thyroid gland overview
Reading File
Finding Sources
Searching the Web
thyroid gland anatomy physiology hormones overview
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have everything needed for a thorough overview. Here is the complete response:
Thyroid Gland - Overview
1. Anatomy
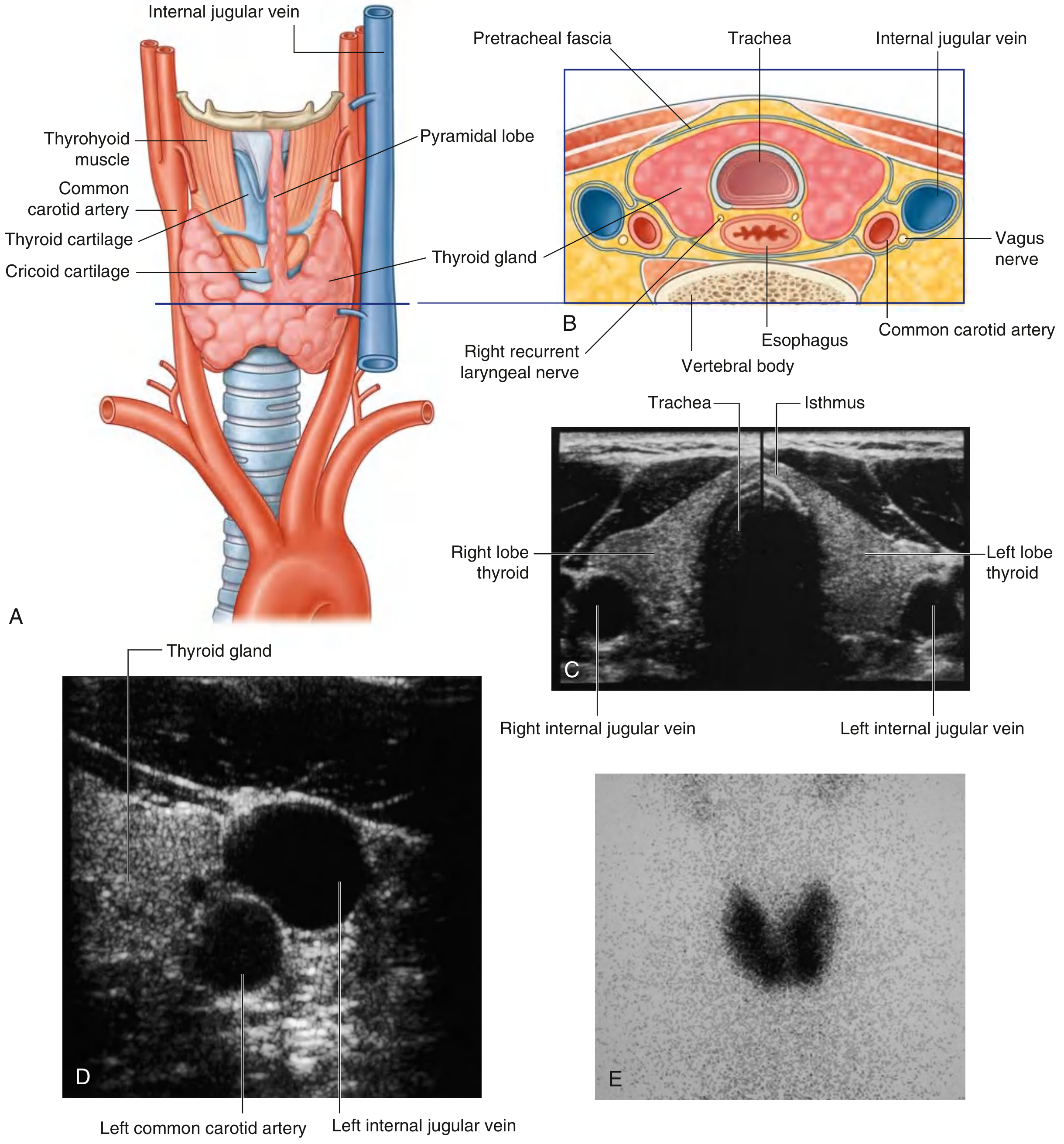
The thyroid is a butterfly-shaped endocrine gland located in the anterior neck, inferior to the larynx and anterior to the trachea. It overlies cervical levels C5-T1.
Gross structure:
- Two lateral lobes connected by a narrow isthmus, which crosses anterior to the 2nd and 3rd tracheal cartilages
- The lobes cover the anterolateral surfaces of the trachea, the cricoid cartilage, and the lower thyroid cartilage
- A pyramidal lobe may extend superiorly from the isthmus in ~50% of individuals, representing a remnant of the thyroglossal duct
- Lies deep to the strap muscles (sternohyoid, sternothyroid, and omohyoid) within the visceral (pretracheal) compartment
2. Embryology
The thyroid develops from an endodermal evagination of the pharyngeal floor (foramen cecum at the base of the tongue) and descends along the thyroglossal duct to its final position in the anterior neck. The thyroglossal duct normally obliterates; remnants can persist as:
- A thyroglossal duct cyst (midline neck mass)
- A lingual thyroid (ectopic functional thyroid at the base of tongue)
- A fistula connecting to the foramen cecum
Parafollicular C cells originate from the neural crest (via the ultimobranchial body), not from endoderm.
