17-year-old woman who recently began taking birth control pills presents to the emergency room with cramping abdominal pain, anxiety, paranoia, and hallucinations. A surgical evaluation, including ultrasound and computed tomography scan, fails to demonstrate an acute abdominal process. An urinalysis reveals an increase in urine ALA and PBG. What is your probable diagnosis? Which enzyme deficiency leads to this condition? Explain in detail the metabolic pathway that is defective in this patient What is the biochemical basis of the clinical features? Give reasons for the development of symptoms after taking birth control pills
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Acute Intermittent Porphyria (AIP)
1. Probable Diagnosis
Acute Intermittent Porphyria (AIP)
The clinical triad of:
- Cramping abdominal pain with a normal abdominal exam and negative surgical workup
- Neuropsychiatric features (anxiety, paranoia, hallucinations)
- Elevated urinary ALA (delta-aminolevulinic acid) and PBG (porphobilinogen)
...is the classic presentation of AIP. The disorder is "one of the great mimics in clinical medicine, with manifestations ranging from acute abdominal pain to psychosis." The onset in a post-pubertal young woman who recently started a hormonal drug is entirely characteristic.
2. Enzyme Deficiency
The deficient enzyme is Porphobilinogen (PBG) deaminase - also called Hydroxymethylbilane synthase (HMBS).
All patients with AIP carry approximately a 50% reduction in PBG deaminase enzymatic activity, consistent with the autosomal dominant inheritance of the condition. Under normal baseline conditions, this halved activity is sufficient - symptoms only appear when the demand for heme synthesis increases and the residual enzyme is overwhelmed.
3. The Heme Biosynthetic Pathway and Where It Goes Wrong
