

17291.jpg
17293.jpg
Possible diagnosis from the xray provided
analyse_media
analyse_media
Reading File
Finding Sources
Finding Sources
Searching the Web
skull X-ray AP lateral normal findings differential diagnosis 50 year old male
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Now I have a comprehensive picture. Let me synthesize the findings with a detailed analysis.
Skull X-Ray Analysis - Peter Muriithi | Male | 50Y
Isiolo County Teaching and Referral Hospital
Views Provided
- AP (Anteroposterior) view - Image 1
- Lateral view - Image 2
Systematic Radiological Findings
What the AI vision analysis found on both views:
AP View:
- Calvarium bone density within normal limits; no gross lytic or blastic lesions
- Coronal/sagittal sutures normally fused for age
- Orbital rims intact bilaterally
- Frontal sinuses well-pneumatized, no air-fluid levels
- No obvious cortical disruptions or displaced fracture lines
- Soft tissues appear symmetric
Lateral View:
- Inner and outer tables intact and well-defined
- Sutures (coronal, lambdoid, squamosal) appear normally interdigitated
- Normal vascular grooves along inner table
- Frontal and sphenoid sinuses aerated
- Sella turcica appears normal - normal U-shape, no enlargement or floor erosion
- Cervical vertebrae C1-C6 visible with preserved disc spaces and alignment
- Prevertebral soft tissue within normal limits
Possible Diagnoses (Differential)
Given that both views show no gross acute abnormality, this study could represent:
1. Normal Skull Study (Most likely if this was a screening X-ray)
Both projections show a skull within expected parameters for a 50-year-old male. Plain skull X-rays are low-yield for most pathology at this age.
2. Early/Subclinical Paget's Disease of Bone (important to exclude)
- Paget's disease affects ~3% of people aged 40+ and predominantly males
- Early "lytic phase" can appear nearly normal on X-ray before the classic "cotton-wool" densities develop
- The textbook lateral view from Cummings Otolaryngology (shown above) demonstrates the thickened skull table with patchy densities - features that may be subtle in early disease
- Harrison's (2025) describes "cotton wool," osteoporosis circumscripta, thickening of diploic areas, and skull bone enlargement as hallmarks
- Clinical clues: elevated alkaline phosphatase, skull enlargement, hearing loss, headache
- Onset typically in the sixth decade of life - this patient at 50 is in the right age range
