Give the clinical relations of anterior and posterior triangle for all
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have all the information needed from Gray's Anatomy for Students. Here is the complete, well-structured answer on clinical relations of the anterior and posterior triangles of the neck.
Clinical Relations of the Anterior and Posterior Triangles of the Neck
Source: Gray's Anatomy for Students
Anatomical Overview
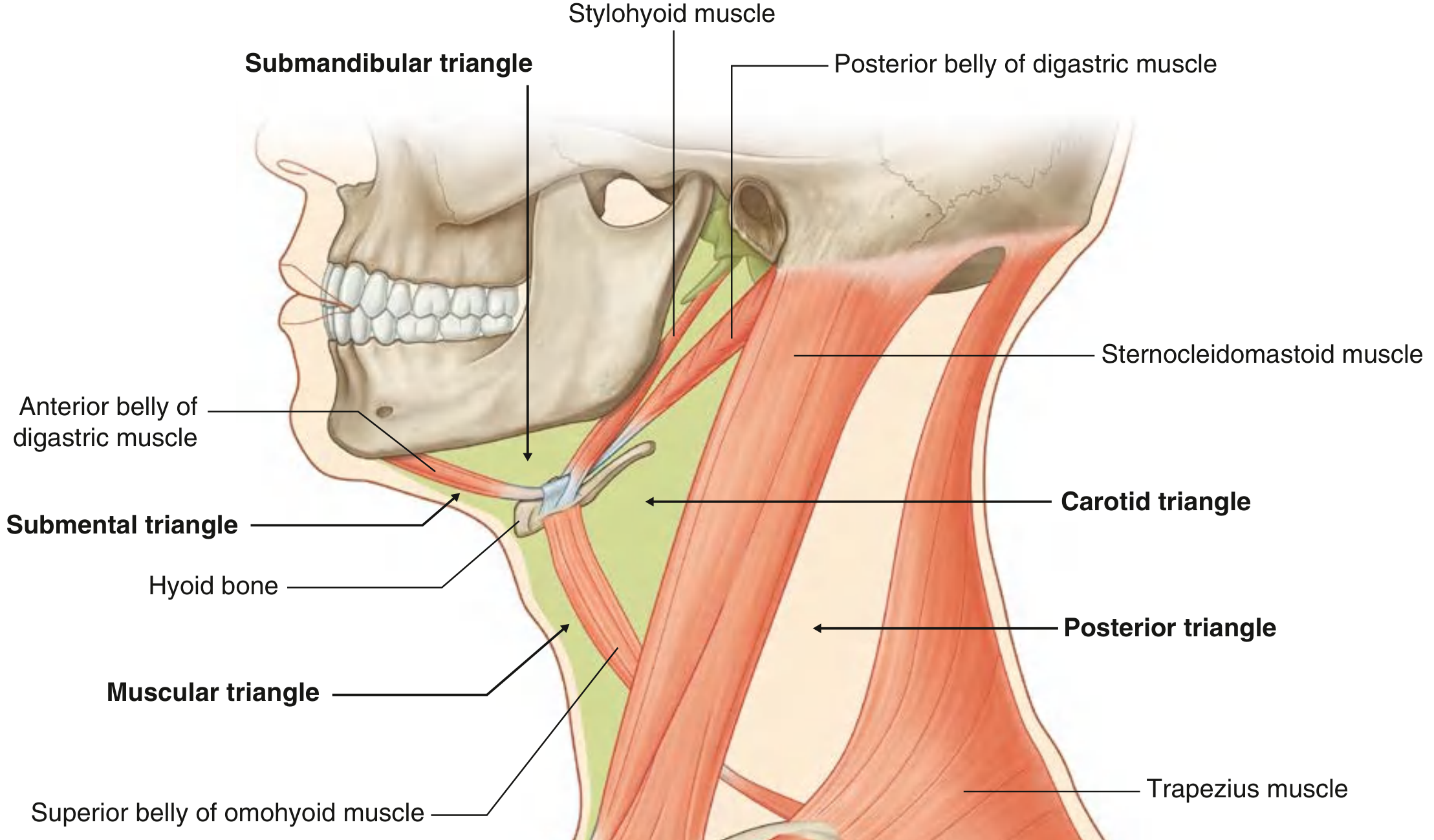
ANTERIOR TRIANGLE OF THE NECK
Borders:
- Lateral: Anterior border of sternocleidomastoid muscle
- Superior: Inferior border of mandible
- Medial: Midline of the neck
The anterior triangle is divided into four sub-triangles, each with distinct clinical significance.
1. Submental Triangle (Unpaired)
Boundaries: Mandibular symphysis (superior), anterior bellies of digastric (laterally), body of hyoid (inferior)
Contents: Submental lymph nodes; tributaries forming the anterior jugular vein
Clinical Relations:
- Submental lymph nodes drain the tip of the tongue, floor of the mouth, lower incisors, and midline lower lip. Enlargement here raises suspicion for:
- Infection of the lower anterior teeth or tip of tongue
- Metastatic spread from carcinoma of the lip, floor of mouth, or tip of tongue
- Submental abscess presents as midline swelling here; may track deep to form Ludwig's angina (a potentially life-threatening cellulitis of the floor of the mouth)
- Dermoid cysts and thyroglossal duct cysts may present as midline swellings in this region
2. Submandibular Triangle (Paired)
Boundaries: Lower border of mandible (superior), anterior belly of digastric (anteroinferiorly), posterior belly of digastric (posteroinferiorly)
Contents: Submandibular gland; submandibular lymph nodes; hypoglossal nerve [XII]; mylohyoid nerve; facial artery and vein
Clinical Relations:
- Submandibular salivary gland enlargement - most common cause of a lump in this triangle; causes include:
- Calculus (stone) obstructing Wharton's duct - presents with painful swelling at mealtimes (obstruction to salivary flow)
- Submandibular sialadenitis (infection)
- Pleomorphic adenoma or carcinoma
- Submandibular lymphadenopathy - enlarged nodes here are commonly associated with infections or malignancy of the:
- Tongue, teeth, gums, lips, cheek, floor of mouth, and anterior nasal cavity
- Level I nodes in neck dissection classification
- Hypoglossal nerve [XII] crosses through this triangle. Injury during submandibular gland excision causes ipsilateral tongue deviation and wasting
- Facial artery and vein loop through this triangle; the facial artery is palpable as it crosses the inferior border of the mandible just anterior to the masseter - a useful pulse point in clinical examination
- Ludwig's angina - spreading cellulitis of the submandibular and submental spaces, a surgical emergency with risk of airway compromise
3. Carotid Triangle (Paired)
Boundaries: Posterior belly of digastric + stylohyoid (superior), superior belly of omohyoid (anteroinferiorly), anterior border of SCM (posteriorly)
Contents: Common carotid artery; internal and external carotid arteries and their branches (superior thyroid, ascending pharyngeal, lingual, facial, occipital arteries); internal jugular vein; vagus nerve [X], accessory nerve [XI], hypoglossal nerve [XII]; superior and inferior roots of ansa cervicalis; transverse cervical nerve; common facial vein tributaries; cervical branch of facial nerve [VII]
Clinical Relations:
- Carotid bifurcation lies within this triangle (at the level of C4 / upper border of thyroid cartilage). This is clinically important for:
- Carotid endarterectomy - surgical access to remove atherosclerotic plaque from the carotid bifurcation; through an incision along the anterior border of SCM
- Carotid artery aneurysm/pseudoaneurysm - pulsatile swelling in this triangle