Here is the full heme biosynthetic pathway, with the AIP defect shown:
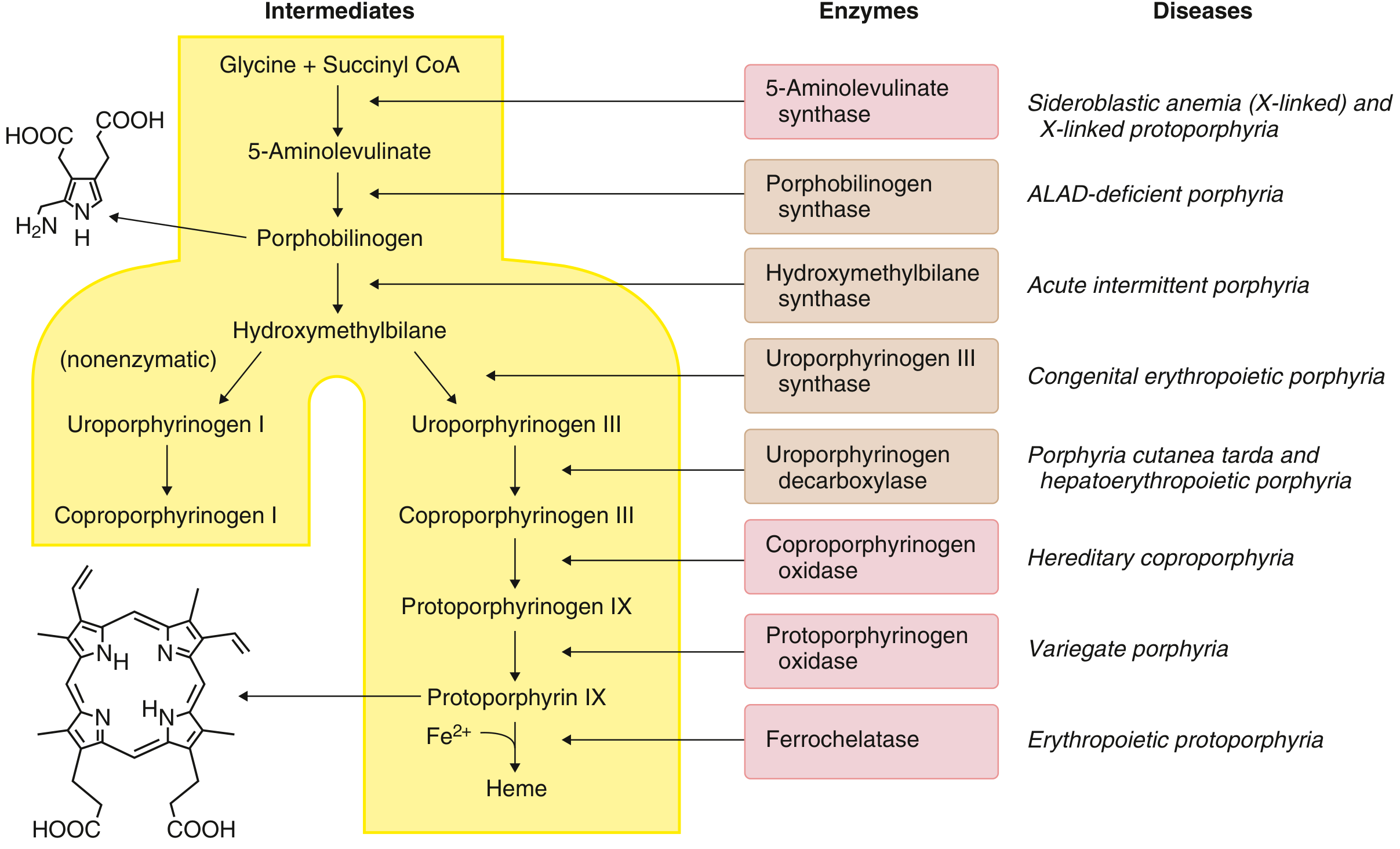
Step-by-step pathway:
| Step | Location | Substrate | Enzyme | Product |
|---|---|---|---|---|
| S1 | Mitochondria | Glycine + Succinyl-CoA | ALA synthase (ALAS1) | 5-Aminolevulinate (ALA) |
| S2 | Cytosol | 2x ALA | ALA dehydratase (PBG synthase) | Porphobilinogen (PBG) |
| S3 | Cytosol | 4x PBG | PBG deaminase / Hydroxymethylbilane synthase ← DEFICIENT in AIP | Hydroxymethylbilane |
| S4 | Cytosol | Hydroxymethylbilane | Uroporphyrinogen III synthase | Uroporphyrinogen III |
| S5 | Cytosol | Uroporphyrinogen III | Uroporphyrinogen decarboxylase (UROD) | Coproporphyrinogen III |
| S6 | Mitochondria | Coproporphyrinogen III | Coproporphyrinogen oxidase (CPOX) | Protoporphyrinogen IX |
| S7 | Mitochondria | Protoporphyrinogen IX | Protoporphyrinogen oxidase (PPOX) | Protoporphyrin IX |
| S8 | Mitochondria | Protoporphyrin IX + Fe²⁺ | Ferrochelatase (FECH) | Heme |
Note: Heme synthesis starts and ends in the mitochondrion, with the middle steps occurring in the cytosol. Approximately 90% of heme synthesis occurs in erythroid precursors (for hemoglobin), while the remainder occurs in the liver, largely for incorporation into cytochrome P450 (CYP) enzymes.
The pathogenic mechanism in AIP:
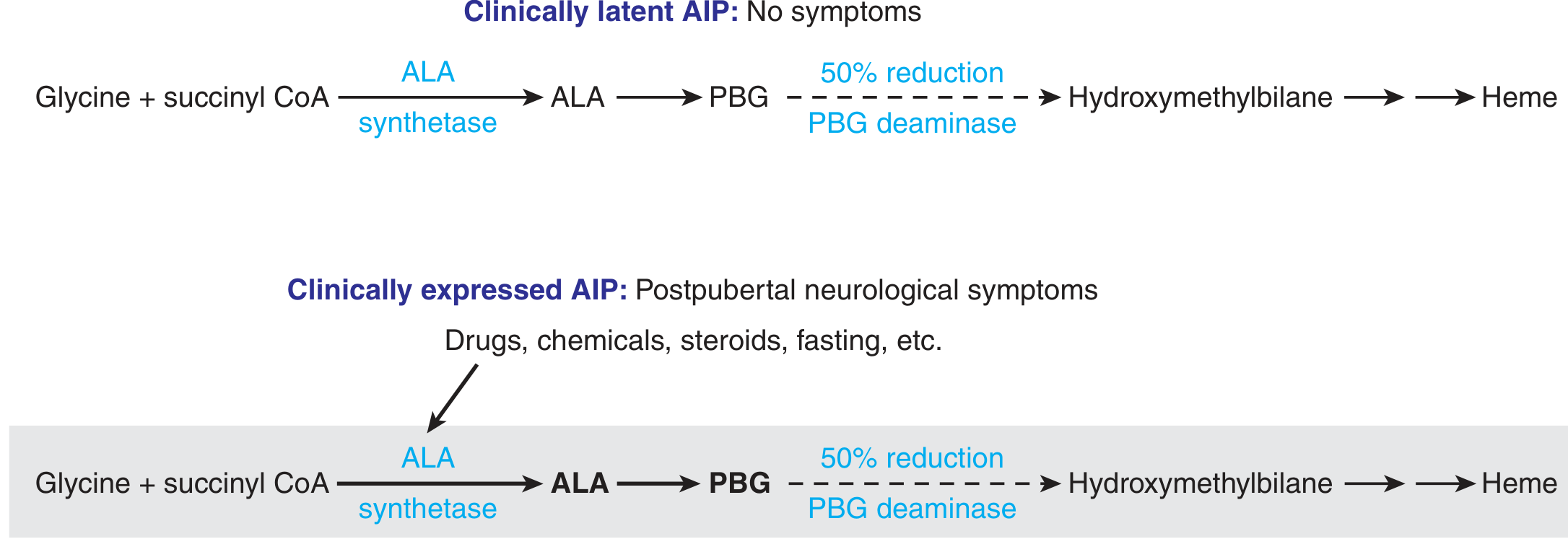
Under normal conditions, 50% PBG deaminase activity is adequate and the patient remains clinically latent (this accounts for ~90% of carriers throughout their lifetime). When a triggering agent (drugs, hormones, fasting) increases ALAS1 activity, ALA and PBG are produced in large amounts that the reduced PBG deaminase simply cannot process. ALA and PBG then accumulate to toxic levels in the liver, plasma, and urine.
