
Screenshot_20260621-123802.png
Explain
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete explanation of all three topics from the image, sourced directly from Robbins, Cotran & Kumar - Pathologic Basis of Disease.
Pancreatic Neuroendocrine Neoplasms (PanNENs)
What are they? PanNENs are tumors arising from the hormone-secreting islet cells of the pancreas (formerly called "islet cell tumors"). They are rare, accounting for only about 2% of all pancreatic neoplasms. They can arise anywhere in the pancreas or adjacent peripancreatic tissue, and may be single or multiple. Some produce hormones and cause distinct clinical syndromes ("functional"), while others are silent ("nonfunctional").
Grading: PanNENs are graded by their proliferative index (Ki-67 marker) and mitotic activity. Poorly differentiated ones (Ki-67 >20%) behave as carcinomas.
Key genetic mutations in sporadic PanNENs:
- MEN1 gene mutations (also seen in familial MEN-1 syndrome)
- PTEN / TSC2 loss-of-function mutations → activate mTOR signaling pathway
- ATRX / DAXX inactivating mutations → allow "alternative lengthening of telomeres" (ALT); nearly half of PanNENs carry one of these
1. Hyperinsulinism (Insulinoma)
The most common PanNEN. These are β-cell tumors that produce excess insulin.
Pathology:
- Usually solitary, small (<2 cm), encapsulated, benign (only ~10% are malignant)
- Located anywhere in the pancreas
- Histologically resemble enlarged islets - monotonous cells in regular cords
- Characteristic finding: amyloid deposition within the tumor (see histology image below)
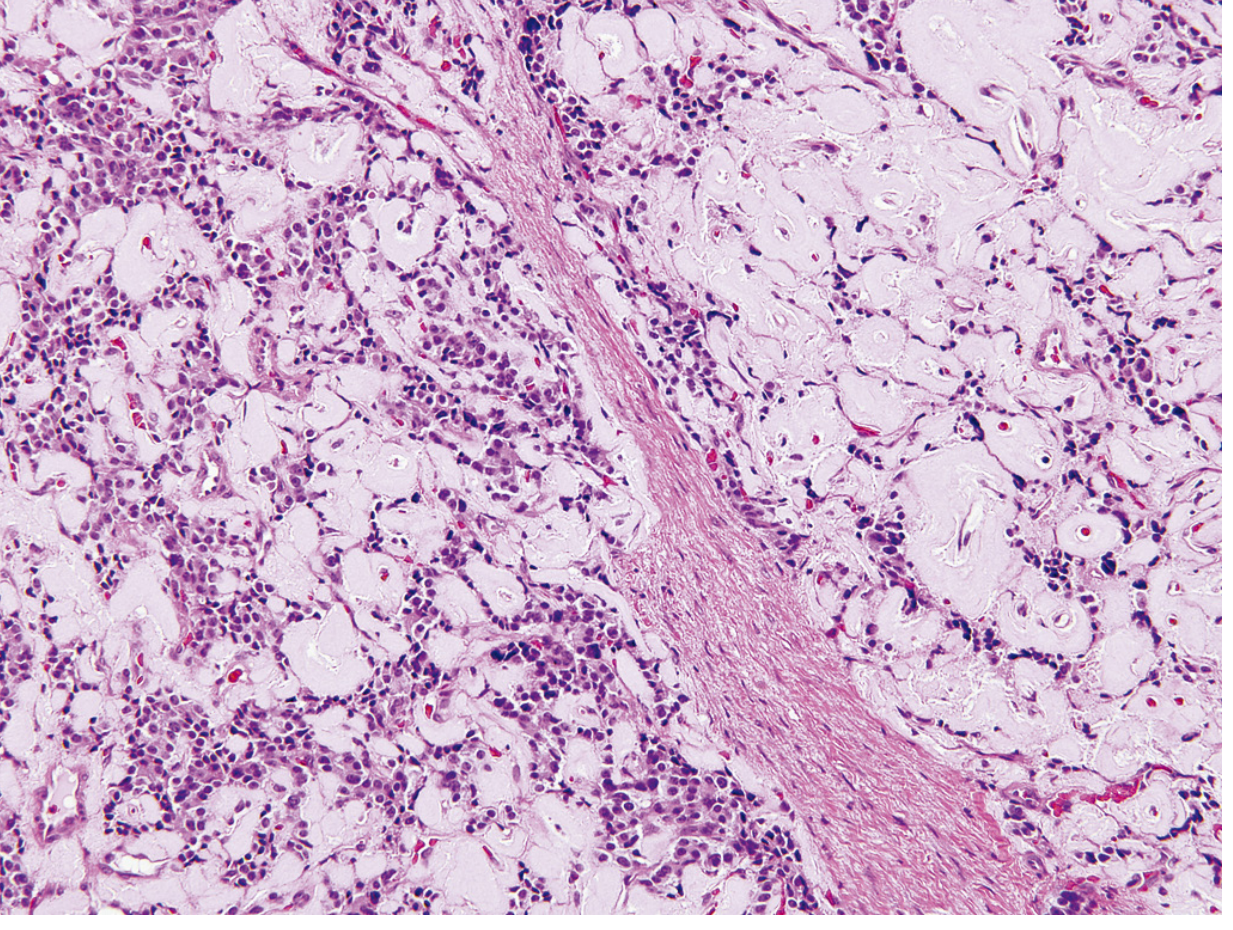
Histology of an insulinoma: monotonous neoplastic islet cells with characteristic pink amyloid deposits. The patient had episodic hypoglycemia.
