A 15-year-old boy presents to his physician with a history of chronic fatigue and intermittent jaundice, which he notes is more pronounced after febrile illness. His family history is significant for a paternal uncle who required a splenectomy for a similar lifelong condition. Laboratory tests reveal a persistent normocytic anemia with a high reticulocyte count. This patient's condition is most likely caused by a congenital enzyme deficiency in which of the following metabolic pathways? The answer was glycolysis. So this topic, the question is based on congenital hemolytic anemia, which can be caused due to enzyme deficiencies in the glycolytic pathway as well as another case with changes, issues in the HMP shunt pathway. So regarding this question, what more info should I learn regarding these congenital hemolytic anemias for complete NEET PG pathology coverage?
pyruvate kinase deficiency hemolytic anemia glycolysis enzyme deficiency congenital
G6PD deficiency HMP shunt hemolytic anemia pathophysiology diagnosis
Congenital Hemolytic Anemias — Enzyme Deficiency Type
Overview: The Two Pathways
| Feature | Glycolytic Pathway | HMP Shunt (Pentose Phosphate Pathway) |
|---|---|---|
| Key enzyme deficient | Pyruvate Kinase (PK) (most common glycolytic) | G6PD (most common overall) |
| Type of hemolysis | Chronic, non-spherocytic | Episodic/acute (triggered) |
| Inheritance | Autosomal recessive | X-linked recessive |
| RBC morphology | Echinocytes (burr cells) | Bite cells, blister cells, Heinz bodies |
| Coombs test | Negative | Negative |
Per Harrison's (p. 2985): Prevalence order of enzyme deficiencies causing hemolysis — G6PD > Pyruvate Kinase > G6P Isomerase > others
1. Pyruvate Kinase (PK) Deficiency — Glycolysis
Pathophysiology
- PK catalyzes the last step of glycolysis: PEP → Pyruvate + ATP
- Deficiency → ↓ ATP in RBCs → membrane pump failure (Na⁺/K⁺ ATPase) → RBC dehydration & rigidity → extravascular hemolysis (spleen)
- Also: ↑ 2,3-BPG (substrate backs up upstream) — paradoxically shifts O₂ dissociation curve rightward (better O₂ unloading), which is why symptoms are less severe than expected for the degree of anemia
Clinical Features
- Chronic hemolytic anemia from birth/childhood
- Jaundice (intermittent, worsened by infection/febrile illness)
- Splenomegaly (chronic extravascular hemolysis)
- Positive family history — autosomal recessive (parental uncle having splenectomy fits)
- Aplastic crisis precipitated by Parvovirus B19
- Cholelithiasis (pigment stones) — chronic hemolysis → ↑ unconjugated bilirubin
Labs
| Parameter | Finding |
|---|---|
| Hemoglobin | Low |