- Carotid body tumour (chemodectoma/paraganglioma) - benign tumour at the bifurcation; presents as a slowly growing, pulsatile swelling that is mobile side-to-side but NOT up-and-down; gives a positive "lyre sign" on angiography
- Carotid sinus (at bifurcation) - baroreceptors here respond to pressure; hypersensitivity causes syncope (carotid sinus syndrome). Firm palpation during examination can cause bradycardia and hypotension
- Carotid sheath runs through this triangle, containing the common and internal carotid artery, internal jugular vein, and vagus nerve. Deep cervical abscesses can spread along this sheath
- Internal jugular vein is used for:
- Central venous catheter insertion - the junction of the internal jugular vein and subclavian vein (at the inferior limit of this region) is a common site for central line placement
- Venepuncture and cannulation in critically ill patients
- Vagus nerve [X] injury (rare, during surgery): causes hoarseness (recurrent laryngeal nerve) and autonomic dysfunction
- Hypoglossal nerve [XII] loops down and forward through the carotid triangle; at risk during carotid endarterectomy - injury causes ipsilateral tongue deviation
- Lymph nodes in the carotid triangle (deep cervical chain - Level II/III) receive drainage from many head and neck structures; enlargement may indicate:
- Primary or secondary malignancy (metastatic squamous cell carcinoma of the pharynx, larynx, or thyroid)
- Lymphoma
- Tuberculosis (scrofula) - painless enlargement, may develop a collar-stud abscess through the investing fascia
4. Muscular Triangle (Paired)
Boundaries: Midline of neck (medially), superior belly of omohyoid (laterally), anterior border of SCM (posterolaterally), hyoid bone (superiorly)
Contents: Infrahyoid (strap) muscles - sternohyoid, omohyoid, sternothyroid, thyrohyoid; thyroid and parathyroid glands; trachea; pharynx/oesophagus
Clinical Relations:
- Thyroid gland is the dominant structure. Swellings in this triangle suggest:
- Goitre (diffuse enlargement) - moves with swallowing (key diagnostic sign, as it is attached to the larynx and trachea by pretracheal fascia)
- Thyroid nodules - single cold nodule needs investigation to exclude malignancy
- Thyroid carcinoma - papillary (most common), follicular, medullary, anaplastic
- Parathyroid glands sit on the posterior surface of the thyroid. Surgically important during thyroidectomy - inadvertent removal causes hypoparathyroidism and hypocalcaemia
- Tracheotomy / tracheostomy - surgical access to the trachea is through the midline of this triangle, below the thyroid isthmus (usually between rings 2-4)
- Thyroglossal duct cyst - midline swelling between foramen caecum and isthmus; moves upward on tongue protrusion (distinguishing feature). Sistrunk operation is the surgical treatment
- Surgical approach to the larynx and trachea - the infrahyoid muscles are retracted to access the thyroid, larynx, trachea, and parathyroids
POSTERIOR TRIANGLE OF THE NECK
Borders:
- Anteriorly: Posterior edge of sternocleidomastoid
- Posteriorly: Anterior edge of trapezius
- Base: Middle one-third of the clavicle
- Apex: Meeting of SCM and trapezius at the superior nuchal line / occiput
The inferior belly of the omohyoid crosses the triangle, dividing it into:
- Occipital triangle (larger, superior)
- Omoclavicular (subclavian) triangle (smaller, inferior)
Clinical Relations of the Posterior Triangle
A. Accessory Nerve [XI]
- The accessory nerve [XI] exits the jugular foramen, pierces or passes deep to SCM (which it innervates), then crosses the posterior triangle in a superficial plane within the investing layer of cervical fascia, before entering the trapezius (which it also innervates)
- It is the most superficially located nerve in the posterior triangle
- Clinical significance:
- Highly vulnerable to injury during lymph node biopsy, block dissection, or other surgical procedures in the posterior triangle
