• Gross splenomegaly, reaching up to left iliac fossa causing inferomedial displacement of left kidney, medial displacement of jejunal loops and posterior displacement of transverse colon. Anteriorly enlarged spleen is seen abutting the anterior abdominal wall. • Large wedge shaped hypodense non-enhancing area in mid-region of spleen - Infarct. - Splenic vessels shows normal contrast opacification. • Splenic vein is tortuous in course. • Cholelithiasis. No features of cholecystitis. • Minimal left pleural effusion with minimal basal atelectatic changes. This is a cect abdomen report of a 68 year old female suggest evaluation and treatment strategy
gross splenomegaly causes evaluation workup elderly
splenic infarct causes management treatment
myeloproliferative neoplasm splenomegaly myelofibrosis diagnosis treatment
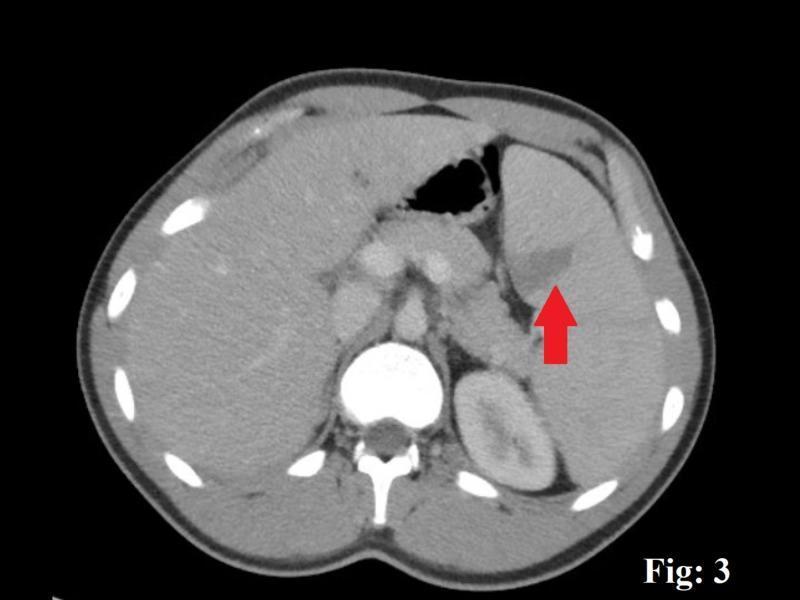
splenic infarct CT scan hypodense wedge shaped splenomegaly
CECT Abdomen — Interpretation & Management Plan
Summary of Key Findings
| Finding | Significance |
|---|---|
| Gross splenomegaly reaching left iliac fossa | Massive — beyond "huge spleen" threshold (>22 cm) |
| Wedge-shaped hypodense non-enhancing mid-splenic area | Splenic infarct (characteristic CT appearance) |
| Normal splenic vessel opacification | No proximal arterial/venous occlusion seen |
| Tortuous splenic vein | Suggests portal hypertension OR long-standing splenomegaly |
| Cholelithiasis, no cholecystitis | Possibly hemolysis-related pigment stones |
| Minimal left pleural effusion + basal atelectasis | Reactive — mechanical compression from massive spleen |
The Central Question: What is Causing Gross Splenomegaly?
Priority Differential Diagnosis
-
Myeloproliferative Neoplasms (MPN)
- Primary Myelofibrosis (PMF) — commonest cause of truly massive splenomegaly
- Polycythemia Vera (PV)
- Essential Thrombocythemia (ET)
- CML (Chronic Myeloid Leukemia)
-
Lymphoproliferative Disease
- Non-Hodgkin Lymphoma (especially splenic marginal zone lymphoma)
- Chronic Lymphocytic Leukemia (CLL)
- Hairy Cell Leukemia
-
Portal Hypertension / Congestive Splenomegaly
- Cirrhosis with portal hypertension
- Non-cirrhotic portal fibrosis
- Visceral Leishmaniasis (Kala-azar) — endemic regions
- Storage diseases (Gaucher's) — though rare at 68 years
The co-existence of cholelithiasis raises the possibility of hemolytic component (pigment stones from chronic hemolysis in MPNs or hemolytic anemias).
The tortuous splenic vein suggests elevated portal pressure or long-standing splenic engorgement.