| MCV | Normocytic (normal) |
| Reticulocytes | Markedly elevated |
| Peripheral smear | Echinocytes (burr/spiculated cells) |
| Bilirubin | ↑ Indirect (unconjugated) |
| LDH | ↑ |
| Haptoglobin | ↓ |
| Coombs test | Negative |
| Osmotic fragility | Normal or decreased |
Confirmatory Test
- Fluorescent spot test (screening) — no fluorescence with PK deficiency
- Enzyme assay — quantitative PK activity (definitive)
Treatment
- Splenectomy — reduces hemolytic rate (spleen is the main site of destruction); indicated in transfusion-dependent cases
- Regular folic acid supplementation
- Blood transfusions for aplastic crises
- Mitapivat (pyruvate kinase activator) — newer drug, activates mutant PK enzyme
2. G6PD Deficiency — HMP Shunt
Pathophysiology
- G6PD is the rate-limiting enzyme of the HMP shunt
- Its product (NADPH) regenerates glutathione (GSH), which neutralizes oxidative stress in RBCs
- Deficiency → ↓ NADPH → ↓ GSH → oxidative damage to Hb → Hb denaturation → Heinz bodies → RBC membrane damage → intravascular + extravascular hemolysis
Inheritance
- X-linked recessive → males predominantly affected; females are carriers (lyonization can cause variable expression in females)
Common Triggers (must memorize for NEET PG)
| Category | Examples |
|---|---|
| Drugs | Primaquine, dapsone, nitrofurantoin, rasburicase, methylene blue, sulfonamides |
| Infections | Fever/any infection (most common trigger globally) |
| Foods | Fava beans (favism) — particularly in Mediterranean variant |
| Others | Metabolic acidosis, naphthalene (moth balls) |
Clinical Variants (NEET PG High Yield)
| Variant | Ethnicity | Severity | Notes |
|---|---|---|---|
| A- (African) | African descent | Mild | Enzyme unstable in old RBCs; young RBCs spared → self-limiting hemolysis |
| Mediterranean | Southern Europe, Middle East, India | Severe | Low enzyme activity in ALL cells; severe hemolysis, favism |
| Canton | Southeast Asia | Moderate-severe | — |
Clinical Features
- Episodic hemolytic anemia — triggered, not chronic (unlike PK deficiency)
- Neonatal jaundice (can be severe enough to cause kernicterus)
- Back/abdominal pain during acute episode (intravascular hemolysis → hemoglobinuria → dark urine)
- Splenomegaly is NOT prominent (unlike PK deficiency)
Labs
| Parameter | Finding |
|---|---|
| Hemoglobin | Acute drop during attack |
| Reticulocytes | ↑ (post-crisis) |
| Peripheral smear | Bite cells (degmacytes), blister cells, Heinz bodies (with supravital stain — crystal violet) |
| Urine | Hemoglobinuria (dark/cola-colored) |
| Coombs test | Negative |
Confirmatory Test