Clinical features:
- Hypoglycemic episodes when blood glucose falls below 50 mg/dL
- Symptoms: confusion, stupor, loss of consciousness
- Triggered by fasting or exercise; relieved immediately by glucose
- Key lab finding: inappropriately elevated insulin + low blood glucose + elevated C-peptide (confirms endogenous source)
- Treatment: surgical removal - usually curative
Important DDx of hypoglycemia: adrenal insufficiency, liver disease, glycogen storage disorders, ectopic insulin production, sulfonylurea use, factitious insulin injection.
2. Zollinger-Ellison Syndrome (Gastrinoma)
G-cell tumors (gastrinomas) that hypersecrete gastrin, driving excessive gastric acid production.
Location: These arise in the "gastrinoma triangle" - spanning the duodenum, pancreas, and peripancreatic soft tissues. They are as likely to arise in the duodenum as in the pancreas.
Pathology:
- Over 50% are already locally invasive or metastatic at diagnosis (more aggressive than insulinomas)
- ~25% arise as part of MEN-1 syndrome (typically multifocal); sporadic ones are usually single
- Histologically bland, minimal anaplasia
Clinical features (Zollinger-Ellison Syndrome):
- Hypergastrinemia → excess gastric acid → peptic ulceration
- Ulcers are often multiple, recurrent, and in unusual locations (including the jejunum)
- Ulcers are resistant to standard therapy
- Present in 90-95% of patients with gastrinoma
Treatment:
- Suppress acid: H⁺/K⁺-ATPase inhibitors (PPIs)
- Surgical excision of the tumor when possible (curative)
- Hepatic metastases carry a poor prognosis (liver failure typically within 10 years)
3. Other Rare Pancreatic Endocrine Neoplasms
| Tumor | Cell of Origin | Hormone | Clinical Syndrome |
|---|---|---|---|
| Glucagonoma | α-cells | Glucagon | Mild diabetes, necrolytic migratory erythema (skin rash), anemia; mainly in peri/postmenopausal women |
| Somatostatinoma | δ-cells | Somatostatin | Diabetes, gallstones (cholelithiasis), steatorrhea, achlorhydria (hypochlorhydria); hard to localize preoperatively |
| VIPoma | - | VIP (Vasoactive Intestinal Peptide) | WDHA syndrome: Watery Diarrhea, Hypokalemia, Achlorhydria; can metastasize |
| Pancreatic carcinoid | - | Serotonin | Atypical carcinoid syndrome; exceedingly rare |
| PPoma | - | Pancreatic polypeptide | Presents as a mass lesion only (no symptoms even with high hormone levels) |
Some PanNENs are multihormonal, secreting two or more hormones simultaneously (e.g., insulin + glucagon, or ACTH + ADH). These must be distinguished from MEN syndromes, where separate tumors arise in multiple endocrine glands independently.
Summary table:
| Feature | Insulinoma | Gastrinoma | Others |
|---|---|---|---|
| Frequency | Most common PanNEN | 2nd most common | Rare |
| Malignancy rate | ~10% | >50% | Variable |
| Key hormone | Insulin | Gastrin | Glucagon/VIP/somatostatin |
| Key syndrome | Hypoglycemia | Peptic ulcers (ZES) | See table above |
| Treatment | Surgery | PPIs + surgery | Surgery |
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease, pp. 1027-1029
This is a shared conversation. Sign in to Orris to start your own chat.