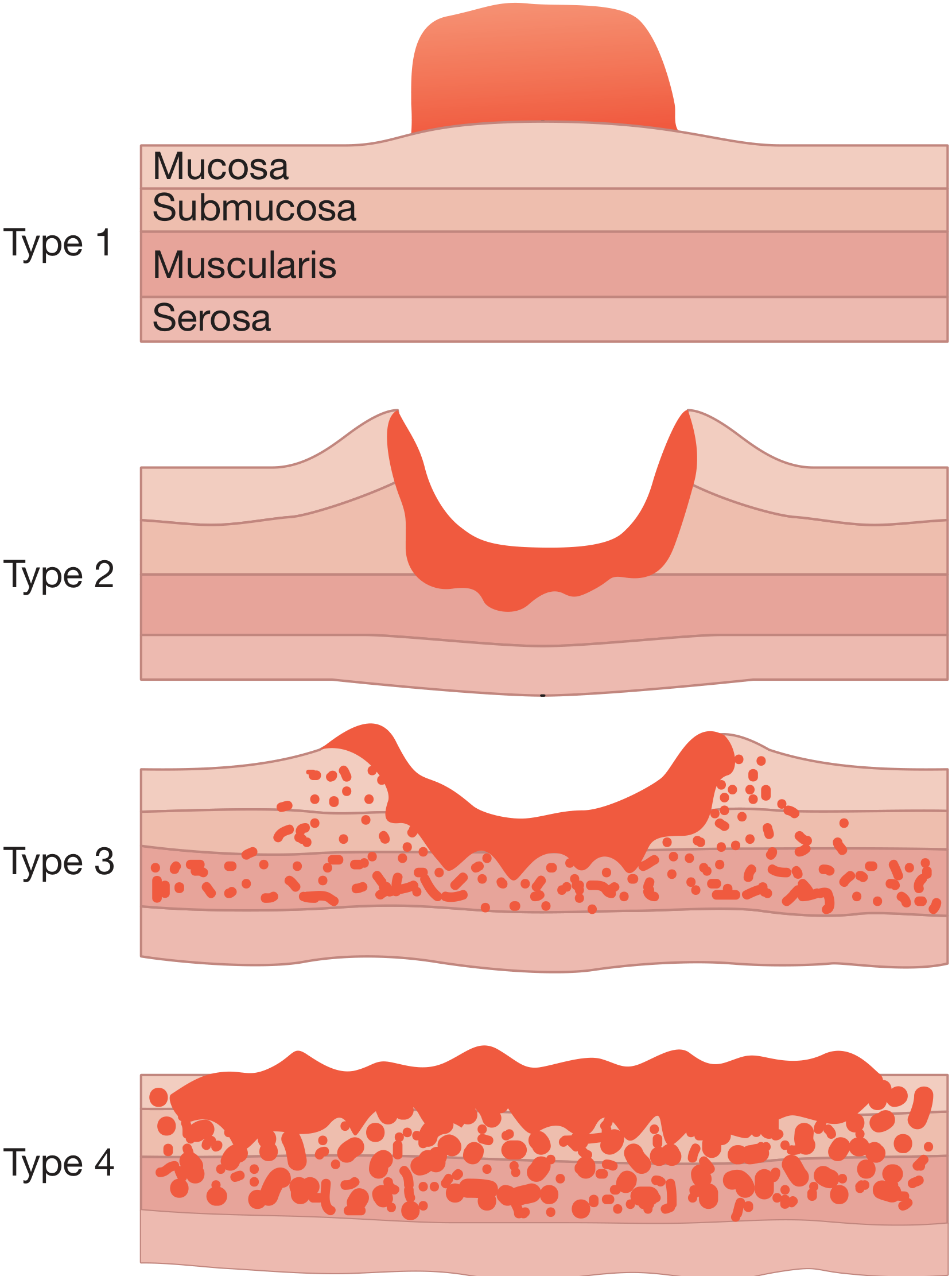
| Type | Description |
|---|---|
| Type 1 | Polypoid - well-defined, protruding mass |
| Type 2 | Ulcerating with sharp margins - crater with raised edges |
| Type 3 | Infiltrating and ulcerating - ulcer with ill-defined infiltrating margins |
| Type 4 | Diffuse infiltrating (Linitis plastica / "leather bottle stomach") - no clear margin, diffuse wall thickening |
Bailey and Love's Short Practice of Surgery, 28th Ed.
Linitis plastica (Type 4 / Borrmann IV) is a scirrhous diffuse tumour in which the stomach appears as a narrowed, rigid structure. It is the most aggressive form and has the worst prognosis.
STAGING - AJCC/UICC TNM System (8th Edition, 2017)
The staging system used universally is the AJCC/UICC TNM classification (8th edition). An important change in this edition: tumours involving the oesophago-gastric junction (EGJ) with the epicentre >2 cm into the proximal stomach are now staged as gastric cancers, while those ≤2 cm into the proximal stomach are staged as oesophageal cancers.
Grainger & Allison's Diagnostic Radiology; Bailey and Love's Short Practice of Surgery, 28th Ed.