- Fluorescent spot test (screening) — no fluorescence indicates G6PD deficiency
- Quantitative G6PD assay — must be done 4–6 weeks after acute episode (because young RBCs released post-hemolysis have higher G6PD activity and can give false-normal results during attack)
- DNA testing — for heterozygous females
Treatment
- Avoid triggers (educate patient)
- Supportive care during acute hemolytic episode
- Blood transfusion if severe
- No role for splenectomy
- Folic acid supplementation
3. Other Glycolytic Enzyme Deficiencies (Lower Yield, but Know for Completeness)
| Enzyme | Special Feature |
|---|---|
| Glucose-6-phosphate isomerase | 2nd most common glycolytic defect; AR; chronic hemolysis |
| Aldolase | Very rare; associated with myopathy |
| Triose phosphate isomerase | Rare; associated with severe neurological disease + hemolysis (most lethal) |
| Phosphoglycerate kinase | X-linked; hemolysis + CNS dysfunction |
4. Key Comparisons — High Yield Table for NEET PG
| Feature | PK Deficiency | G6PD Deficiency |
|---|---|---|
| Pathway | Glycolysis | HMP Shunt |
| Inheritance | AR | X-linked recessive |
| Hemolysis type | Chronic | Episodic/acute |
| Smear | Echinocytes | Bite cells, Heinz bodies |
| Triggers | Infections (aplastic crisis with Parvo B19) | Drugs, infections, fava beans |
| 2,3-BPG | ↑ (protective; right shift of ODC) | Normal |
| Splenomegaly | Yes | Minimal |
| Splenectomy | Beneficial | Not indicated |
| Neonatal jaundice | Yes | More prominent |
| Dark urine | Rare | Yes (hemoglobinuria) |
| Lab timing of enzyme assay | Anytime | Only after 4–6 weeks post-attack |
5. Distinguishing from Other Hemolytic Anemias
- Hereditary Spherocytosis (HS): Defect in spectrin/ankyrin/band 3 (membrane, not enzyme); spherocytes on smear; ↑ osmotic fragility; AR/AD
- Sickle Cell Disease: Structural Hb defect; sickle cells; vaso-occlusion
- Thalassemia: Quantitative Hb synthesis defect; microcytic, target cells
- Autoimmune Hemolytic Anemia (AIHA): Coombs POSITIVE — key differentiator from all enzyme deficiencies
6. NEET PG Exam Traps & High-Yield Points
- PK deficiency → ↑ 2,3-BPG → rightward shift of ODC → better O₂ delivery → symptoms milder than anemia degree suggests
- G6PD assay timing: Do NOT test during acute hemolytic episode — will miss diagnosis (young reticulocytes have higher activity → false negative)
- Heinz bodies are seen with supravital stains (crystal violet, brilliant cresyl blue), NOT routine Giemsa stain
- Favism = G6PD deficiency triggered by fava beans — Mediterranean variant
- Bite cells on smear = macrophages in spleen "bite off" Heinz body-containing portions of RBC