Textbook image for comparison (Paget skull - lateral view):
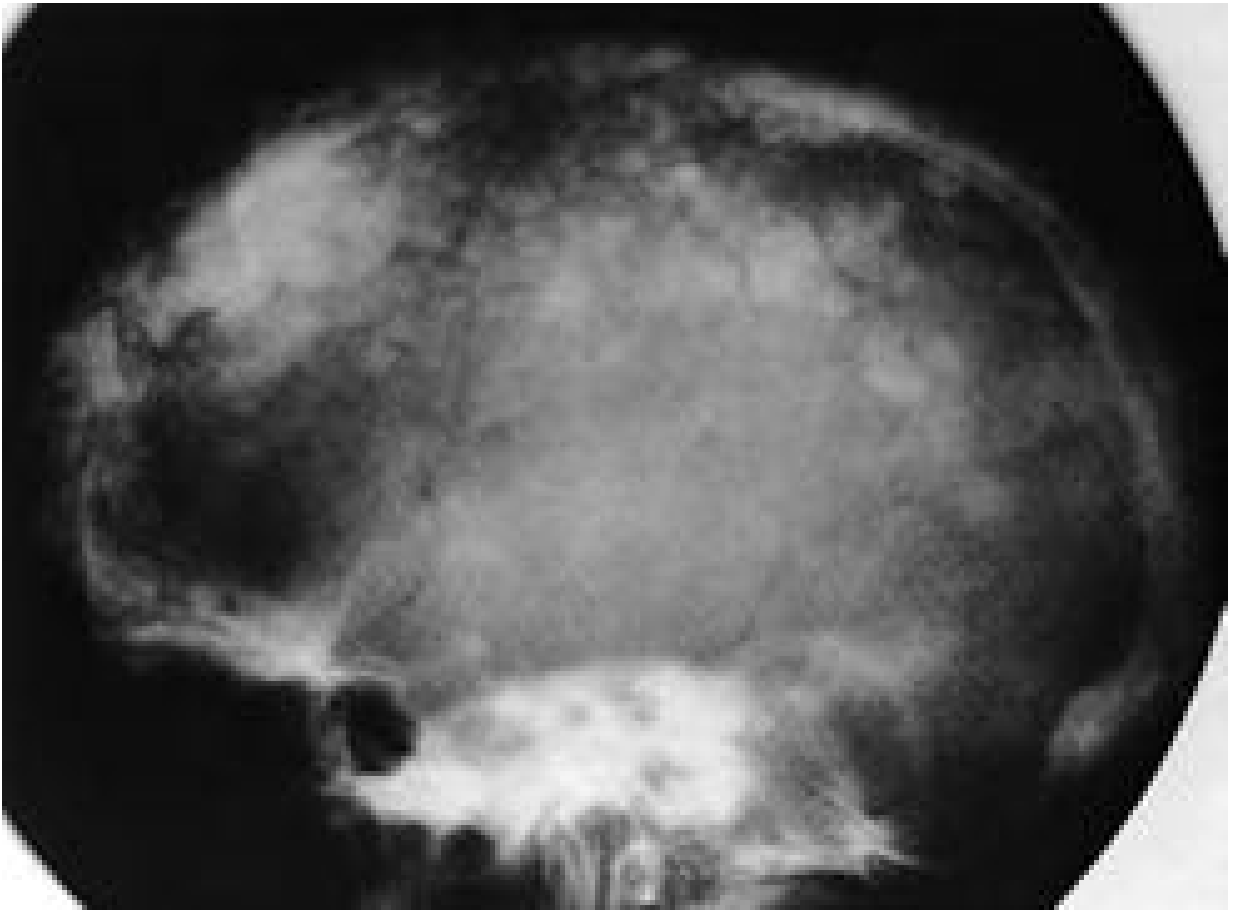 (Cummings Otolaryngology, Fig. 151.24 - Paget disease skull)
(Cummings Otolaryngology, Fig. 151.24 - Paget disease skull)
3. Post-traumatic Evaluation (No Fracture Identified)
- If taken after head injury, this study shows no gross fracture line, no sutural diastasis, no obvious air-fluid level in the sphenoid sinus (which would suggest basal skull fracture)
- Note: Plain X-rays miss up to 25-30% of skull fractures - CT is the gold standard for trauma
4. Raised Intracranial Pressure (ruled out on this X-ray)
- No sutural diastasis noted
- Sella turcica appears normal with no erosion of the dorsum sellae
- "Beaten silver" or "copper beaten" appearance not described
5. Fibrous Dysplasia
- Can present in adults as a ground-glass density change in the skull
- Usually monostotic in adults; no obvious expansion or ground-glass change noted here
Key Limitations
| Limitation | Implication |
|---|---|
| Single AP + lateral views only | Cannot fully characterize lesions - two-dimensional superimposition |
| Photo of a monitor, not DICOM | Reduces ability to detect subtle density changes |
| No clinical history provided | Diagnosis context unknown (trauma? headache? incidental?) |
| Plain X-ray is insensitive | CT head is far superior for fractures, intracranial pathology, and bone lesions |
Recommendations
- If trauma context - proceed to non-contrast CT head (plain X-ray is insufficient to exclude intracranial hemorrhage or subtle fracture)
- If bone disease suspected - order serum Alkaline Phosphatase (ALP) and bone-specific ALP; consider bone scan or MRI
- If neurological symptoms - MRI brain with gadolinium is indicated regardless of plain X-ray result
- Correlate clinically - the plain skull X-ray should not be used in isolation for any major diagnostic decision in a 50-year-old male
Disclaimer: This analysis is for educational and clinical support purposes only. Formal radiological reporting by a qualified radiologist is required for clinical decision-making.

17265.jpg
Possible diagnosis
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
right lung white out mediastinal shift toward opacity chest X-ray differential diagnosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have enough information from the vision analysis and clinical knowledge to provide a thorough response. Let me now compile the complete diagnosis.
