About hysterectomy
Reading File
Finding Sources
Searching PubMed
"hysterectomy"[MeSH Terms] AND "indications OR complications OR techniques"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Hysterectomy - A Comprehensive Overview
Definition
Hysterectomy is the surgical removal of the uterus. It is one of the most commonly performed surgical procedures in the United States, with uterine leiomyoma and abnormal uterine bleeding accounting for the largest share of cases.
- Berek & Novak's Gynecology, p. 1409; Sabiston Textbook of Surgery, p. 2799
Types of Hysterectomy
By Extent of Removal
| Type | What is Removed |
|---|---|
| Total hysterectomy | Uterine corpus + cervix |
| Supracervical (subtotal) hysterectomy | Uterine corpus only; cervix left in situ |
| Radical hysterectomy | Uterus + cervix + parametria + upper vagina (for cervical cancer) |
| Simple hysterectomy | Uterus + cervix without parametrial dissection |
Note on supracervical hysterectomy: There is no demonstrated advantage over total hysterectomy for benign disease. Cervical cancer screening must continue after supracervical hysterectomy. It is contraindicated when malignant or premalignant disease of the uterus or cervix is present.
- Sabiston Textbook of Surgery, p. 2799; Berek & Novak's Gynecology, Key Points
By Surgical Route
| Route | Key Features |
|---|---|
| Vaginal hysterectomy (VH) | Preferred route unless contraindicated; earliest described technique; colpotomy done first, cornual pedicles last |
| Total abdominal hysterectomy (TAH) | Open approach via low transverse (Pfannenstiel) or vertical midline incision |
| Laparoscopic hysterectomy (LH) | Minimally invasive; similar or lower complication rate to VH; shorter stay, less pain than TAH |
| Robotic-assisted laparoscopic hysterectomy | Similar to LH; lower conversion rates; higher cost; no proven advantage over conventional laparoscopy in RCTs |
| Laparoendoscopic single-site (LESS) | Single incision variant |
Key rule on route selection:
"Vaginal hysterectomy is the procedure of choice unless this route is contraindicated. LH offers no advantage for women in whom VH is possible... The ideal place for LH is as a replacement for laparotomy."
- Berek & Novak's Gynecology, p. 1297, Key Points
Laparotomy-based hysterectomy is now reserved for a minority of patients, including those with cardiopulmonary disease contraindicating laparoscopy, or when anatomy is severely distorted by adhesions or uterine disease.
- Berek & Novak's Gynecology, p. 1297
Surgical Steps (Abdominal Approach)
Key steps in sequence:
- Divide round ligaments (bilaterally) with electrocautery or ligature
- Incise anterior leaf of broad ligament, develop bladder flap
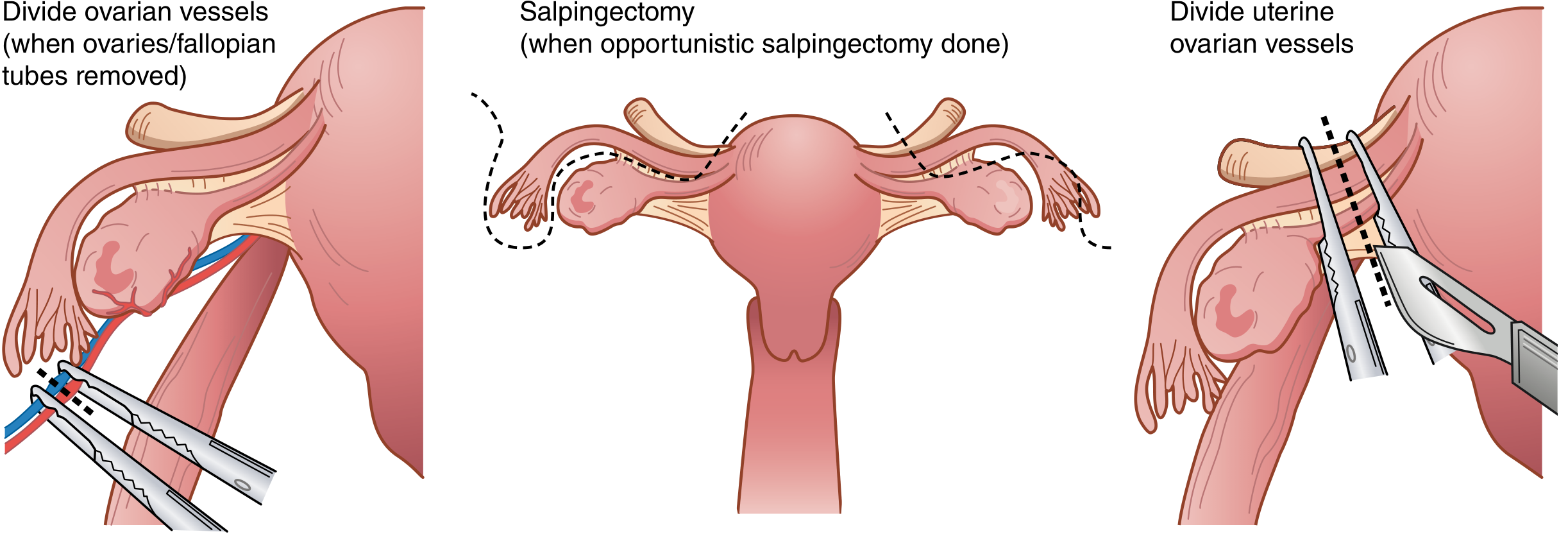
- If salpingo-oophorectomy is planned: identify ureters, doubly clamp and divide infundibulopelvic ligaments (ovarian vessels)
- If ovaries are to be preserved: clamp utero-ovarian vessels
- Dissect bladder off the cervix inferiorly
- Clamp, divide, and suture-ligate uterine vessels at the internal cervical os
- Serially clamp and divide cardinal and uterosacral ligaments
- Perform colpotomy (circumferential incision around cervix at vaginal junction)
- Close vaginal cuff with interrupted or running absorbable sutures, incorporating uterosacral ligaments for apical support
Sabiston Textbook of Surgery, p. 2799-2800
Indications
Benign Indications
From the US National Hospital Discharge Survey 2010 (top causes):
| Indication | Number of Hysterectomies (2010) |
|---|---|
| Uterine leiomyoma (fibroids) | 195,000 |
| Abnormal uterine bleeding | 195,000 |
| Endometriosis | 83,000 |
| Uterovaginal prolapse | - |
| Chronic pelvic pain / adenomyosis | - |
| Pelvic inflammatory disease | - |
| Pelvic organ prolapse | - |
Other benign indications include:
- Intractable dysmenorrhea
- Cervical intraepithelial neoplasia (CIN) - as treatment of last resort for recurrent high-grade CIN
- Obstetric emergencies (e.g., uterine rupture, intractable postpartum hemorrhage)
- Benign ovarian/pelvic masses
For chronic pelvic pain: ACOG requires at least 6 months of pelvic pain without correctable pathology before proceeding with hysterectomy. ~25% of women with central pelvic pain may have persistent or worsened pain postoperatively.