- Injury produces dropped shoulder (trapezius paralysis), winging of scapula, inability to abduct the arm above 90°, and pain
- Injury to SCM component causes loss of head rotation to the opposite side
- Must be identified and protected in radical / modified radical neck dissection for cervical lymph node metastases
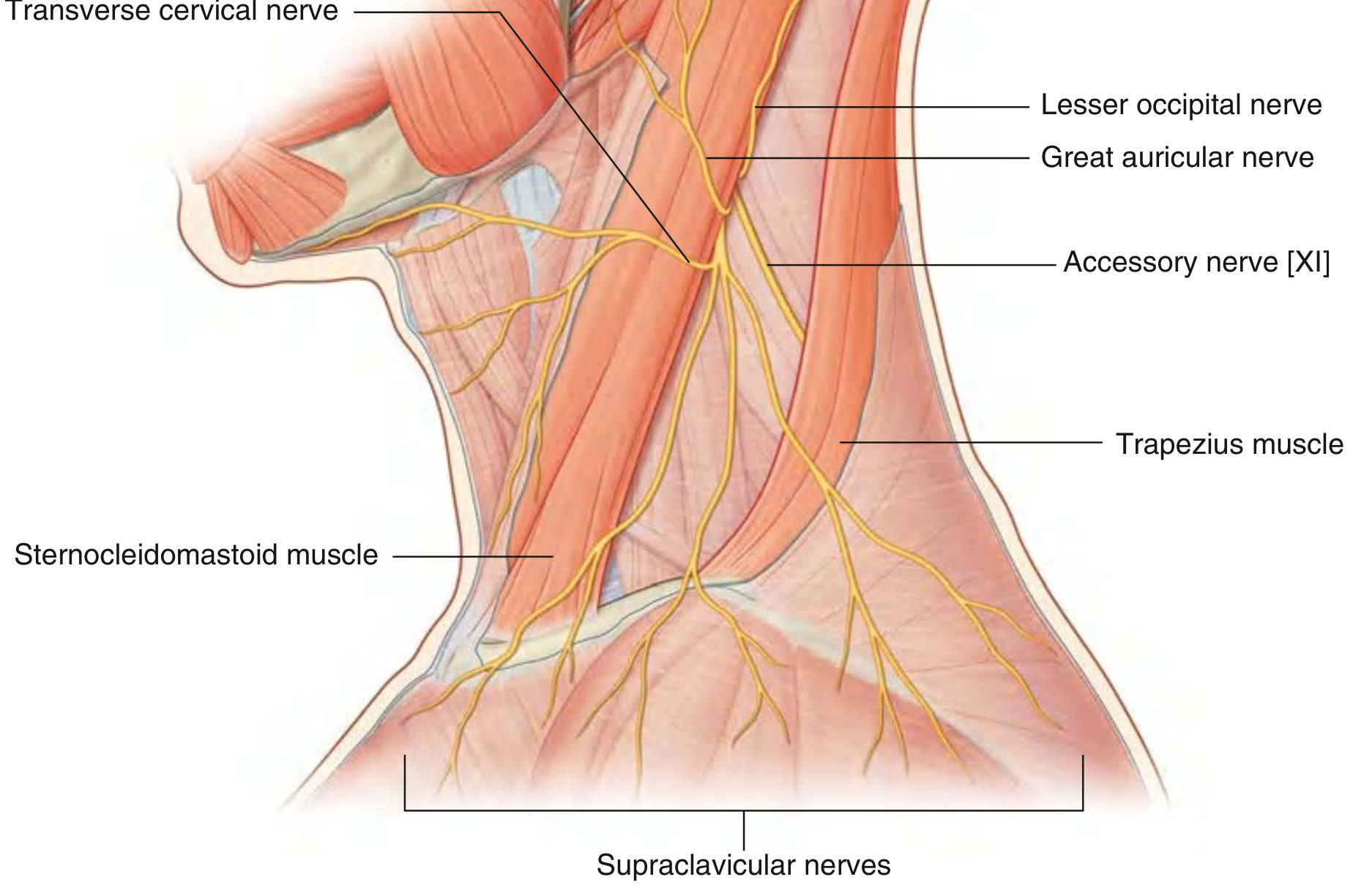
B. Cervical Plexus (Cutaneous branches)
- The cutaneous branches emerge at the posterior border of SCM (Erb's point / nerve point of the neck) at approximately the junction of the upper and lower halves of the posterior border
- Four main cutaneous branches:
- Lesser occipital nerve (C2) - supplies scalp posterior to the ear
- Great auricular nerve (C2, C3) - supplies skin over parotid and lower ear
- Transverse cervical nerve (C2, C3) - supplies anterior neck
- Supraclavicular nerves (C3, C4) - supply lower neck, shoulder, and upper chest
- Clinical significance:
- Cervical plexus block - local anaesthetic injected at Erb's point (posterior border of SCM at its midpoint) to block all four cutaneous branches; used for superficial neck surgeries
- Meralgia paraesthetica analogy - "burning" dysaesthesia in the neck, ear, or shoulder may result from compression of these nerves by swollen lymph nodes, tumours, or direct trauma
- Greater auricular nerve can be harvested as a nerve graft (e.g., for facial nerve repair)
C. Phrenic Nerve
- The phrenic nerve (C3, C4, C5) forms from muscular branches of the cervical plexus and descends on the anterior surface of the anterior scalene muscle within the prevertebral fascia
- Clinical significance:
- Malignancy or enlarged lymph nodes in the posterior triangle (e.g., from lung, breast, or lymphoma) can compress the phrenic nerve, causing ipsilateral diaphragm paralysis (seen as elevated hemidiaphragm on chest X-ray)
- Scalene node biopsy (Daniels procedure) - fat pad anterior to the anterior scalene at the base of the posterior triangle is sampled in staging of lung cancer; the phrenic nerve must be protected
- Cervical rib or thoracic outlet syndrome - abnormal ribs or fascial bands at the base of the posterior triangle can compress the phrenic nerve, subclavian artery, or brachial plexus
D. Brachial Plexus
- The trunks of the brachial plexus emerge between the anterior and middle scalene muscles and pass through the inferior part of the posterior triangle (omoclavicular/subclavian triangle) before entering the axilla
- Clinical significance:
- Thoracic outlet syndrome - compression of brachial plexus (and subclavian artery or vein) as it crosses rib I; causes pain, paraesthesia, and weakness in the upper limb
- Cervical rib - additional rib from C7 compresses lower trunk of brachial plexus (C8, T1); produces wasting of small muscles of the hand, loss of sensation along the medial forearm
- Brachial plexus injuries during difficult deliveries or trauma
- Scalene block - supraclavicular or interscalene nerve block is performed in this region for upper limb anaesthesia
E. External Jugular Vein
- One of the most superficial structures in the posterior triangle; descends vertically after crossing the SCM
- Clinical significance:
- Venous cannulation for fluid resuscitation or drug administration when other access is difficult
- Visible distension in raised jugular venous pressure (JVP) - an important clinical sign of right heart failure, cardiac tamponade, or superior vena cava obstruction
- Air embolism risk if the vein is cut during neck surgery (as it is under negative pressure in the neck)
F. Subclavian Artery
- The third part of the subclavian artery (after crossing anterior scalene) runs through the omoclavicular triangle at the base of the posterior triangle
- Clinical significance:
- Subclavian artery aneurysm - pulsatile swelling at the base of the posterior triangle, may cause thoracic outlet syndrome
