Do Research on " Variations in The Shape of The Stomach "
Reading File
search_medical_text
variations in the shape of the stomach anatomy
search_medical_text
stomach morphology types J-shape steer-horn orthotonic hypertonic
search_medical_image
stomach shape variations anatomy diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
gastric shape classification types position anatomical variation
search_medical_text
stomach parts anatomy fundus body pylorus greater lesser curvature
search_medical_image
stomach parts anatomy fundus body pylorus curvature
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive research summary on Variations in the Shape of the Stomach:
Variations in the Shape of the Stomach
1. Normal Gastric Anatomy (Baseline Reference)
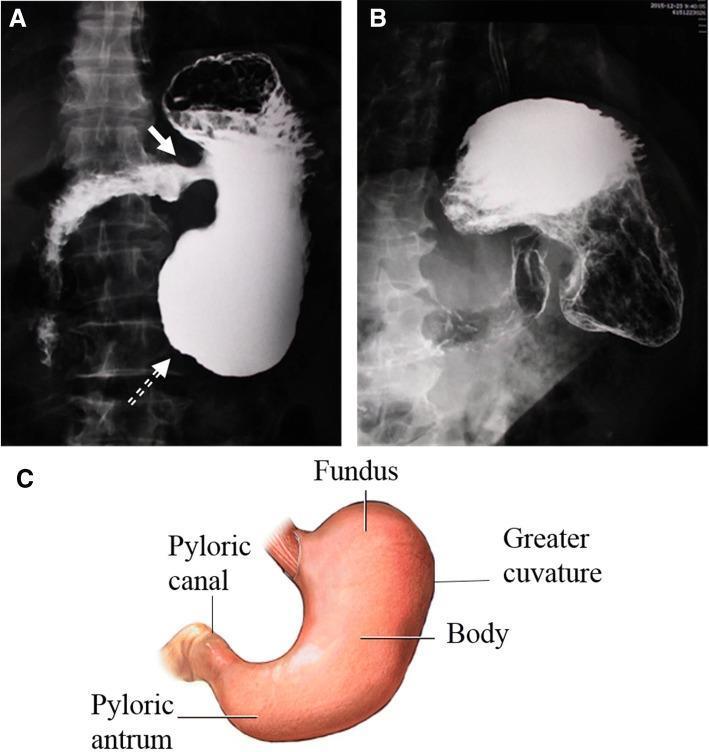
Before describing variations, understanding the standard anatomy is essential. The stomach is a J-shaped hollow viscus located in the left hypochondrium and epigastric region. Its key anatomical landmarks include:
| Region | Description |
|---|---|
| Cardia | Junction with the esophagus |
| Fundus | Dome-shaped superior portion, lies above the cardio-esophageal junction |
| Body (Corpus) | Main central portion |
| Pyloric Antrum | Distal funnel-shaped region |
| Pyloric Canal | Narrow channel leading to the duodenum |
| Greater Curvature | Long convex left border; receives gastroepiploic vessels |
| Lesser Curvature | Short concave right border; receives left and right gastric arteries |
The typical "J-shape" is considered the standard morphology in an upright adult (Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1169).
2. Classification of Gastric Shape Variations
Gastric shape is highly variable between individuals and is influenced by body habitus, posture, age, muscular tone, and degree of filling. The classic descriptive classification (used in radiological and gross anatomy) includes:
A. Orthotonic (J-shaped) Stomach — Most Common
- Resembles the letter "J"
- Found in individuals of average body build (mesomorphic)
- The pylorus lies at approximately the level of L1–L2
- The long axis is oblique, descending from left to right
- Most commonly depicted in anatomical textbooks
B. Hypertonic (Steer-Horn) Stomach
- Found in short, stocky (hypersthenic) individuals
- The stomach is high in position and nearly horizontal
- Resembles the shape of a bull's or steer's horn
- The pylorus is positioned higher, near L1
- The stomach appears wide and transverse with a high-riding fundus
- Common in obese individuals and infants
C. Hypotonic (Elongated / Cascade) Stomach
- Found in tall, thin (asthenic) individuals
- The stomach is elongated and descends low into the pelvis
- The pylorus may lie at L4–L5 or even lower
- Associated with ptosis (gastroptosis) — a sagging stomach
D. Atonic / Ptotic Stomach
- Extreme form of hypotonicity
- The stomach hangs very low, sometimes reaching the pelvis
- Associated with general visceroptosis and weak abdominal musculature
- More common in elderly or malnourished individuals
3. The Burdan Classification (Morphological Types)
A more detailed gross anatomical classification system — the Burdan classification — categorizes gastric shapes based on cadaveric and ex vivo studies:
| Type | Shape | Features |
|---|---|---|
| Type I | J-shaped (Standard) | Normal oblique orientation |
| Type II | Hook / Fishhook | Accentuated inferior loop at the pyloric end |
| Type III | Crescentic / C-shaped | Pronounced curvature along the longitudinal axis forming a distinct C or crescent |
| Type IV | Transverse / Steer-horn | Horizontal position, high pylorus |
| Type V | Cascade | Fundus folded posteriorly over the body |
The crescentic (Type III) variation is particularly notable — the organ exhibits a highly pronounced curvature with visible rugal surface wrinkles and remnant attachments of the greater and lesser omentum. This is a congenital and developmental variation studied in embryology and gastrointestinal topography.