- Triose phosphate isomerase deficiency = only glycolytic enzyme defect with neurological involvement
- Neonatal jaundice requiring phototherapy/exchange transfusion in a male infant — think G6PD deficiency
- In the question stem: "worsened by febrile illness" + "chronic" + "family history/splenectomy" + "AR pattern" = PK deficiency (glycolysis)
- "Episodic" + "drug/food trigger" + "male" + "dark urine" = G6PD deficiency (HMP shunt)
Could you give me a very short summary of this about topic, but it should include everything that will help me to answer an EPG 2026 quiz regarding this topic. I mean, regarding the pathology aspect of this topic.
congenital hemolytic anemia enzyme deficiency glycolysis HMP shunt pathology key points
Congenital Hemolytic Anemia — Enzyme Deficiencies (NEET PG Rapid Recap)
Glycolysis — Pyruvate Kinase (PK) Deficiency
- AR, most common glycolytic defect
- ↓ ATP → membrane pump failure → extravascular hemolysis (spleen)
- ↑ 2,3-BPG → right shift ODC → anemia better tolerated than expected
- Chronic hemolysis; worsens with infection/fever
- Smear: Echinocytes (burr cells); Coombs negative
- Splenomegaly + pigment gallstones; aplastic crisis with Parvovirus B19
- Rx: Splenectomy helpful; folic acid; Mitapivat (new)
HMP Shunt — G6PD Deficiency
- X-linked recessive (males affected; females carriers)
- ↓ NADPH → ↓ GSH → oxidative Hb damage → Heinz bodies → bite cells
- Episodic hemolysis, triggered by: drugs (primaquine, dapsone, sulfonamides), infections, fava beans
- Smear: Bite cells + Heinz bodies (supravital stain only); Coombs negative
- Dark urine (hemoglobinuria); prominent neonatal jaundice
- Enzyme assay: Wait 4–6 weeks post-attack (false normal during attack)
- Rx: Avoid triggers; splenectomy not helpful
The One Differentiator
| PK Deficiency | G6PD Deficiency | |
|---|---|---|
| Hemolysis | Chronic | Episodic |
| Trigger | Infection (chronic) | Drugs/fava beans/fever |
| Smear | Echinocytes | Bite cells, Heinz bodies |
| Splenectomy | ✅ Beneficial | ❌ Not indicated |
| Inheritance | AR | X-linked recessive |
- Heinz bodies → supravital stain only (missed on routine smear)
- ↑ 2,3-BPG in PK deficiency = right shift = milder symptoms
- Triose phosphate isomerase deficiency = only glycolytic defect with neuro involvement
- Coombs negative in ALL enzyme deficiencies (positive = AIHA)
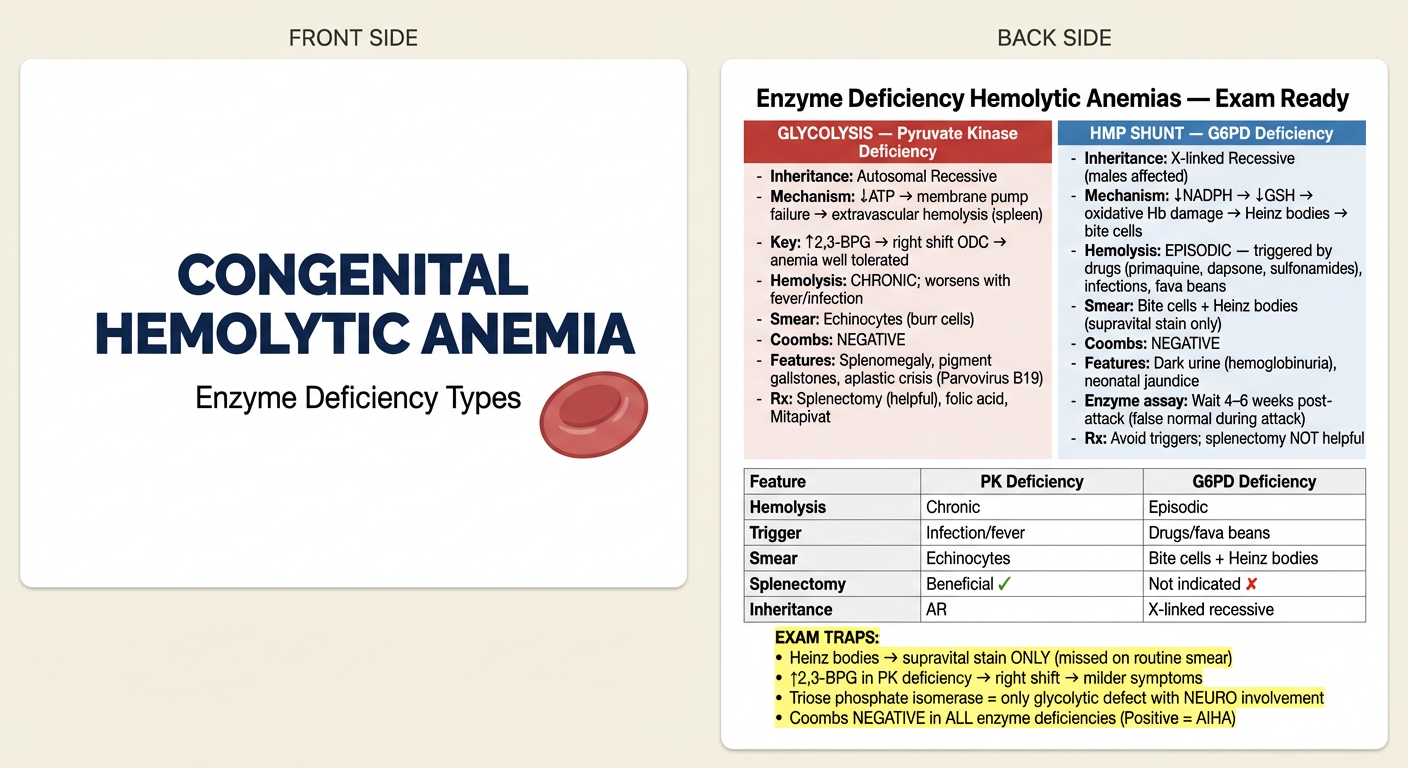
Can you convert this topic into a monkey card? Front portion should be congenital hemolytic anemia. Back portion should be the complete explanation, which is an exam ready. It should be an exam ready read involving the pathology of this condition.
