Hypertension cause kidney damge how what is logic in steps mechanism understand with Fully logic for genius students
hypertension kidney damage pathophysiology mechanism glomerular hemodynamic
hypertensive nephrosclerosis vascular remodeling afferent arteriole RAAS kidney
hypertension kidney damage mechanism diagram glomerulosclerosis
intraglomerular hypertension autoregulation breakdown proteinuria glomerulosclerosis mechanism
hypertensive kidney RAAS angiotensin TGF-beta tubulointerstitial fibrosis CKD progression
How Hypertension Destroys the Kidney: The Full Mechanistic Logic
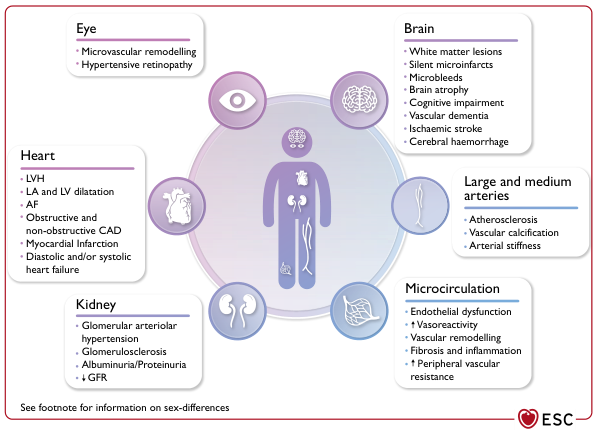
Sources: Harrison's Principles of Internal Medicine, 21st Ed. (pp. 7642, 7647–7648) | ESC Management of Hypertension (p. 18)
The Big Picture First
Phase 1 — The Vascular Wall Takes the First Hit
Resistance ∝ 1 / r⁴
| Response | Mechanism | Net Effect |
|---|---|---|
| Hypertrophic remodeling | Smooth muscle hypertrophy + increased extracellular matrix deposition | Lumen narrows, wall thickens |
| Eutrophic remodeling | Cell rearrangement around a smaller lumen, no volume change | Lumen narrows with same wall mass |
Phase 2 — The Glomerulus Loses Its Pressure Shield (Autoregulation Fails)
- BP rises → afferent arteriole constricts → glomerular capillary pressure stays constant (~50 mmHg)
- BP falls → arteriole dilates → pressure maintained
Systemic high pressure is transmitted directly into the glomerular capillaries — this is called intraglomerular hypertension.
"With progressive renal injury, there is a loss of autoregulation of renal blood flow, resulting in a lower blood pressure threshold for renal damage and a steeper slope between blood pressure and renal damage."
Phase 3 — Glomerular Hyperfiltration and the Protein Leak
3A: Mechanical Stretch → Podocyte Injury
- Fenestrated endothelium
- Glomerular basement membrane (GBM)
- Podocytes (the key pressure-sensing filtration cells with interdigitating foot processes)
- Large proteins (primarily albumin) leak through into the filtrate → proteinuria / albuminuria
3B: Glomerular Hyperperfusion and Hyperfiltration
- Protein is toxic to tubular epithelial cells
- Proximal tubule cells endocytose filtered protein → triggers inflammatory mediator release (NF-κB, MCP-1)
- Tubular inflammation and injury follow
Phase 4 — Ischemic and Fibrotic Destruction of the Tubulointerstitium
4A: Ischemia from Arteriolar Narrowing
"Atherosclerotic, hypertension-related vascular lesions in the kidney primarily affect preglomerular arterioles, resulting in ischemic changes in the glomeruli and postglomerular structures."