4. Factors Influencing Gastric Shape
| Factor | Effect on Shape |
|---|---|
| Body habitus | Hypersthenic → steer-horn; Asthenic → elongated |
| Degree of filling | Empty stomach = contracted; Full stomach = globular expansion |
| Posture | Upright → J-shape; Supine → stomach shifts superiorly |
| Age | Infants have a more horizontal, hypertonic stomach; elderly may develop ptosis |
| Musculature & tone | High tone → compact shape; low tone → elongated/ptotic |
| Pregnancy | Gravid uterus displaces the stomach superiorly and to the left |
| Pathological conditions | Volvulus, linitis plastica, surgical alterations |
5. Cascade Stomach — A Special Variant
The cascade stomach is a normal variant where the fundus is folded posteriorly and overlies the body, creating a "cascade" appearance on barium studies. Features:
- The fundus fills first on barium swallow before spilling over ("cascading") into the body
- Often discovered incidentally on upper GI series
- Usually asymptomatic but may occasionally cause vague epigastric discomfort
- Must be distinguished from pathological posterior fundal masses
6. Pathological Shape Alterations (Distinguished from Normal Variants)
Some changes in gastric shape are due to disease:
| Condition | Shape Change |
|---|---|
| Linitis plastica (diffuse gastric carcinoma) | "Leather bottle" stomach — rigid, non-distensible, uniformly narrowed |
| Organoaxial volvulus | Stomach rotated along its long axis; pylorus displaced |
| Mesenteroaxial volvulus | Rotation around the mesenteric axis |
| Gastric outlet obstruction | Distended stomach with retained contents |
| Post-surgical (e.g., sleeve gastrectomy) | Tubular/sleeve shape after partial resection |
| Congenital pyloric stenosis | Hypertrophic pylorus causing distension of the proximal stomach |
7. Radiological Assessment of Gastric Shape
The shape of the stomach is best evaluated by:
- Barium Meal / Upper GI Series: Gold standard for demonstrating morphological variants — outlines rugal folds, curvatures, and mucosal pattern
- CT Abdomen: Cross-sectional assessment of position and relationship to surrounding organs
- Gastric Ultrasound: Used to assess the antrum and gastric content; patient positioning (right lateral decubitus at 0° or semi-recumbent at 45°) affects sonographic appearance significantly (Gastric Point-of-Care Ultrasound, p. 2)
- MRI: Useful in complex cases, especially for soft tissue characterization
8. Clinical Significance
Understanding gastric shape variations is important for:
- Surgical planning — e.g., gastric conduit construction in esophageal resection requires appreciation of the vascular arcade along the greater curvature (Bailey and Love's, p. 1169)
- Radiological interpretation — avoiding misdiagnosis of a normal variant as pathology (e.g., cascade stomach vs. posterior mass)
- Anesthesia / aspiration risk — gastric ultrasound assessment of content and position varies with body habitus
- Embryology and developmental studies — shape variants reflect different degrees of foregut rotation during development
- Laparoscopic procedures — trocar placement and visualization depend on gastric position and tone
Summary Table: Gastric Shape Variants at a Glance
| Variant | Body Type | Position | Key Feature |
|---|---|---|---|
| J-shaped (Orthotonic) | Mesomorphic | Oblique, moderate | Standard; most common |
| Steer-Horn (Hypertonic) | Hypersthenic | High, horizontal | Bull-horn appearance |
| Elongated (Hypotonic) | Asthenic | Low, vertical | Descends toward pelvis |
| Ptotic (Atonic) | Elderly/thin | Very low | May reach pelvis |
| Cascade | Any | Normal position | Fundus folds posteriorly |
| Crescentic (Type III) | — | Varies | Pronounced C-curvature |
The shape of the stomach is one of the most variable structures in human anatomy. Recognizing the spectrum — from normal physiological variants driven by body habitus and posture, to pathological alterations driven by disease — is fundamental to clinical anatomy, radiology, and surgery.
This is a shared conversation. Sign in to Orris to start your own chat.