A medical flashcard (Anki-style monkey card) with two sides shown vertically. FRONT SIDE (top half): Clean white background with a bold centered title "CONGENITAL HEMOLYTIC ANEMIA" in large dark navy text. Below it in smaller text: "Enzyme Deficiency Types" with a subtle red blood cell icon. BACK SIDE (bottom half): Light cream/white background, dense but clean medical study notes layout. Title: "Enzyme Deficiency Hemolytic Anemias — Exam Ready" in bold dark text. Two columns side by side: LEFT COLUMN header (red): "GLYCOLYSIS — Pyruvate Kinase Deficiency" - Inheritance: Autosomal Recessive - Mechanism: ↓ATP → membrane pump failure → extravascular hemolysis (spleen) - Key: ↑2,3-BPG → right shift ODC → anemia well tolerated - Hemolysis: CHRONIC; worsens with fever/infection - Smear: Echinocytes (burr cells) - Coombs: NEGATIVE - Features: Splenomegaly, pigment gallstones, aplastic crisis (Parvovirus B19) - Rx: Splenectomy (helpful), folic acid, Mitapivat RIGHT COLUMN header (blue): "HMP SHUNT — G6PD Deficiency" - Inheritance: X-linked Recessive (males affected) - Mechanism: ↓NADPH → ↓GSH → oxidative Hb damage → Heinz bodies → bite cells - Hemolysis: EPISODIC — triggered by drugs (primaquine, dapsone, sulfonamides), infections, fava beans - Smear: Bite cells + Heinz bodies (supravital stain only) - Coombs: NEGATIVE - Features: Dark urine (hemoglobinuria), neonatal jaundice - Enzyme assay: Wait 4–6 weeks post-attack (false normal during attack) - Rx: Avoid triggers; splenectomy NOT helpful Bottom comparison table with 5 rows: Feature | PK Deficiency | G6PD Deficiency Hemolysis | Chronic | Episodic Trigger | Infection/fever | Drugs/fava beans Smear | Echinocytes | Bite cells + Heinz bodies Splenectomy | Beneficial ✓ | Not indicated ✗ Inheritance | AR | X-linked recessive EXAM TRAPS box at bottom (yellow highlight): • Heinz bodies → supravital stain ONLY (missed on routine smear) • ↑2,3-BPG in PK deficiency → right shift → milder symptoms • Triose phosphate isomerase = only glycolytic defect with NEURO involvement • Coombs NEGATIVE in ALL enzyme deficiencies (Positive = AIHA)
Is the above image better for revision or is it converting the information into an anki card?
- Front = a single question or cue that forces active recall
- Back = the answer, revealed only after you attempt to recall it
- The challenge-response mechanism is what builds memory
- e.g., Front: "What is the smear finding in PK deficiency?" → Back: "Echinocytes (burr cells)"
- Best for active recall and spaced repetition
- Everything on one visual sheet
- Best for quick review before an exam
- Front: "Congenital Hemolytic Anemia — Enzyme Deficiencies"
- Back: Concise, well-organized bullet points — not dense paragraphs
Which is better for spaced repetition and actually remembering the topic and at the same time revising very fastly and
Option A — Multiple Anki Cards (one concept per card)
- Your brain is forced to retrieve a specific fact
- You can rate each card (easy/hard) — hard cards come back sooner
- You identify weak spots precisely (e.g., you know G6PD triggers but keep forgetting the enzyme assay timing)
- You flip through cards rapidly
- Easy cards get dismissed quickly
- Only weak cards slow you down
- Total revision of a topic takes 5–10 minutes once cards are mature
The Ideal Card Structure for This Topic
| Front | Back |
|---|---|
| PK deficiency — inheritance? | Autosomal Recessive |
| PK deficiency — mechanism of hemolysis? | ↓ATP → membrane pump failure → extravascular hemolysis |
| Why is PK deficiency anemia well tolerated? | ↑2,3-BPG → right shift ODC → better O₂ delivery |
| G6PD deficiency — smear findings? | Bite cells + Heinz bodies (supravital stain only) |
| G6PD enzyme assay — when to test? | 4–6 weeks after acute attack |
| ...and so on |
Yeah, give me that, and also for the Hmp shunt.
🔴 GLYCOLYSIS — Pyruvate Kinase Deficiency
🔵 HMP SHUNT — G6PD Deficiency
⚡ EXAM TRAP CARDS
When I copy paste this, they are showing 88 cards. Can you format it in a better way so that it shows only 22 cards?