4. Biochemical Basis of the Clinical Features
Abdominal Pain
Visceral and autonomic neurons are damaged by accumulated ALA and PBG. ALA structurally resembles GABA and can act as a GABA agonist/antagonist, disrupting normal neural signaling in autonomic ganglia. This causes disordered gut motility, visceral pain, nausea, vomiting, and constipation. Because the pain is neurogenic (not peritoneal), the abdomen is soft and imaging is normal.
Neuropsychiatric Features (anxiety, paranoia, hallucinations, psychosis)
The central nervous system is vulnerable to ALA neurotoxicity. ALA can enter the CNS and act at GABA-A receptors, disrupting inhibitory neurotransmission. This produces a spectrum from mild anxiety and behavioral change through to psychosis, confusion, hallucinations, and - in severe attacks - seizures and coma. The textbooks describe this as a "short-lived psychotic episode, which reverses completely with remission of the attack."
Autonomic Overactivity (tachycardia, hypertension)
Sustained activation of the sympathetic nervous system occurs, producing hypertension, tachycardia, and sweating. This can occasionally be severe enough to mimic a pheochromocytoma crisis.
Dark Urine
PBG and ALA are water-soluble and excreted in urine. On standing, PBG undergoes nonenzymatic conversion to the colored molecules porphobilin and uroporphyrin-I, causing the urine to turn dark red/brown - a hallmark of the acute attack.
Hyponatremia
Present in up to 40% of cases. The pattern suggests inappropriate renal salt wasting (SIADH-like), contributing to encephalopathy and seizures in severe attacks.
5. Why Did Birth Control Pills Trigger the Attack?
This is the key pharmacogenetic aspect of AIP:
The core mechanism:
Oral contraceptive pills (OCPs) contain synthetic estrogens and progestogens. These steroids are metabolized in the liver by cytochrome P450 (CYP) enzymes. The liver must synthesize additional CYP enzymes to handle this drug load.
The chain of events is:
- OCPs are introduced → the liver needs more CYP enzymes to metabolize them
- More CYP enzymes require more heme for their prosthetic groups
- This decreases the free heme pool in the hepatocyte
- Heme normally suppresses ALAS1 via feedback inhibition; when free heme falls, this inhibition is lifted
- ALAS1 is upregulated (induced) → massive increase in ALA and PBG synthesis
- The normal pathway would handle this by accelerating all downstream steps; but in this patient, PBG deaminase at step S3 is already only 50% functional
- The residual 50% enzyme activity is overwhelmed → ALA and PBG accumulate → acute attack
Additionally, the estrogen component itself directly induces ALAS1 transcription via nuclear hormone receptors in hepatocytes, independently of CYP demand. This is why AIP is:
- Rare before puberty
- More common in females
- Often cyclically linked to the luteal phase (high progesterone)
- Classically triggered by hormonal contraceptives
The fact that clinical disease is rare before puberty (endogenous sex hormones are low) and uncommon after menopause (hormones decline again) further confirms that steroid hormones are a major physiological inducer of ALAS1 in genetically predisposed individuals.
- Goldman-Cecil Medicine International Edition, p. 2316-2320
- Thompson & Thompson Genetics and Genomics in Medicine (9th ed.), p. 279
- Harrison's Principles of Internal Medicine (22E, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.