4B: RAAS Activation → TGF-β → Fibrosis
Reduced renal perfusion pressure
↓
Juxtaglomerular cells release RENIN
↓
Renin cleaves Angiotensinogen → Angiotensin I
↓
ACE converts → Angiotensin II (Ang II)
↓
Ang II binds AT1 receptors on:
• Systemic vessels → vasoconstriction → BP↑↑
• Efferent arteriole (preferentially) → ↑ intraglomerular pressure
• Mesangial cells → proliferation
• Tubular cells → NaCl retention → volume expansion → BP↑↑
↓
Ang II also stimulates TGF-β (Transforming Growth Factor-beta)
↓
TGF-β activates myofibroblasts in the interstitium
↓
Myofibroblasts deposit collagen → TUBULOINTERSTITIAL FIBROSIS
↓
Nephron loss → permanent GFR decline
Phase 5 — The Vicious Self-Amplifying Cycle (The "Death Spiral")
Hypertension
│
▼
Nephron loss (from all above mechanisms)
│
▼
Remaining nephrons hypertrophy + hyperfiltrate
│
▼
RAAS activated → Na retention → BP rises further
│
▼
Reduced renal mass = less renal vasodilatory prostaglandins
│
▼
BP rises MORE → more nephron loss
│
▼
End-Stage Renal Disease (ESRD)
"The result may be a vicious cycle of renal damage and nephron loss leading to more severe hypertension, glomerular hyperfiltration, and further renal damage."
Special Case: Malignant (Accelerated) Hypertension
- Fibrinoid necrosis of afferent arterioles (plasma proteins leak into and coagulate within the vessel wall, destroying it)
- This extends into the glomerular tuft → focal glomerular necrosis
- The glomerulus is destroyed within days, not years
Integrated Summary Table
| Phase | Location | Mechanism | Consequence |
|---|---|---|---|
| 1 | Afferent arteriole | Hypertrophic/eutrophic remodeling, fibrosis | Lumen narrowing, stiffness |
| 2 | Glomerular capillary | Autoregulation failure → intraglomerular HTN | Capillary hypertension |
| 3 | Glomerular filtration barrier | Podocyte injury, basement membrane stretch | Proteinuria, hyperfiltration |
| 4A | Tubules | Ischemia from arteriolar narrowing | Tubular atrophy |
| 4B | Interstitium | RAAS → Ang II → TGF-β → fibrosis | Collagen deposition, nephron loss |
| 5 | Whole kidney | Nephron loss → more RAAS → more HTN | Vicious cycle → ESRD |
The One-Sentence Master Logic
Chronic high pressure stiffens and narrows the afferent arteriole, breaking the glomerulus's pressure-protection mechanism; high pressure is then transmitted directly into delicate filtration capillaries, destroying podocytes and leaking protein, while ischemia and RAAS-driven fibrosis destroy the tubules and interstitium, and the loss of nephrons elevates BP further — completing a self-accelerating cycle that ends in renal failure.
More logical mechanism and easy wordimg for genius doctor
glomerular autoregulation myogenic response tubuloglomerular feedback afferent efferent arteriole pressure
podocyte injury mechanical stretch oxidative stress endothelial dysfunction hypertension glomerular filtration barrier
angiotensin II efferent arteriole constriction intraglomerular pressure hyperfiltration single nephron GFR
Hypertension → Kidney Damage: Full Mechanistic Logic
Start With One Core Idea
Step 1 — The Kidney Has a Built-In Pressure Shield
Renal artery → Afferent arteriole → [GLOMERULUS] → Efferent arteriole → Peritubular capillaries
| Defense Mechanism | How It Works | Speed |
|---|---|---|
| Myogenic reflex | Afferent arteriole senses stretch from high BP → constricts immediately | Seconds |
| Tubuloglomerular Feedback (TGF) | Macula densa senses increased NaCl delivery → signals afferent to constrict | Minutes |
| Angiotensin II on efferent | Low flow → Ang II preferentially constricts efferent → maintains filtration pressure | Minutes |
Step 2 — Chronic Hypertension Destroys the Shield
- Hypertrophic remodeling: smooth muscle cells hypertrophy, matrix proteins (collagen, fibronectin) are deposited in the wall → wall thickens inward → lumen narrows
- Arteriosclerosis / hyalinosis: plasma proteins leak into the vessel wall → get deposited as hyaline material → wall becomes stiff and glassy
The afferent arteriole stays open. High pressure flows straight through, unfiltered, into the glomerular capillary.
Step 3 — Intraglomerular Hypertension: The Glomerulus Takes the Full Hit
Blood side:
1. Fenestrated endothelium (pores ~100 nm — almost no barrier to proteins)
2. Glomerular Basement Membrane (GBM) — blocks large proteins >100 kDa
3. Podocytes — foot processes with slit diaphragms — the final protein barrier
Filtrate side (Bowman's space)
What happens to the endothelium:
What happens to podocytes — the critical injury:
- Mechanical stretch → foot process effacement (flattening and fusion)
- Effaced foot processes → slit diaphragms disappear
- Without slit diaphragms → albumin and proteins pour into the filtrate → PROTEINURIA
Think of podocytes as the waterproof tiles on a pool floor. Smash enough tiles and the water (protein) leaks through permanently.