.txt file:.txt file, then import into Anki with semicolon as the separator:PK deficiency — which metabolic pathway and inheritance?;Glycolysis | Autosomal Recessive
PK deficiency — exact enzyme defect and its normal function?;Pyruvate Kinase | Catalyzes last step of glycolysis: PEP → Pyruvate + ATP
PK deficiency — mechanism of hemolysis?;↓ATP → Na⁺/K⁺ ATPase pump failure → RBC dehydration + rigidity → extravascular hemolysis in spleen
Why is anemia in PK deficiency better tolerated than expected?;Metabolic block → ↑2,3-BPG → right shift of O₂ dissociation curve → better O₂ delivery to tissues
PK deficiency — type of hemolysis and triggers?;CHRONIC hemolysis | Worsens with fever/infection | Aplastic crisis triggered by Parvovirus B19
PK deficiency — peripheral smear finding?;Echinocytes (burr cells) | Coombs NEGATIVE
PK deficiency — complications?;Splenomegaly | Pigment gallstones | Aplastic crisis (Parvovirus B19)
PK deficiency — confirmatory test?;Quantitative PK enzyme assay | Fluorescent spot test (screening — no fluorescence = deficient)
PK deficiency — treatment?;Splenectomy (beneficial) | Folic acid | Mitapivat (activates mutant PK) | Transfusion for aplastic crisis
G6PD deficiency — which pathway and inheritance?;HMP Shunt (Pentose Phosphate Pathway) | X-linked Recessive — males affected, females carriers
G6PD deficiency — mechanism of hemolysis?;↓G6PD → ↓NADPH → ↓GSH → oxidative Hb damage → Heinz bodies → RBC membrane damage → hemolysis
G6PD deficiency — type of hemolysis and triggers?;EPISODIC | Drugs (primaquine, dapsone, nitrofurantoin, sulfonamides) | Infections (most common globally) | Fava beans | Naphthalene
G6PD deficiency — peripheral smear findings and how are Heinz bodies visualized?;Bite cells + Blister cells + Heinz bodies | Heinz bodies: supravital stain ONLY (crystal violet/brilliant cresyl blue) — NOT on routine Giemsa
What are bite cells and how do they form?;Splenic macrophages bite off Heinz body-containing portions of RBC → bite cells (degmacytes)
G6PD deficiency — clinical features?;Episodic hemolytic anemia | Dark urine (hemoglobinuria) | Back/abdominal pain | Neonatal jaundice (kernicterus risk) | Minimal splenomegaly
G6PD deficiency — when to perform enzyme assay and why?;Wait 4–6 weeks after acute attack | During attack young reticulocytes have higher G6PD activity → false normal result
G6PD deficiency — variants, ethnicity, severity?;A- (African) mild self-limiting | Mediterranean severe favism all RBCs affected | Canton (SE Asian) moderate-severe
G6PD deficiency — treatment?;Avoid triggers | Supportive care | Transfusion if severe | Folic acid | Splenectomy NOT indicated
Which glycolytic enzyme deficiency causes neurological involvement plus hemolysis?;Triose Phosphate Isomerase (TPI) deficiency — rarest and most lethal
How to differentiate enzyme deficiency hemolytic anemias from AIHA on one test?;Coombs test — NEGATIVE in all enzyme deficiencies | POSITIVE in AIHA
Prevalence order of RBC enzyme deficiencies causing hemolysis?;G6PD > Pyruvate Kinase > G6P Isomerase > others
PK deficiency vs G6PD deficiency — splenectomy useful in which?;PK deficiency — YES (extravascular hemolysis in spleen) | G6PD deficiency — NO
- Save the above as
hemolytic_anemia.txt - Open Anki → File → Import
- Select the file
- Set Field separator: Semicolon
- Map Field 1 → Front, Field 2 → Back
- Import — you will get exactly 22 cards

Convert the information to Anki cards, front and back format. Also add anything regarding reticulocytes which are important for NEET PG 2026.