Immediate Evaluation Protocol
1. Laboratory Investigations (Urgent)
- CBC: look for leuco-erythroblastic picture (tear-drop cells = myelofibrosis), cytopenias (hypersplenism), leukocytosis (CML/leukemia), thrombocytosis (ET/PV)
- Peripheral blood smear: dacrocytes, nucleated RBCs, blasts
- Reticulocyte count
- LDH, uric acid (tumor burden / cell turnover)
- Liver function tests, bilirubin (direct vs indirect — hemolysis vs cholestasis)
- PT/INR, coagulation profile
- JAK2 V617F mutation — positive in ~95% PV, ~50% PMF and ET
- BCR-ABL1 (Philadelphia chromosome) — to rule out CML
- CALR, MPL mutations — if JAK2 negative (PMF/ET)
- Serum EPO level (elevated in secondary causes, suppressed in PV)
- Vitamin B12 (markedly elevated in CML/PV)
- Bone marrow aspiration + trephine biopsy — essential for definitive diagnosis of myelofibrosis (fibrosis grading MF-0 to MF-3), lymphoma, leukemia
- Serum protein electrophoresis (SPEP)
- Flow cytometry (lymphoproliferative disease)
- LDH, β2-microglobulin
- Viral serology: HBsAg, Anti-HCV, HIV (if portal hypertension suspected)
- Leishmania serology / rK39 strip test (if endemic area)
2. Imaging — Further Workup
- USG Doppler abdomen: Assess portal vein caliber, hepatic echotexture, flow direction — evaluate for portal hypertension; assess splenic vein thrombosis more carefully
- Upper GI Endoscopy: Screen for esophageal/gastric varices if portal hypertension is suspected
- PET-CT: If lymphoma is high on differential (staging + metabolic activity)
- Echocardiography: If cardiac source of emboli is considered for the infarct
3. Assess for Hypersplenism
- Sequestration-related cytopenias (anemia, thrombocytopenia, neutropenia) — guide transfusion needs and surgical decision-making
Splenic Infarct — Management
"Treatment is conservative and splenectomy should be considered only when a septic infarct causes an abscess."
Conservative Management:
- Analgesia: NSAIDs / opioids for left upper quadrant / left shoulder tip pain
- Hydration: Adequate IV/oral hydration
- Anticoagulation: Consider if thrombotic etiology suspected (thrombocytosis-driven microvascular occlusion in MPN), balanced against bleeding risk — hematology input essential
- Monitor for infarct expansion, abscess formation, or rupture (serial imaging if symptomatic)
Red Flags Warranting Urgent Re-imaging/Surgery:
- Fever with leukocytosis → septic infarct → abscess formation
- Sudden worsening pain → splenic rupture
- Hemodynamic instability
Splenomegaly — Treatment Strategy (After Diagnosis)
If Myelofibrosis (most likely cause of this degree of splenomegaly):
| Approach | Details |
|---|---|
| JAK inhibitors | Ruxolitinib (first-line for intermediate/high-risk MF) — reduces spleen size significantly, improves symptoms |
| Fedratinib / Pacritinib | Alternative JAK inhibitors |
| Allogeneic HSCT | Only curative option — evaluate eligibility in a 68-year-old (performance status, comorbidities) |
| Hydroxyurea | Cytoreduction, especially in MPN with leukocytosis/thrombocytosis |
| Splenectomy | High-risk at this spleen size; reserved for refractory symptomatic splenomegaly, severe cytopenias, transfusion dependence — perioperative mortality ~5-10% in MF |
| Splenic radiation | Palliative option if not fit for surgery |
If CML:
- Tyrosine kinase inhibitors (Imatinib, Dasatinib, Nilotinib) — dramatically reduce spleen size
If Lymphoma:
- Staging + chemotherapy per lymphoma subtype (R-CHOP, BR, etc.)
If Portal Hypertension / Congestive:
- Treat underlying liver disease
- TIPS or surgical shunting for refractory cases
- Variceal management
Cholelithiasis
- No immediate intervention needed (no cholecystitis features on CECT)
- Elective cholecystectomy can be planned concomitantly with splenectomy if surgery is undertaken — standard practice to avoid future biliary complications
- If pigment stones confirmed (hemolytic etiology), treating the underlying hematologic condition reduces further stone formation
Pleural Effusion / Atelectasis
- Mechanical, secondary to the massively enlarged spleen elevating the left diaphragm
- Will resolve with treatment of underlying cause / spleen size reduction
- No independent pleural intervention needed unless symptomatic dyspnea develops
Proposed Management Algorithm
CECT Findings
↓
Urgent CBC + Peripheral Smear + LFT + LDH
↓
┌────────────────────────────────────┐
│ Leuco-erythroblastic picture? │──Yes──→ Bone marrow biopsy
│ JAK2/BCR-ABL/CALR mutation? │ → Myeloproliferative workup
│ Lymphocytosis/Lymphadenopathy? │──Yes──→ Flow cytometry + PET-CT
│ Portal HTN features on Doppler? │──Yes──→ GI endoscopy + Hepatology ref
└────────────────────────────────────┘
↓
Hematology/Oncology referral (urgent)
↓
Treat underlying cause
↓
Reassess spleen size + infarct at 3 months
↓
Surgical planning (splenectomy ± cholecystectomy) if:
- Refractory cytopenias
- Failed medical therapy
- Abdominal discomfort/mechanical complications
Relevant CT Appearance — Splenic Infarct
Priority Actions Summary
- Urgent hematology referral — degree of splenomegaly mandates specialist evaluation
- CBC with smear + JAK2/BCR-ABL — within 24-48 hours
- Bone marrow biopsy — once hematology review complete
- Doppler USG abdomen — assess portal hemodynamics, splenic vein
- Conservative management of infarct — analgesia, monitor for complications
- Cholelithiasis — defer, manage electively
- Multidisciplinary team — Hematology, Surgery, Gastroenterology
⚠️ Clinical note: At this spleen size, the risk of spontaneous splenic rupture is non-trivial. The patient should be counseled to avoid contact activities and return immediately for acute left-sided pain. Any planned procedures (including biopsy) should account for thrombocytopenia/coagulopathy risk.