- Gray's Anatomy for Students, p. 1157
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 994
3. Vasculature
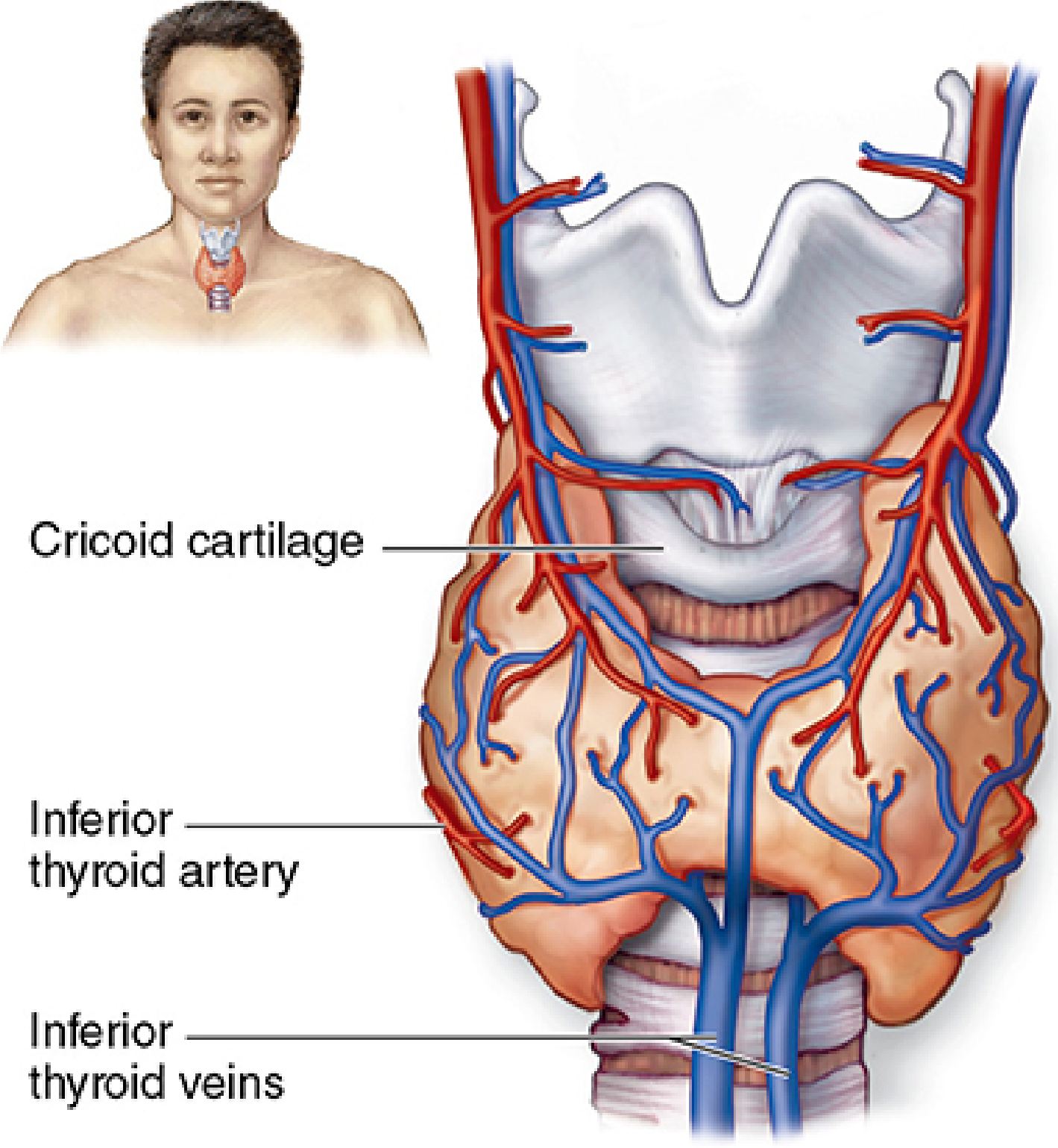
| Vessel | Origin | Notes |
|---|---|---|
| Superior thyroid artery | First branch of external carotid artery | Descends along the thyrohyoid muscle to the superior pole; anterior branch anastomoses across the isthmus with its contralateral twin |
| Inferior thyroid artery | Thyrocervical trunk (from subclavian artery) | Passes posterior to the carotid sheath; closely related to the recurrent laryngeal nerve - surgically important |
| Superior thyroid vein | Drains upper pole | Tributary of internal jugular vein |
| Middle thyroid vein | Drains lateral gland | Tributary of internal jugular vein |
| Inferior thyroid veins | Drain lower pole | Drain into left brachiocephalic vein |
| Thyroidea ima artery | Aortic arch or brachiocephalic (variable) | Present in ~10%; can bleed during tracheotomy |
Important surgical relationship: The recurrent laryngeal nerve (RLN) runs in the groove between the trachea and esophagus and is at risk during inferior thyroid artery ligation in thyroidectomy.