reticulocyte count corrected reticulocyte index production index hemolytic anemia
.txt and import with semicolon as separator.What are reticulocytes?;Non-nucleated red cell precursors | Have blue-red polychromatophilic cytoplasm due to residual ribosomal RNA (mesh-like reticular network)
How are reticulocytes visualized on smear?;Supravital stains — methylene blue or brilliant cresyl blue | Stain the ribosomal RNA | NOT seen on routine Giemsa stain
What is the normal reticulocyte count?;0.5–1.5% of total red cells
What does reticulocytosis indicate?;Effective erythropoiesis — good bone marrow response to anemia | Seen in: Hemolytic anemias | Acute blood loss
What does reticulocytopenia indicate?;Ineffective erythropoiesis — poor bone marrow response | Seen in: Aplastic anemia | Chemotherapy | Bone marrow malignancy | Anemia of chronic disease | Iron deficiency anemia | Vitamin B12/Folate deficiency
Why is reticulocyte count HIGH in hemolytic anemias like PK and G6PD deficiency?;Increased RBC destruction → bone marrow compensates → releases more reticulocytes into circulation (effective erythropoiesis)
What is the corrected reticulocyte count formula and why is it used?;Corrected count = Reticulocyte% × (Patient Hb/Normal Hb i.e. 15) | Raw % is falsely high in anemia because fewer total RBCs; correction adjusts for this
What is Reticulocyte Production Index (RPI) and its interpretation?;RPI = Corrected reticulocyte count ÷ Maturation factor | RPI >3 = Hemolytic anemia or acute blood loss (hyperproliferative) | RPI <2 = Hypoproliferative anemia (iron deficiency, aplastic, B12/folate deficiency)
What is polychromasia on routine smear and what does it represent?;Blue-tinged RBCs on Giemsa stain = reticulocytes released early from marrow | Indicates stress erythropoiesis / active hemolysis
PK deficiency — which metabolic pathway and inheritance?;Glycolysis | Autosomal Recessive
PK deficiency — exact enzyme defect and its normal function?;Pyruvate Kinase | Catalyzes last step of glycolysis: PEP → Pyruvate + ATP
PK deficiency — mechanism of hemolysis?;↓ATP → Na⁺/K⁺ ATPase pump failure → RBC dehydration + rigidity → extravascular hemolysis in spleen
Why is anemia in PK deficiency better tolerated than expected?;Metabolic block → ↑2,3-BPG → right shift of O₂ dissociation curve → better O₂ delivery to tissues
PK deficiency — type of hemolysis and triggers?;CHRONIC hemolysis | Worsens with fever/infection | Aplastic crisis triggered by Parvovirus B19
PK deficiency — peripheral smear finding?;Echinocytes (burr cells) | Coombs NEGATIVE | HIGH reticulocyte count
PK deficiency — complications?;Splenomegaly | Pigment gallstones | Aplastic crisis (Parvovirus B19)
PK deficiency — confirmatory test?;Quantitative PK enzyme assay | Fluorescent spot test (screening — no fluorescence = deficient)
PK deficiency — treatment?;Splenectomy (beneficial) | Folic acid | Mitapivat (activates mutant PK) | Transfusion for aplastic crisis
G6PD deficiency — which pathway and inheritance?;HMP Shunt (Pentose Phosphate Pathway) | X-linked Recessive — males affected, females carriers
G6PD deficiency — mechanism of hemolysis?;↓G6PD → ↓NADPH → ↓GSH → oxidative Hb damage → Heinz bodies → RBC membrane damage → hemolysis
G6PD deficiency — type of hemolysis and triggers?;EPISODIC | Drugs (primaquine, dapsone, nitrofurantoin, sulfonamides) | Infections (most common globally) | Fava beans | Naphthalene
G6PD deficiency — peripheral smear findings and how are Heinz bodies visualized?;Bite cells + Blister cells + Heinz bodies | Heinz bodies: supravital stain ONLY (crystal violet/brilliant cresyl blue) — NOT on routine Giemsa