- Pulse palpation - the subclavian artery can be pressed against rib I to compress and feel the pulse
- Subclavian steal syndrome - stenosis proximal to the vertebral artery origin causes reversed flow in the vertebral artery, leading to vertebrobasilar ischaemia on upper limb exercise; can be detected by blood pressure difference between arms
G. Lymph Nodes (Level V - Posterior Triangle Group)
- Nodes of the posterior triangle (Level Va - spinal accessory chain; Level Vb - transverse cervical chain) receive lymphatics from the occipital scalp, posterior neck, and nasopharynx
- Clinical significance:
- Lymph node metastases from nasopharyngeal carcinoma, thyroid carcinoma, or occipital scalp melanoma frequently involve the posterior triangle
- Lymphoma - one of the most common malignancies presenting as posterior triangle lymphadenopathy, especially in young adults
- Tuberculosis - scrofula (TB lymphadenitis) is a classic cause of persistent posterior triangle node enlargement; may develop a collar-stud abscess (extends through the investing fascia)
- Nerve point block for diagnostic block or pain management
- Posterior triangle nodes are included in Level V neck dissection for head and neck cancers
Summary Table
| Triangle | Key Clinical Conditions |
|---|---|
| Submental | Midline cyst (thyroglossal/dermoid), submental node metastases (floor of mouth/lip cancers), Ludwig's angina |
| Submandibular | Submandibular calculus/sialadenitis, salivary gland tumour, Level I metastatic nodes, hypoglossal nerve injury |
| Carotid | Carotid endarterectomy, carotid body tumour, IJV central line insertion, deep cervical abscess, lymphoma, TB (collar-stud abscess) |
| Muscular | Thyroid/parathyroid disease, goitre, thyroglossal cyst, tracheostomy, laryngeal access |
| Posterior | Accessory nerve injury (shoulder drop), cervical plexus block (Erb's point), brachial plexus/thoracic outlet syndrome, cervical rib, phrenic nerve compression, IJV distension, Level V lymphadenopathy (NPC, lymphoma, TB) |
- Gray's Anatomy for Students, pp. 1145-1167
Give about perineal pouches in unddrstandable manner with diagrams for gold medal
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a gold-medal quality answer. Let me compose it.
Perineal Pouches - Complete Gold Medal Notes
Source: Gray's Anatomy for Students + Campbell-Walsh Urology
First, Understand the Framework
Think of the perineum like a sandwich. From below upward, the layers are:
PELVIC CAVITY (above)
│
│ ← Levator ani (pelvic floor / "ceiling" of perineum)
│
├──────────────────────────────────────────────
│ DEEP PERINEAL POUCH ← thin space ABOVE the perineal membrane
├── PERINEAL MEMBRANE (thick fibrous sheet) ──
│ SUPERFICIAL PERINEAL POUCH ← space BELOW the perineal membrane
├──────────────────────────────────────────────
│
│ ← Colles fascia (membranous layer of superficial fascia)
│
SKIN
The perineal membrane is the KEY structure that creates these two pouches. Everything makes sense once you visualize this.
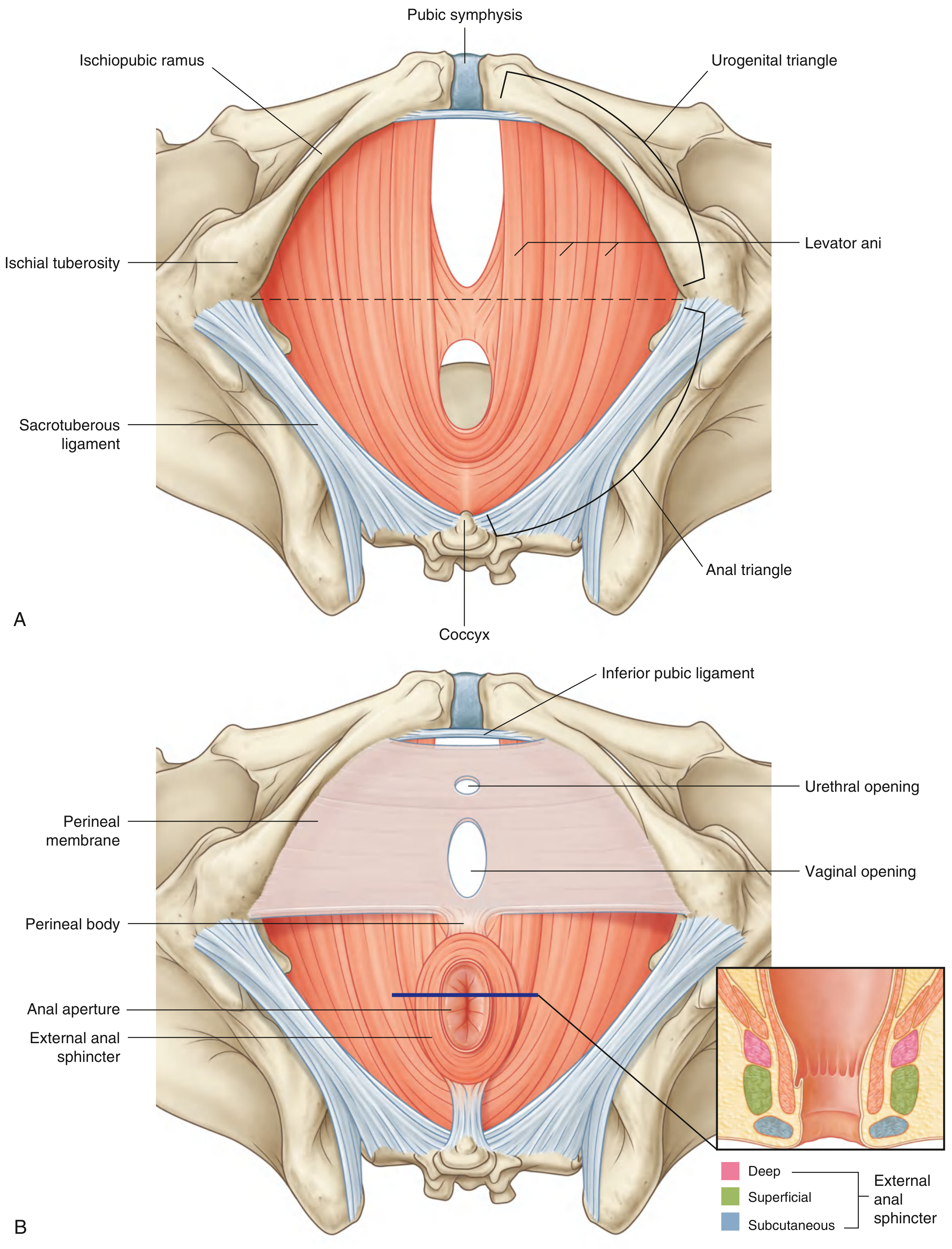
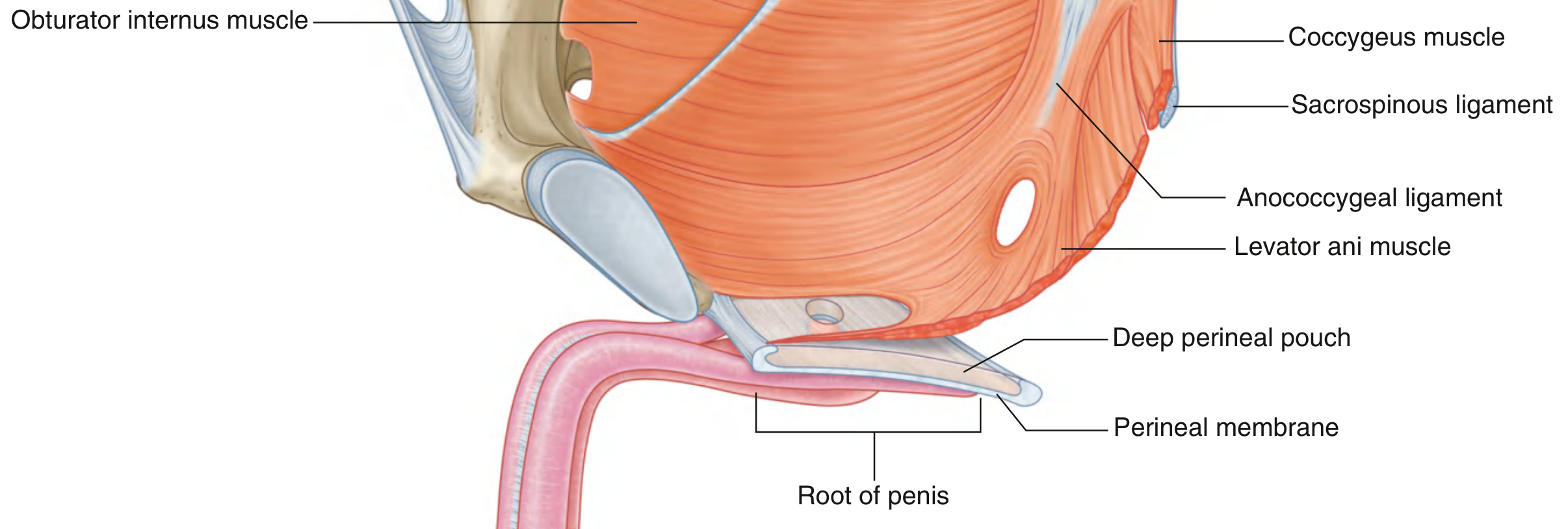
The Perineal Membrane - The Dividing Structure
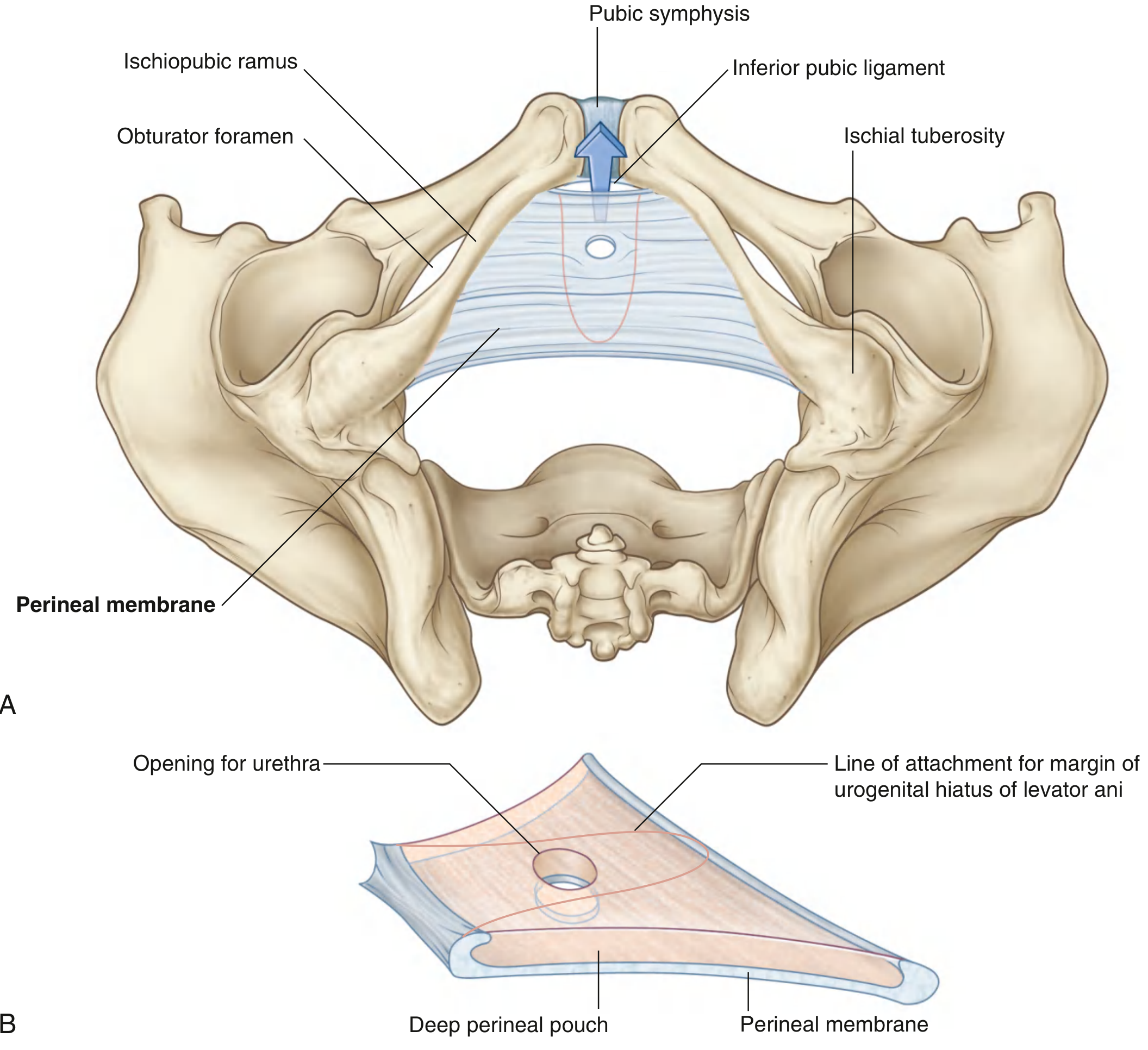
- A thick, fibrous, triangular sheet that fills the urogenital triangle
- Attached laterally to the ischiopubic rami on each side (like a hammock)
- Has a free posterior border, anchored in the midline to the perineal body
- Has two openings: one for the urethra (and vagina in women, just posterior to the urethra)
- The deep dorsal vein of the penis/clitoris passes through a gap between the arcuate pubic ligament and the anterior margin of the membrane (important clinically!)
POUCH 1: Deep Perineal Pouch
Location
Immediately superior (above) the perineal membrane, and inferior (below) the levator ani. It is open superiorly - there is NO distinct fascial layer separating it from the pelvic cavity above. This is clinically very important.