Step 4 — Proteinuria Starts a Second Fire in the Tubules
Filtered protein in tubular lumen
↓
Proximal tubule cells endocytose it (megalin/cubilin receptors)
↓
Protein overload inside tubular cells
↓
Lysosomal rupture → NF-κB activation
↓
Tubular cells release: MCP-1, RANTES, TNF-α, IL-8
↓
Inflammatory cell infiltration (monocytes, T-cells) into interstitium
↓
Interstitial inflammation → fibroblast activation
↓
TGF-β released → myofibroblasts deposit COLLAGEN
↓
TUBULOINTERSTITIAL FIBROSIS
Step 5 — Ischemia Attacks from the Other Side
Afferent arteriole narrowing
↓
Reduced peritubular capillary flow
↓
Tubular cell ischemia
↓
ATP depletion → tubular cell apoptosis/necrosis
↓
Tubular atrophy → GFR loss
Step 6 — RAAS Activation: The Kidney Makes Everything Worse
Ischemic kidney → JGA releases RENIN
↓
Renin cleaves Angiotensinogen → Angiotensin I
↓
Lung ACE converts → Angiotensin II
↓
Ang II acts on:
SYSTEMIC vessels → vasoconstriction → systemic BP rises
↓ (back to damaging the kidney again)
EFFERENT arteriole → constricts preferentially
↓
Raises intraglomerular pressure FURTHER
↓ (accelerates podocyte and GBM injury)
Adrenal gland → releases ALDOSTERONE
↓
Kidney retains Na and water → blood volume rises → BP rises
↓ (further systemic hypertension)
Mesangial cells → proliferate, produce matrix
↓ (glomerulosclerosis)
Fibroblasts → TGF-β stimulation → more fibrosis
↓ (accelerates interstitial scarring)
Step 7 — The Death Spiral (Nephron Loss Loop)
Nephrons are lost (from all above mechanisms)
↓
Surviving nephrons must hypertrophy and hyperfiltrate
to maintain total GFR
↓
Hyperfiltration = more mechanical stress on podocytes
↓
More podocyte loss → more proteinuria → more fibrosis
↓
More nephron loss → smaller kidney mass
↓
Less kidney mass = less ability to excrete sodium
↓
Na retention → more volume → more BP
↓
Higher BP → more glomerular damage
↓
Even more nephron loss → loop restarts, faster
The Malignant Hypertension Exception
- Fibrinoid necrosis: the vessel wall is so overwhelmed that plasma proteins leak into the wall itself, coagulate there, and destroy the vessel from within
- Looks like "pink smudgy glass" on histology (fibrin + necrotic muscle)
- Extends into the glomerular tuft → focal necrotizing glomerulonephritis
- Kidney failure in days, not years
The Master Logic: One Clean Diagram
SYSTEMIC HYPERTENSION
│
▼
Afferent arteriole wall: remodeling + stiffening
│
▼
Autoregulation fails → intraglomerular pressure rises
│
├──────────────────────────┐
▼ ▼
Podocyte injury Peritubular ischemia
(foot process effacement) (tubular cell death)
│ │
▼ ▼
Proteinuria Tubular atrophy
│
▼
Tubular protein toxicity → Inflammation → Fibrosis
│
▼
NEPHRON LOSS → GFR falls
│
▼
RAAS activation → BP rises + more glomerular pressure
│
▼
More nephron loss → more RAAS → more BP
[VICIOUS CYCLE — self-amplifying]
│
▼
END-STAGE RENAL DISEASE (ESRD)
Why ACE Inhibitors / ARBs Are the Logical Treatment
| Drug Action | Mechanism Interrupted |
|---|---|
| Blocks Ang II formation / receptor | No efferent constriction → intraglomerular pressure drops |
| Reduces systemic BP | Less pressure transmitted to glomerulus |
| Reduces TGF-β stimulation | Less fibrosis |
| Reduces aldosterone | Less Na retention → less volume → less BP |
| Reduces proteinuria directly | Less podocyte stress → slower destruction |