What are bite cells and how do they form?;Splenic macrophages bite off Heinz body-containing portions of RBC → bite cells (degmacytes)
G6PD deficiency — clinical features?;Episodic hemolytic anemia | Dark urine (hemoglobinuria) | Back/abdominal pain | Neonatal jaundice (kernicterus risk) | Minimal splenomegaly | HIGH reticulocytes post-attack
G6PD deficiency — when to perform enzyme assay and why?;Wait 4–6 weeks after acute attack | During attack young reticulocytes have higher G6PD activity → false normal result
G6PD deficiency — variants, ethnicity, severity?;A- (African) mild self-limiting | Mediterranean severe favism all RBCs affected | Canton (SE Asian) moderate-severe
G6PD deficiency — treatment?;Avoid triggers | Supportive care | Transfusion if severe | Folic acid | Splenectomy NOT indicated
Which glycolytic enzyme deficiency causes neurological involvement plus hemolysis?;Triose Phosphate Isomerase (TPI) deficiency — rarest and most lethal
How to differentiate enzyme deficiency hemolytic anemias from AIHA on one test?;Coombs test — NEGATIVE in all enzyme deficiencies | POSITIVE in AIHA
Prevalence order of RBC enzyme deficiencies causing hemolysis?;G6PD > Pyruvate Kinase > G6P Isomerase > others
PK deficiency vs G6PD deficiency — splenectomy useful in which?;PK deficiency — YES (extravascular hemolysis in spleen) | G6PD deficiency — NO
- 9 reticulocyte cards (from your image + extra NEET PG high-yield points)
- 9 PK deficiency cards
- 9 G6PD deficiency cards
- 4 exam trap/comparison cards
- Save as
hemolytic_reticulocyte.txt - Anki → File → Import
- Separator: Semicolon
- Field 1 → Front, Field 2 → Back
- Import → exactly 31 cards
Now don't mix the cuts. Give the reticulocytes separately.
What are reticulocytes?;Non-nucleated red cell precursors | Have blue-red polychromatophilic cytoplasm due to residual ribosomal RNA (mesh-like reticular network)
How are reticulocytes visualized on smear?;Supravital stains — methylene blue or brilliant cresyl blue | Stain the ribosomal RNA | NOT seen on routine Giemsa stain
What is the normal reticulocyte count?;0.5–1.5% of total red cells
What does reticulocytosis indicate?;Effective erythropoiesis — good bone marrow response to anemia | Seen in: Hemolytic anemias | Acute blood loss
What does reticulocytopenia indicate?;Ineffective erythropoiesis — poor bone marrow response | Seen in: Aplastic anemia | Chemotherapy | Bone marrow malignancy | Anemia of chronic disease | Iron deficiency anemia | Vitamin B12/Folate deficiency
Why is reticulocyte count HIGH in hemolytic anemias like PK and G6PD deficiency?;Increased RBC destruction → bone marrow compensates → releases more reticulocytes into circulation (effective erythropoiesis)
What is the corrected reticulocyte count formula and why is it used?;Corrected count = Reticulocyte% × (Patient Hb ÷ 15) | Raw % is falsely high in anemia because fewer total RBCs — correction adjusts for the dilution effect
What is Reticulocyte Production Index (RPI) and its interpretation?;RPI = Corrected reticulocyte count ÷ Maturation factor | RPI >3 = Hemolytic anemia or acute blood loss (hyperproliferative) | RPI <2 = Hypoproliferative anemia (iron deficiency, aplastic, B12/folate deficiency)
What is polychromasia on routine smear and what does it represent?;Blue-tinged RBCs on Giemsa stain = reticulocytes released early from marrow | Indicates stress erythropoiesis or active hemolysis
reticulocytes.txt and import with semicolon as separator — gives exactly 9 cards.