T - Primary Tumour
| Stage | Description |
|---|---|
| Tx | Primary tumour cannot be assessed |
| T0 | No evidence of primary tumour |
| Tis | Carcinoma in situ: intraepithelial tumour without invasion of lamina propria; high-grade dysplasia |
| T1 | Tumour involves lamina propria, muscularis mucosae, or submucosa |
| T1a | Invades lamina propria or muscularis mucosae |
| T1b | Invades submucosa |
| T2 | Invades muscularis propria |
| T3 | Involves subserosa (subserosal connective tissue) |
| T4 | Perforates serosa or invades adjacent structures |
| T4a | Perforates serosa (visceral peritoneum) |
| T4b | Invades adjacent structures (pancreas, colon, liver, etc.) |
N - Regional Lymph Nodes
| Stage | Description |
|---|---|
| Nx | Cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Metastasis in 1-2 regional lymph nodes |
| N2 | Metastasis in 3-6 regional lymph nodes |
| N3 | Metastasis in 7+ regional lymph nodes |
| N3a | 7-15 lymph nodes involved |
| N3b | 16 or more lymph nodes involved |
M - Distant Metastasis
| Stage | Description |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis present (includes retropancreatic, mesenteric, para-aortic nodes; liver metastases; peritoneal seedlings) |
Overall Stage Grouping (UICC 8th Edition)
| Stage | T | N | M |
|---|---|---|---|
| IA | T1 | N0 | M0 |
| IB | T1 / T2 | N1 / N0 | M0 |
| IIA | T1 / T2 / T3 | N2 / N1 / N0 | M0 |
| IIB | T1 / T2 / T3 / T4a | N3 / N2 / N1 / N0 | M0 |
| IIIA | T2 / T3 / T4a | N3 / N2 / N1 | M0 |
| IIIB | T3 / T4a / T4b | N3 / N2 / N0-1 | M0 |
| IIIC | T4a / T4b | N3 / N2-3 | M0 |
| IV | Any T | Any N | M1 |
Bailey and Love's Short Practice of Surgery, 28th Ed. (Table 67.6)
Spread of Gastric Cancer
| Route | Details |
|---|---|
| Direct | Penetrates muscularis → serosa → adjacent organs (pancreas, colon, liver) |
| Lymphatic | To perigastric and then para-aortic nodes; may reach supraclavicular nodes (Troisier's/Virchow's sign) |
| Blood-borne | First to liver, then lung and bone; uncommon without prior nodal disease |
| Transperitoneal | Once serosa is reached; leads to ascites, peritoneal seedlings; ovarian metastases (Krukenberg's tumour); umbilical metastasis (Sister Joseph's nodule); pelvic "shelf" on rectal exam (Blumer's shelf) |
Key Prognostic Factors
- Depth of invasion (T stage) and nodal status (N stage) are the most important prognostic factors in resectable gastric cancer.
- At least 15 lymph nodes must be sampled from a resected specimen for adequate staging.
- Molecular biomarkers (HER2/ERBB2 amplification ~20-25%, PD-L1 status, MSI/dMMR, Claudin 18.2) now guide systemic therapy selection.
Harrison's Principles of Internal Medicine, 22E; Grainger & Allison's Diagnostic Radiology
Imaging for Staging
- MDCT (multi-detector CT) is the primary modality; criteria revised for 8th edition TNM
- MRI - limited experience; T1 WI shows intermediate signal in carcinoma; T2 WI shows low signal; abnormal focal thickening ≥6 mm is significant
- EUS (endoscopic ultrasound) - useful for T and N staging, especially early disease
- FDG-PET - used for detecting distant metastases
Grainger & Allison's Diagnostic Radiology
Can you make ppt presentation for the same topic
Reading File
Reading File
Reading File
Running Command
Writing File
Running Command
Editing File
Running Command
Running Command
Your presentation is ready! Download it here:
Stomach Cancer Types Staging
Presentation · PPTX
The deck is 15 slides with a medical/oncology color theme (deep navy, vivid red, gold accents):
| Slide | Content |
|---|---|
| 1 | Title slide |
| 2 | Epidemiology & overview (stat boxes) |
| 3 | Section divider - Types |
| 4 | Lauren Classification - Intestinal vs. Diffuse (side-by-side comparison) |
| 5 | Other tumour types: MALT lymphoma, GIST, NETs, SCC |
| 6 | Borrmann Classification (Types I-IV, visual columns) |
| 7 | Early Gastric Cancer - Japanese endoscopic classification (Types I, IIa, IIb, IIc, III) |
| 8 | Section divider - Staging |
| 9 | T Staging - tumour depth with colour-coded rows |
| 10 | N & M Staging |
| 11 | Overall Stage Grouping (IA → IV with 5-year survival estimates) |
| 12 | Routes of spread + clinical signs (Krukenberg, Virchow, Blumer, etc.) |
| 13 | Staging imaging modalities (MDCT, EUS, PET, MRI, Laparoscopy) |
| 14 | Molecular biomarkers & targeted therapy table (HER2, PD-L1, MSI, Claudin 18.2, CDH1) |
| 15 | Key take-home points summary |
This is a shared conversation. Sign in to Orris to start your own chat.