- Berek & Novak's Gynecology, p. 605
Malignant/Premalignant Indications
- Endometrial carcinoma
- Cervical carcinoma (radical hysterectomy)
- Recurrent/refractory CIN
- Uterine sarcoma
Concomitant Procedures
- Bilateral salpingo-oophorectomy (BSO): Optional. In premenopausal women with average ovarian cancer risk, oophorectomy at hysterectomy is associated with increased long-term mortality from cardiovascular disease - ovarian conservation should be strongly considered.
- Opportunistic salpingectomy: Bilateral salpingectomy is increasingly performed at the time of hysterectomy to reduce ovarian cancer risk (the fallopian tube is implicated in the pathogenesis of high-grade serous carcinoma).
- Sentinel lymph node (SLN) mapping: For endometrial cancer, indocyanine green (ICG) injected into the cervix at 3 and 9 o'clock positions, traced to pelvic nodes; preferred over full lymphadenectomy to reduce morbidity.
- McCall culdoplasty: Performed at vaginal hysterectomy for apical support.
Preoperative Considerations
- Health assessment including cardiopulmonary fitness
- Total vs. supracervical: No routine advantage to supracervical; avoid if cervical/uterine pathology present
- Route decision: Based on anatomy, uterine size/disease, patient wishes, surgeon training
- Concurrent procedures: Pelvic floor repair, appendectomy, cholecystectomy, abdominoplasty
- Tissue morcellation: Avoid if malignancy is known or suspected (risk of disseminating occult malignancy)
Postoperative Complications
Intraoperative
- Hemorrhage (1.4-2.6% in vaginal hysterectomy)
- Urinary tract injury (ureter, bladder)
- Bowel injury
- Conversion to open approach (laparoscopic cases)
Postoperative
| Complication | Notes |
|---|---|
| Hemorrhage | Can require re-operation |
| Urinary retention | Common in early postop period |
| Ureteral injury | Risk especially with distorted anatomy |
| Vesicovaginal fistula | Presents as continuous urine leak vaginally |
| Vaginal cuff dehiscence | Risk higher after laparoscopic hysterectomy |
| Incisional pain & infections | Wound infections, cuff cellulitis |
| Prolapse of the fallopian tube | Through vaginal cuff |
| DVT/PE | Standard surgical risk |
Berek & Novak's Gynecology, p. 1408; Campbell-Walsh-Wein Urology
Route Comparison Summary
| Feature | Vaginal | Laparoscopic | Abdominal |
|---|---|---|---|
| Complication rate | Lowest | Low (similar to VH) | Highest |
| Hospital stay | Shortest | Short | Longest |
| Postoperative pain | Least | Less | Most |
| Cost | Lowest | Higher | Intermediate |
| Recovery time | Fastest | Fast | Slowest |
| Hospital readmission | Comparable | Lowest (some data) | Higher |
| Quality of life at 12 months | Best | Best | Lower |
Berek & Novak's Gynecology, p. 1297; Cochrane Systematic Review 2023
Key Points (Evidence-Based)
- Hysterectomy is one of the most commonly performed surgeries in the US.
- Vaginal hysterectomy is the preferred route unless contraindicated.
- Randomized clinical trials do not show any advantage of robotic or single-port hysterectomy over conventional laparoscopic hysterectomy.
- There is no routine advantage to supracervical over total hysterectomy.
- Bilateral salpingo-oophorectomy at hysterectomy in premenopausal women at average risk increases long-term mortality from cardiovascular disease - ovarian conservation is strongly recommended.
- Opportunistic salpingectomy at time of hysterectomy is encouraged to reduce ovarian cancer risk.
Recent Evidence (2023-2024)
- A 2023 Cochrane systematic review on surgical approaches to hysterectomy for benign disease confirms the minimally invasive advantage over laparotomy (PMID 37642285).
- A 2024 meta-analysis on long-term outcomes of hysterectomy with bilateral salpingo-oophorectomy found significant associations with cardiovascular and metabolic morbidity when performed in premenopausal women (PMID 37364803).
- A 2023 JAMA Surgery systematic review supports opportunistic salpingectomy at time of hysterectomy for primary prevention of ovarian cancer (PMID 37672283).
Sources: Berek & Novak's Gynecology (9781496380357); Sabiston Textbook of Surgery, 21st Ed. (9780443124341); Campbell-Walsh-Wein Urology (9780323546423)
This is a shared conversation. Sign in to Orris to start your own chat.