Contents (same in both sexes)
| Structure | Notes |
|---|---|
| External urethral sphincter | Most important muscle here; surrounds the membranous urethra; innervated by pudendal nerve (S2-S4); voluntarily relaxes during micturition |
| Deep transverse perineal muscle | Runs transversely, attaches to perineal body; stabilizes the perineal body |
| Neurovascular structures | Branches of internal pudendal vessels + pudendal nerve |
Contents - Additional in Women Only
| Structure | Notes |
|---|---|
| Compressor urethrae | Runs from ischiopubic ramus, blends with partner anterior to urethra; accessory sphincter |
| Sphincter urethrovaginalis | From perineal body, passes forward lateral to vagina, blends anterior to urethra |
Contents - Additional in Men Only
| Structure | Notes |
|---|---|
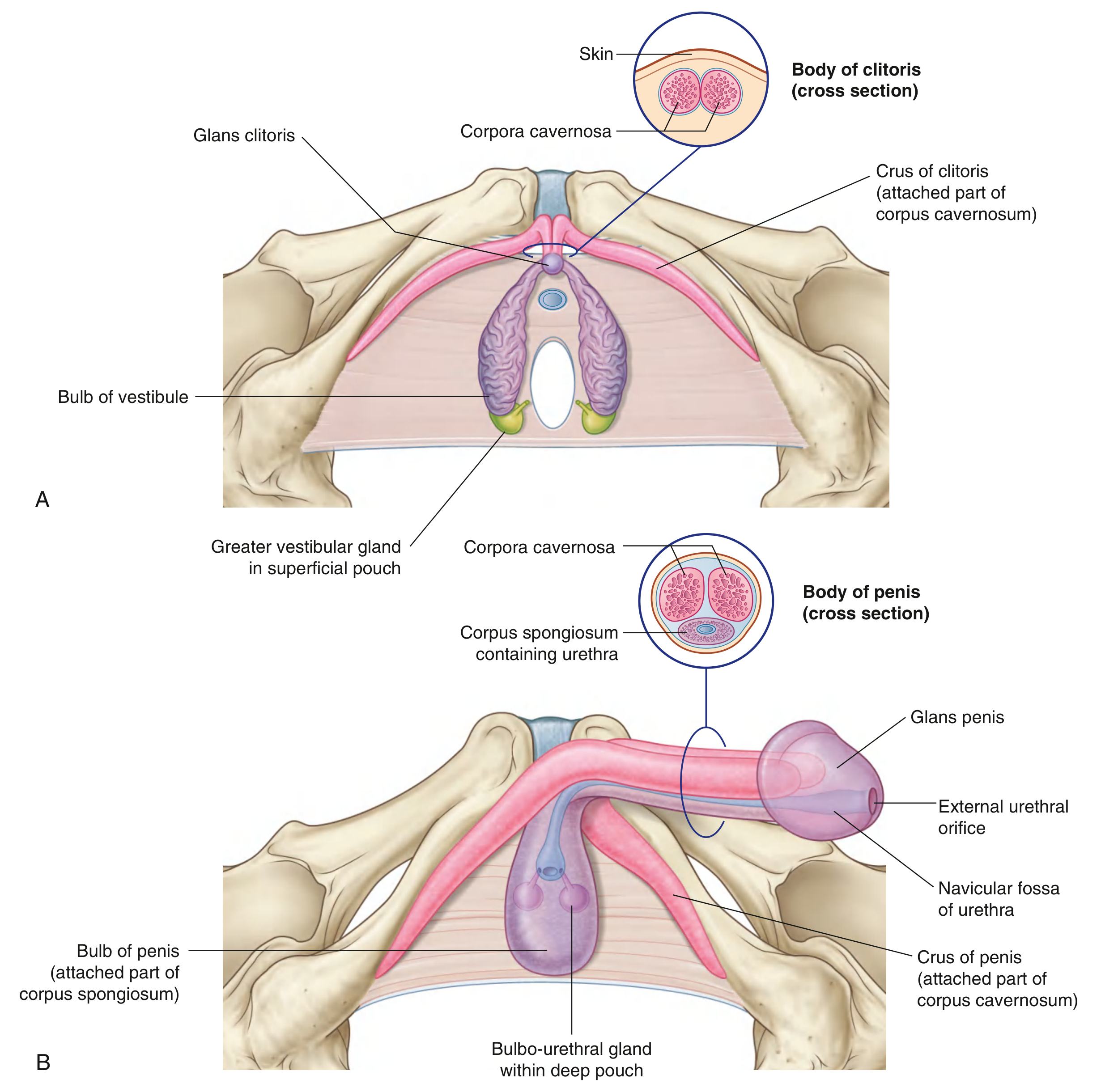
| Bulbo-urethral (Cowper's) glands | Paired glands in the deep pouch; their long ducts (about 3 cm) pierce the perineal membrane and open into the bulbous urethra in the superficial pouch. They secrete mucus for lubrication before ejaculation |
Functions of the Deep Pouch
- Supports external genitalia - perineal membrane and deep pouch together provide a strong platform for attachment of the erectile tissue roots below
- Supports pelvic viscera - because it is open above and covered by the urogenital hiatus of levator ani, it forms part of the pelvic floor
- Voluntary urinary control - through the external urethral sphincter
Clinical Relations of Deep Perineal Pouch
- Urethral injury above the perineal membrane - because the deep pouch is open above, extravasated urine or blood can track upward into the extraperitoneal space of the pelvis
- Cowper's gland abscess - presents as perineal swelling; duct stricture can cause obstruction
- Nerve damage during radical prostatectomy - pudendal nerve branches in the deep pouch may be injured, causing stress urinary incontinence (urethral sphincter damage)
POUCH 2: Superficial Perineal Pouch
Location
Below (inferior to) the perineal membrane, and above Colles fascia (the membranous layer of superficial perineal fascia). It is a closed space (this is the most important clinical point).
Boundaries (Think: "Closed Box")
| Wall | Structure |
|---|---|
| Roof (superior) | Perineal membrane (inferior fascia of urogenital diaphragm) |
| Floor (inferior) | Colles fascia (membranous layer of superficial perineal fascia) |
| Lateral walls | Ischiopubic rami |
| Posterior | Posterior border of perineal membrane fused to perineal body; Colles fascia sweeps backward and fuses here → CLOSED posteriorly |
| Anterior | OPEN anteriorly - continuous with the loose connective tissue beneath Scarpa's fascia on the anterior abdominal wall |
Contents in BOTH Sexes
| Structure | Notes |
|---|---|
| Roots (crura) of the corpora cavernosa | Attached to ischiopubic rami; covered by ischiocavernosus muscles |
| Ischiocavernosus muscles | Cover the crura; compress venous outflow during erection, maintaining rigidity |
| Superficial transverse perineal muscles | Anchor perineal body; innervated by pudendal nerve |
| Perineal body | Central fibromuscular node where many muscles converge |
| Branches of pudendal nerve and internal pudendal vessels | Sensory and motor supply to perineal structures |
Contents - In MEN
| Structure | Notes |
|---|---|
| Bulb of penis (attached part of corpus spongiosum) | Fixed to perineal membrane; bulbospongiosus muscle covers it |
| Bulbospongiosus muscle | Covers the bulb; compresses urethra during micturition (expels last drops) and ejaculation (pulsatile expulsion of semen) |
Contents - In WOMEN
| Structure | Notes |
|---|---|
| Bulbs of the vestibule | Paired erectile structures flanking the vaginal opening; equivalent to corpus spongiosum in men; attached to perineal membrane |
| Bulbospongiosus muscle | Covers each vestibular bulb; compresses it during sexual arousal, directs blood to glans clitoris |
| Greater vestibular glands (Bartholin's glands) | Located at the posterior ends of the vestibular bulbs; open via ducts at the 4 and 8 o'clock positions of the vaginal orifice; secrete mucus for lubrication |
Clinical Relations of Superficial Perineal Pouch - THE GOLD MEDAL PART
The superficial pouch is a CLOSED BOX, open only anteriorly. This governs how fluid (blood/urine) spreads when the pouch is breached.
1. Extravasation of Urine (Rupture of Spongy/Bulbar Urethra)
- The bulbar urethra is the most commonly injured part (straddle injury / fall astride)
- Urine or blood escapes into the superficial perineal pouch
- Because the pouch is closed posteriorly (at the perineal body) and laterally (attached to ischiopubic rami), and open anteriorly, fluid tracks in a predictable direction:
Extravasated urine / blood:
↓
CANNOT go posteriorly (blocked by perineal body)
CANNOT go to thighs (Colles fascia fuses with fascia lata)
↓
Goes ANTERIORLY into:
1. Scrotum / Labia majora (dartos fascia - gives "bag of nuts" swelling)
2. Penis / clitoris (Buck's fascia connects)
3. Anterior abdominal wall under Scarpa's fascia
↓
STOPS at clavicles (Scarpa's ends here)
STOPS at fascia lata laterally
This is the classic "butterfly bruise" / "butterfly hematoma" pattern on the perineum after straddle injury, extending up the scrotum and anterior abdominal wall.
2. Bartholin's Gland Cyst/Abscess (Women)
- Duct blockage → Bartholin's cyst; if infected → Bartholin's abscess
- Presents as a tender unilateral labial swelling at the posterior introitus
- Treatment: incision and drainage or marsupialization
3. Perineal Hematoma after Childbirth
- Injury to the vestibular bulbs (highly vascular) during vaginal delivery
- Blood collects in the superficial pouch, causing a painful vulval hematoma
4. Ischiocavernosus Injury / Priapism
- Damage to the ischiocavernosus muscle or its nerve supply affects venous drainage of the corpora, contributing to priapism or post-traumatic erectile dysfunction
5. Episiotomy
- Surgical incision of the perineum during delivery cuts through the superficial pouch, perineal body, and bulbospongiosus
- Mediolateral episiotomy avoids the Bartholin's gland duct and central perineal body
Summary Comparison Table
| Feature | Superficial Perineal Pouch | Deep Perineal Pouch |
|---|---|---|
| Location | Below perineal membrane | Above perineal membrane |
| Roof | Perineal membrane | Levator ani / open to pelvis |
| Floor | Colles fascia | Perineal membrane |
| Open/Closed | Closed posteriorly, open anteriorly | Open superiorly into pelvis |
| Main muscles | Ischiocavernosus, bulbospongiosus, superficial transverse perineal | External urethral sphincter, deep transverse perineal |
| Key gland (male) | - | Cowper's (bulbo-urethral) glands |
| Key gland (female) | Bartholin's (greater vestibular) glands | - |
| Erectile tissue | Roots of corpora cavernosa + bulb of penis/vestibular bulbs | - |
| Urethra | Spongy (penile) urethra enclosed in corpus spongiosum | Membranous urethra surrounded by external sphincter |
| Clinical disaster | Urethral rupture → "butterfly" extravasation | Pelvic extravasation; stress incontinence |
Quick Memory Hook
"SDP": Superficial = Scrotal swelling; Deep = external sphinCter + Cowper's"
Or for the pouch walls:
Superficial pouch = Colles below, Perineal membrane above Deep pouch = Perineal membrane below, open pelvis above
Sources: Gray's Anatomy for Students, pp. 580-587; Campbell-Walsh Urology 3-Volume Set, Ch. 82
Give a explanation and easy gold medal explanation on sulci and gyri
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have everything needed. Let me compile the complete gold medal answer.