Chest PA X-Ray Analysis
Patient: Abdirahman Roba | Male | 62Y
Institution: Isiolo County Teaching and Referral Hospital
View: Chest PA (Posteroanterior)
Key Radiological Findings
The Single Most Critical Finding: Right Hemithorax "White-Out" with Ipsilateral Mediastinal Shift
This is the dominant and diagnostically decisive observation:
| Feature | Finding |
|---|---|
| Right hemithorax | Dense homogeneous opacification (white-out) of the right mid-to-lower zones |
| Trachea | Deviated to the RIGHT (toward the opacity) |
| Mediastinum | Shifted rightward - heart pulled toward the opacity |
| Left lung | Compensatory hyperinflation - expanded, hyperlucent, crossing midline |
| Right ribs | Crowded - consistent with volume loss |
| Left costophrenic angle | Sharp and clear |
| Spine | S-shaped thoracolumbar scoliosis |
| Left diaphragm | Flattened (from left lung hyperinflation) |
The Diagnostic Key: Direction of Mediastinal Shift
This is a fundamental rule in reading "white-out" hemithorax X-rays:
Shift TOWARD the opacity = Volume LOSS (atelectasis/collapse/fibrosis) Shift AWAY from the opacity = Volume GAIN (effusion/mass/tension pneumothorax)
In this case, the trachea and mediastinum shift toward the right opacity - this confirms volume loss, not volume gain.
Differential Diagnosis (in order of likelihood)
1. Total/Near-Total Right Lung Collapse (Atelectasis) ⭐ Most Likely
- Complete airlessness of the right lung with ipsilateral mediastinal pull
- Most common cause at age 62: Endobronchial obstruction by right main bronchus carcinoma (lung cancer)
- Other causes: mucus plug, foreign body, post-intubation collapse
- The age (62M), smoking history (likely), and complete collapse pattern make central lung carcinoma the top concern
- Requires urgent bronchoscopy
2. Fibrothorax (Chronic Pleural Fibrosis) ⭐ Strong Contender
- Dense pleural thickening/fibrosis encasing the lung, causing chronic volume loss
- Common causes in this region: prior tuberculosis (very common in East Africa/Kenya), old empyema, old hemothorax
- Mediastinum pulled ipsilaterally over time
- The opacification may represent both collapsed lung AND thick fibrous peel
- TB fibrothorax is extremely common in Kenya and perfectly fits this picture
3. Post-Pneumonectomy State
- If the patient had a prior right lung removal (surgical history)
- Complete white-out + mediastinal shift ipsilaterally is the expected post-pneumonectomy appearance
- Requires clinical history to confirm
4. Chronic Empyema with Fibrothorax
- Long-standing infected pleural collection that has fibrosed and shrunk
- Would appear similar to fibrothorax; can also follow TB
5. Massive Atelectasis from Mucus Plugging / Bronchial Obstruction
- Less likely to cause this degree of collapse without an endobronchial lesion at age 62
Priority Diagnoses to Rule Out
Given the patient demographics (62-year-old male, East Africa), the top two diagnoses that must be urgently distinguished are:
| Diagnosis | Key Investigation |
|---|---|
| Right main bronchus carcinoma | CT chest with contrast + bronchoscopy + biopsy |
| Post-TB fibrothorax | TB history, sputum AFB/GeneXpert, CT chest |
Recommended Investigations
- CT chest with IV contrast - mandatory to characterize the right side (distinguish collapse, fibrosis, mass, effusion component)
- Bronchoscopy - if endobronchial obstruction suspected; may allow direct visualization and biopsy
- Sputum for AFB/GeneXpert and TB culture - given high TB prevalence in Kenya
- Complete history - prior TB, smoking history, previous chest surgery, weight loss, hemoptysis
- Spirometry/PFTs - to assess left lung reserve
- Serum LDH, FBC, inflammatory markers
Summary
This X-ray shows a right hemithorax white-out with ipsilateral (rightward) tracheal and mediastinal shift, confirming volume loss as the mechanism. The left lung is compensatorily hyperinflated. In a 62-year-old male in Kenya, the leading diagnoses are:
- Right lung collapse secondary to endobronchial carcinoma (urgent)
- Post-TB fibrothorax (chronic, very prevalent in this region)
Urgent CT chest and pulmonology/thoracic surgery referral is strongly recommended. This X-ray should not be managed without further imaging.
Disclaimer: This is an AI-assisted educational analysis. Formal reporting by a qualified radiologist and clinical correlation are required for all management decisions.
This is a shared conversation. Sign in to Orris to start your own chat.