Sulci and Gyri - Gold Medal Explanation
Sources: Localization in Clinical Neurology 8e, Neuroanatomy through Clinical Cases 3rd Ed, Neuroscience: Exploring the Brain 5th Ed
The Absolute Basics First
Think of the brain like a walnut or a crumpled newspaper.
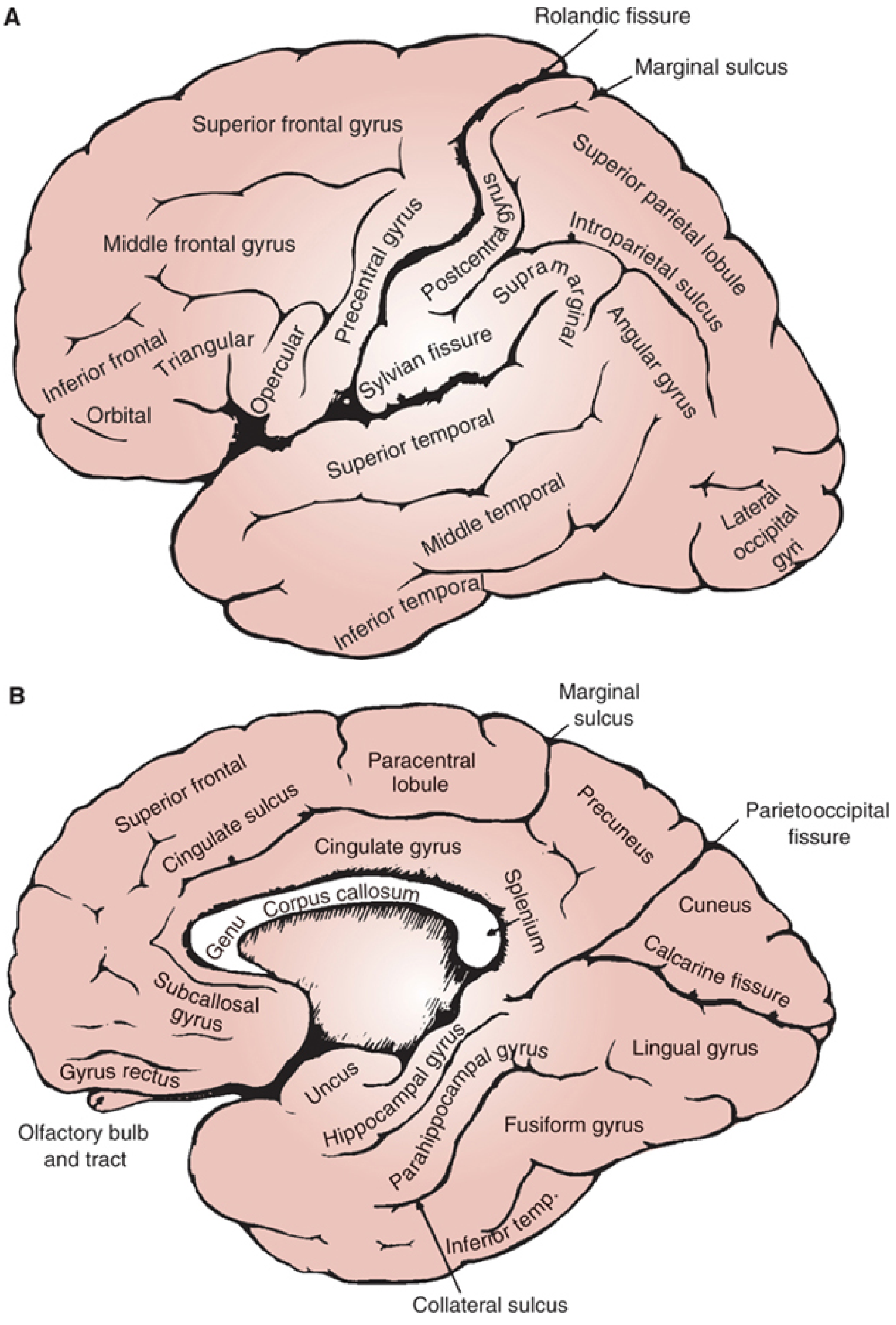
- Gyrus (plural: gyri) = the ridges/bumps you see on the brain surface (from Greek gyros = circle/fold)
- Sulcus (plural: sulci) = the grooves/valleys between the ridges (from Latin sulcus = furrow/ditch)
- Fissure = a very deep sulcus - these are the big landmarks (e.g. Sylvian fissure, longitudinal fissure)
Why does the brain have folds at all?
The cerebral cortex (the outer grey matter) needs a huge surface area to pack billions of neurons. The human skull is a fixed size. The brain solved this by folding - exactly like crumpling an A1 sheet of paper to fit into a wallet. Without folding, the cortex would need a head 3-4x larger.
Key fact: About 2/3 of the cortical surface is hidden inside sulci - only 1/3 is visible on the surface.
The Big Picture - Lobes and Their Boundaries
The brain is divided into 4 main lobes on each hemisphere by key sulci/fissures:
The Two Major Landmark Sulci (Learn These First)
| Sulcus | Other Names | What It Separates |
|---|---|---|
| Central sulcus | Rolandic fissure, Sulcus of Rolando | Frontal lobe (front) from Parietal lobe (back) |
| Lateral sulcus | Sylvian fissure | Frontal + Parietal (above) from Temporal lobe (below) |
Plus on the medial surface:
- Parietooccipital sulcus - separates Parietal from Occipital lobe
LOBE BY LOBE BREAKDOWN WITH GYRI AND SULCI
🧠 FRONTAL LOBE
Location: Anterior to the central sulcus, above the Sylvian fissure
Key Sulci:
- Central sulcus (Rolandic fissure) - the most important sulcus; its posterior bank is the primary motor cortex
- Precentral sulcus - just anterior to the central sulcus; separates precentral gyrus from the frontal gyri
- Superior frontal sulcus - divides superior from middle frontal gyri
- Inferior frontal sulcus - divides middle from inferior frontal gyri
- Cingulate sulcus (medial surface) - separates cingulate gyrus from the medial frontal cortex
Key Gyri and Their Functions:
| Gyrus | Location | Function |
|---|---|---|
| Precentral gyrus | Immediately anterior to central sulcus | Primary MOTOR cortex (Brodmann area 4) - controls movement of OPPOSITE body side |
| Superior frontal gyrus | Topmost strip of frontal lobe | Executive function, working memory |
| Middle frontal gyrus | Middle strip | Executive function, eye movement control (frontal eye field - area 8) |
| Inferior frontal gyrus | Lowest strip; has 3 parts: orbital, triangular (pars triangularis), opercular (pars opercularis) | Broca's area (areas 44, 45) in LEFT hemisphere = speech production/language formulation |
| Paracentral lobule (medial) | Medial surface around central sulcus | Motor and sensory for the LOWER LIMB and genitals |
| Cingulate gyrus (medial) | Arches over corpus callosum | Emotion, motivation, pain processing (part of limbic system) |
| Gyrus rectus (inferior/orbital) | Medial to olfactory tract | Olfaction, higher order integration |
Memory hook for frontal gyri:
"Surgeons Make Incisions" = Superior, Middle, Inferior frontal gyri (top to bottom)
🧠 PARIETAL LOBE
Location: Behind the central sulcus, above the Sylvian fissure, anterior to the occipital lobe
Key Sulci:
- Postcentral sulcus - separates postcentral gyrus from the rest of parietal lobe
- Intraparietal sulcus - divides superior from inferior parietal lobule
- Sylvian fissure (inferiorly) - the floor of parietal lobe borders the temporal lobe
Key Gyri and Their Functions:
| Gyrus | Location | Function |
|---|---|---|
| Postcentral gyrus | Immediately posterior to central sulcus | Primary SOMATOSENSORY cortex (areas 3, 1, 2) - receives touch, pain, temp, proprioception from OPPOSITE body |
| Superior parietal lobule | Above intraparietal sulcus | Spatial perception, visuospatial processing, skilled movements |
| Supramarginal gyrus | Inferior parietal lobule - curves around END of Sylvian fissure | Part of language circuit; lesion → conduction aphasia, ideomotor apraxia |
| Angular gyrus | Inferior parietal lobule - curves around END of superior temporal sulcus | Reading, writing, calculation (Gerstmann syndrome if damaged: agraphia + acalculia + finger agnosia + left-right disorientation) |
🧠 TEMPORAL LOBE
Location: Below the Sylvian fissure, anterior to occipital lobe
Key Sulci:
- Superior temporal sulcus - divides superior from middle temporal gyri
- Inferior temporal sulcus - divides middle from inferior temporal gyri
- Collateral sulcus (inferior surface) - separates parahippocampal gyrus from fusiform gyrus
- Hippocampal sulcus - separates hippocampal gyrus from parahippocampal gyrus
Key Gyri and Their Functions:
| Gyrus | Location | Function |
|---|---|---|
| Superior temporal gyrus (STG) | Top strip of temporal lobe | Wernicke's area (area 22, posterior part of STG) in LEFT hemisphere = language comprehension |
| Transverse temporal gyri (Heschl's gyri) | On the superior bank of Sylvian fissure, hidden | Primary AUDITORY cortex (areas 41, 42); LEFT Heschl > RIGHT in right-handed people |
| Middle temporal gyrus | Middle strip | Semantic memory, word recognition |
| Inferior temporal gyrus | Lowest strip | Visual object recognition, face recognition |
| Parahippocampal gyrus | Inferomedial temporal lobe | Memory encoding/recall; part of Papez circuit |
| Uncus | Anterior hook of parahippocampal gyrus | Contains amygdala; primary olfactory cortex - uncal herniation compresses CN III (blown pupil) |
| Fusiform (occipitotemporal) gyrus | Inferior temporal surface | Face recognition (fusiform face area); prosopagnosia if damaged |
🧠 OCCIPITAL LOBE
Location: Most posterior; behind the parietooccipital sulcus (medial)
Key Sulci:
- Calcarine sulcus (fissure) - the KEY sulcus of the occipital lobe; runs horizontally on medial surface
- Parietooccipital sulcus - separates occipital from parietal lobe (medial)
- Lunate sulcus - anterior boundary of primary visual cortex (lateral surface)
Key Gyri and Their Functions:
| Gyrus | Location | Function |
|---|---|---|
| Cuneus | Medial occipital, ABOVE calcarine sulcus | Upper visual field representation (primary visual cortex, area 17) |
| Lingual gyrus | Medial occipital, BELOW calcarine sulcus | Lower visual field representation (area 17); colour processing |
| Lateral occipital gyri | Lateral surface | Visual association cortex (areas 18, 19) - object recognition |
Memory hook for visual cortex:
Calcarine sulcus = Camera line - the screen where vision is "projected" Upper bank (cuneus) = lower visual field; Lower bank (lingual) = upper visual field (remember: everything is crossed)
THE MOST IMPORTANT SULCI - MASTER LIST
| Sulcus/Fissure | What it Separates | Why You Must Know It |
|---|---|---|
| Central sulcus (Rolando) | Frontal / Parietal | Motor cortex (pre) vs Sensory cortex (post) |
| Lateral sulcus (Sylvian) | Frontal+Parietal / Temporal | Broca vs Wernicke, insula hidden inside |
| Parietooccipital sulcus | Parietal / Occipital | On medial surface only |
| Calcarine sulcus | Cuneus / Lingual gyrus | Primary visual cortex on its banks |
| Cingulate sulcus | Cingulate gyrus / Medial frontal | Limbic system boundary |
| Intraparietal sulcus | Superior / Inferior parietal lobule | Spatial attention |
| Collateral sulcus | Parahippocampal / Fusiform | Temporal lobe base |
THE MOTOR AND SENSORY HOMUNCULUS
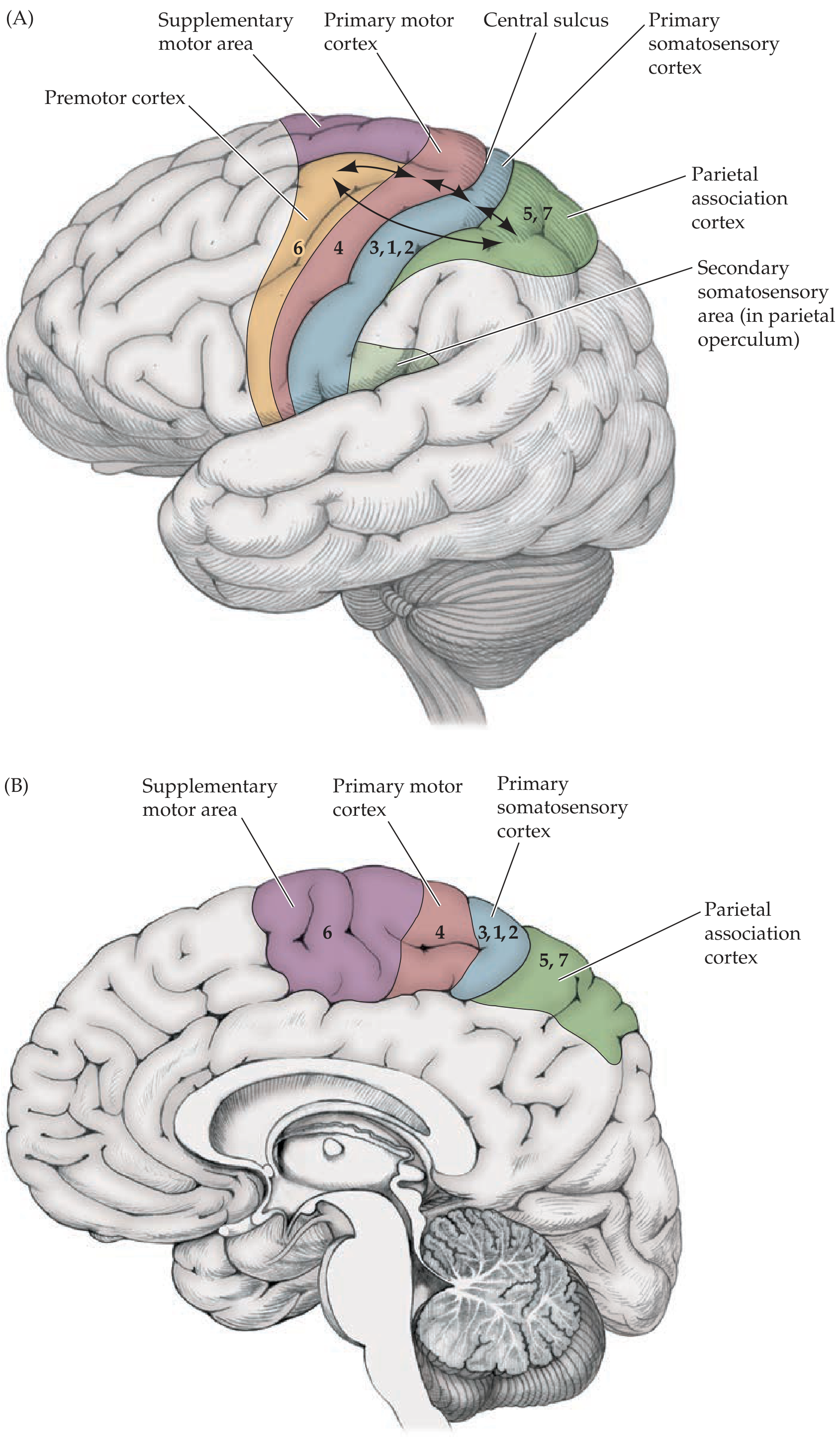
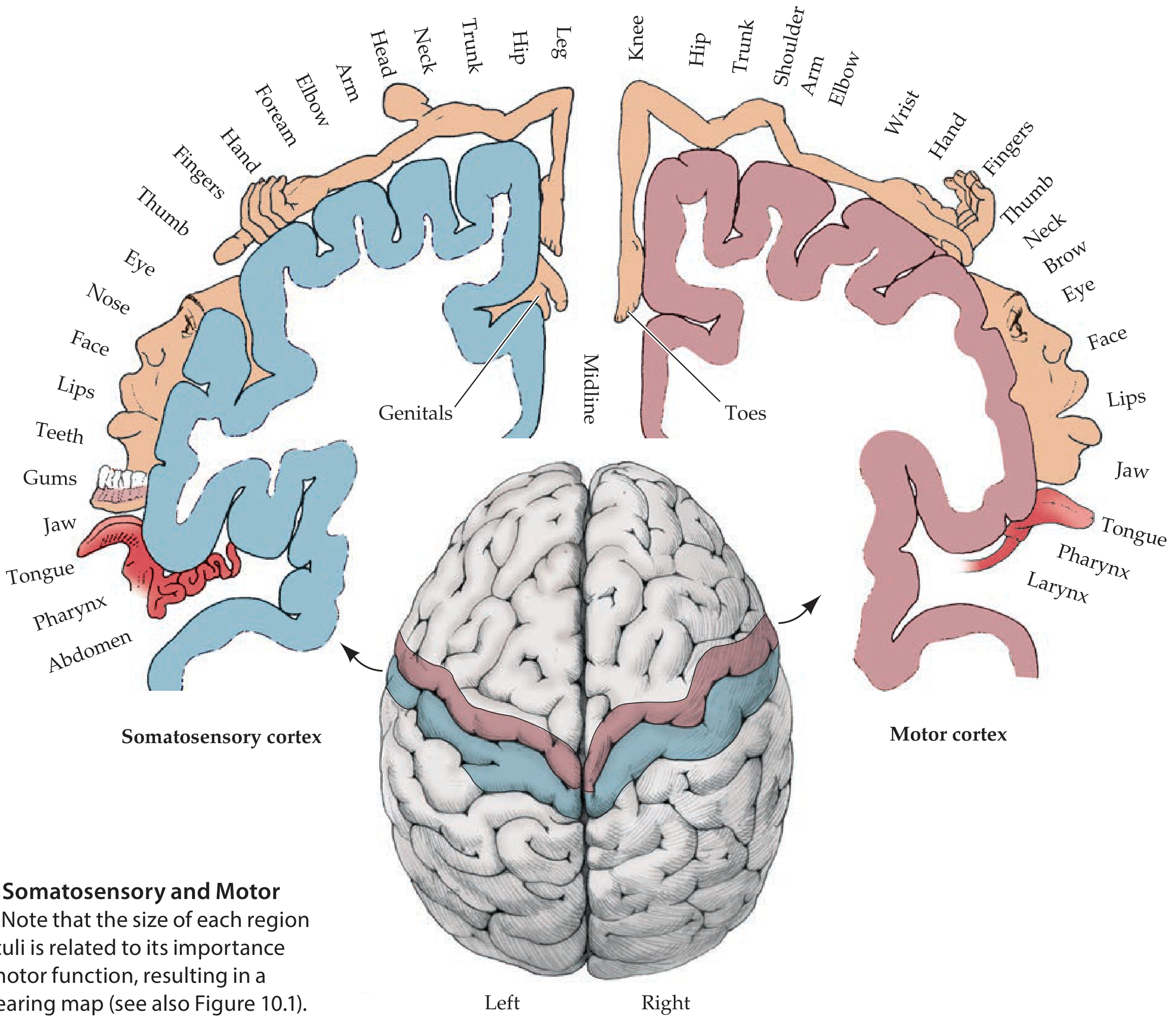
The homunculus ("little man") is the map of the body on the precentral (motor) and postcentral (sensory) gyri:
- Motor homunculus = on the precentral gyrus (area 4)
- Sensory homunculus = on the postcentral gyrus (areas 3, 1, 2)
- Body is upside down: legs and genitals on the medial surface (paracentral lobule); face, lips, tongue at the bottom near Sylvian fissure
- Disproportionate representation - more cortex = more fine control/sensitivity; so hands and face have the most cortex, while trunk has very little
- Both are contralateral - left hemisphere controls/receives from RIGHT body, and vice versa
CLINICALLY IMPORTANT GYRI - WHAT BREAKS WHEN YOU DAMAGE THEM
| Gyrus Damaged | Clinical Result |
|---|---|
| Precentral gyrus (primary motor, area 4) | Contralateral hemiplegia/hemiparesis; UMN signs |
| Postcentral gyrus (primary sensory, areas 3,1,2) | Contralateral hemisensory loss (touch, proprioception, 2-point discrimination) |
| Inferior frontal gyrus - LEFT (Broca's area 44, 45) | Broca's aphasia - non-fluent speech, good comprehension, poor repetition; "knows what to say but can't say it" |
| Superior temporal gyrus - LEFT (Wernicke's area 22) | Wernicke's aphasia - fluent but meaningless speech (paraphasias), POOR comprehension; "can't understand what's said" |
| Angular gyrus - LEFT | Gerstmann syndrome (agraphia + acalculia + finger agnosia + left-right disorientation); also alexia |
| Supramarginal gyrus - LEFT | Conduction aphasia (poor repetition, but fluent speech and good comprehension); ideomotor apraxia |
| Fusiform gyrus | Prosopagnosia - can't recognize faces |
| Parahippocampal + Hippocampal gyrus | Amnesia - especially new memory formation (anterograde amnesia) |
| Uncus | Uncal herniation - compresses CN III → blown (dilated, fixed) pupil; "down and out" eye |
| Calcarine cortex (occipital) | Contralateral homonymous hemianopia (with macular sparing because macula has dual blood supply) |
| Paracentral lobule (medial, legs area) | Leg weakness + bladder/bowel dysfunction (important in parasagittal meningioma, falx meningioma) |
| Cingulate gyrus (bilateral) | Akinetic mutism (patient awake but doesn't move or speak) |
BROCA'S AREA vs WERNICKE'S AREA - Easy Memory
FRONT of brain → FRONTAL lobe → Broca's area → FORMULATES speech
(area 44, 45 = inferior frontal gyrus)
Lesion = can't SPEAK fluently
Comprehension is GOOD (they understand you)
BACK of brain → TEMPORAL lobe → Wernicke's area → hears and UNDERSTANDS
(area 22 = posterior superior temporal gyrus)
Lesion = can't UNDERSTAND
Speech is fluent but makes NO SENSE (word salad)
Simple memory trick:
- Broca = Broken speech (non-fluent, telegraphic)
- Wernicke = Wordy but wrong (fluent but incomprehensible)
INSULA (Island of Reil) - The Hidden Gyrus
The insula is buried deep within the Sylvian fissure. It is covered by the frontal, parietal, and temporal opercula (lids). It is only visible when you pull the lips of the Sylvian fissure apart.
Functions:
- Pain processing
- Autonomic function (cardiac, visceral)
- Taste cortex (primary gustatory cortex)
- Interoception (awareness of internal body state)
- Involved in language (especially in stroke)
Clinical: Insular infarction (middle cerebral artery territory) can cause cardiac arrhythmias (autonomic dysfunction) and significantly worsen stroke outcome.
MEDIAL SURFACE GYRI - The Ones Exams Love
| Gyrus/Structure | Location | Function |
|---|---|---|
| Cingulate gyrus | Arches over corpus callosum | Emotion, attention, pain, motivation (limbic system) |
| Paracentral lobule | Medial continuation of pre- and postcentral gyri | Leg motor and sensory + bladder/bowel control |
| Precuneus | Between marginal sulcus and parietooccipital sulcus | Self-referential processing, visuo-spatial imagery, consciousness |
| Cuneus | Above calcarine sulcus in occipital lobe | Upper visual field |
| Lingual gyrus | Below calcarine sulcus | Lower visual field + colour perception |
| Parahippocampal gyrus | Medial temporal | Memory gateway; contains entorhinal cortex |
| Subcallosal gyrus | Just below genu of corpus callosum | Part of limbic circuit |
QUICK REVISION SUMMARY TABLE
| Lobe | Separated By | Key Gyrus | Key Function |
|---|---|---|---|
| Frontal | Central sulcus (posteriorly), Sylvian (inferiorly) | Precentral gyrus | Primary motor cortex; Broca's area (IFG left) |
| Parietal | Central sulcus (anteriorly) | Postcentral gyrus | Primary somatosensory; Angular gyrus (reading/writing) |
| Temporal | Sylvian fissure (superiorly) | Superior temporal gyrus | Wernicke's area; primary auditory (Heschl) |
| Occipital | Parietooccipital sulcus (medially) | Calcarine banks (cuneus + lingual) | Primary visual cortex |
THE GOLD MEDAL MEMORY SYSTEM
Step 1 - Learn the 2 big dividers:
Central sulcus divides motor (front) from sensory (back) Sylvian fissure divides the temporal lobe from the rest
Step 2 - Each lobe has 3 gyri in a row (Superior, Middle, Inferior):
Frontal: Superior, Middle, Inferior frontal gyri Temporal: Superior, Middle, Inferior temporal gyri
Step 3 - Learn the "border zones" - the special gyri:
Precentral = motor | Postcentral = sensory (these straddle the central sulcus) Supramarginal + Angular = inferior parietal lobule (language connections) Heschl = primary hearing (buried in Sylvian fissure) Calcarine banks = primary vision
Step 4 - Clinical localization:
Front of brain = doing things (motor, speech output) Back of brain = knowing things (sensory, language comprehension, vision) Medial surface = leg + bladder + emotion + memory
Sources: Localization in Clinical Neurology 8e, p. 1182-1186; Neuroanatomy through Clinical Cases 3rd Ed, pp. 248-250
Give a explanation and easy remembering way axially artery and brachial artery and radial artery course and gold medal answer
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Triangle tiopio
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.