- Gray's Anatomy for Students, p. 1158
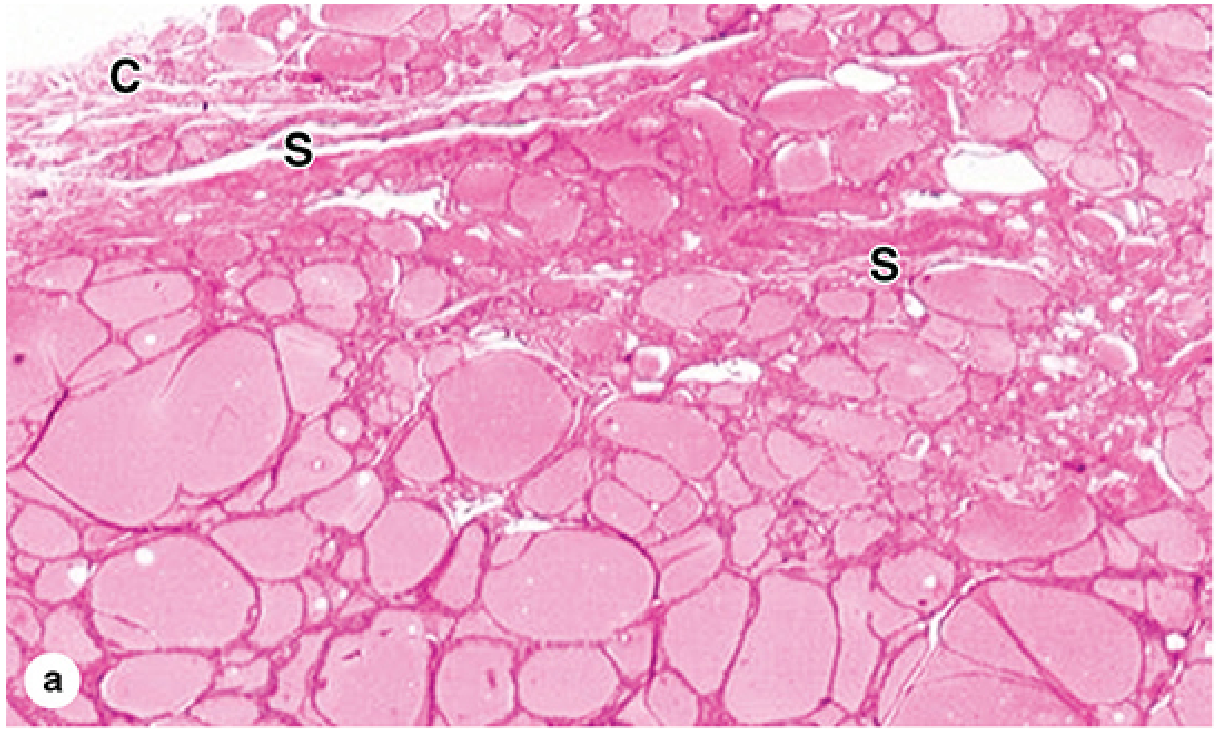
4. Histology
The thyroid is covered by a fibrous capsule that sends septa inward, dividing it into lobules and carrying blood vessels, nerves, and lymphatics.
Follicular units: Each lobule contains 20-40 colloid-filled follicles. Key features:
| Feature | Detail |
|---|---|
| Follicular cell (thyrocyte) shape | Squamous (inactive) to low columnar (active) - controlled by TSH |
| Colloid | Gelatinous, acidophilic; contains thyroglobulin (660 kDa glycoprotein) - the hormone precursor |
| Hormone storage | The thyroid is unique among endocrine glands: large quantities of secretory product are stored extracellularly in follicle lumens (up to 3 months' supply) |
| Stroma | Sparse reticular connective tissue with fenestrated capillaries for rapid hormone transfer |
Two cell populations:
- Follicular cells (thyrocytes) - synthesize T3 and T4
- Parafollicular cells (C cells) - scattered between follicles or within the follicular epithelium; synthesize calcitonin
- Junqueira's Basic Histology, p. 1034-1035
5. Hormone Synthesis and Regulation
Hypothalamus-Pituitary-Thyroid (HPT) Axis
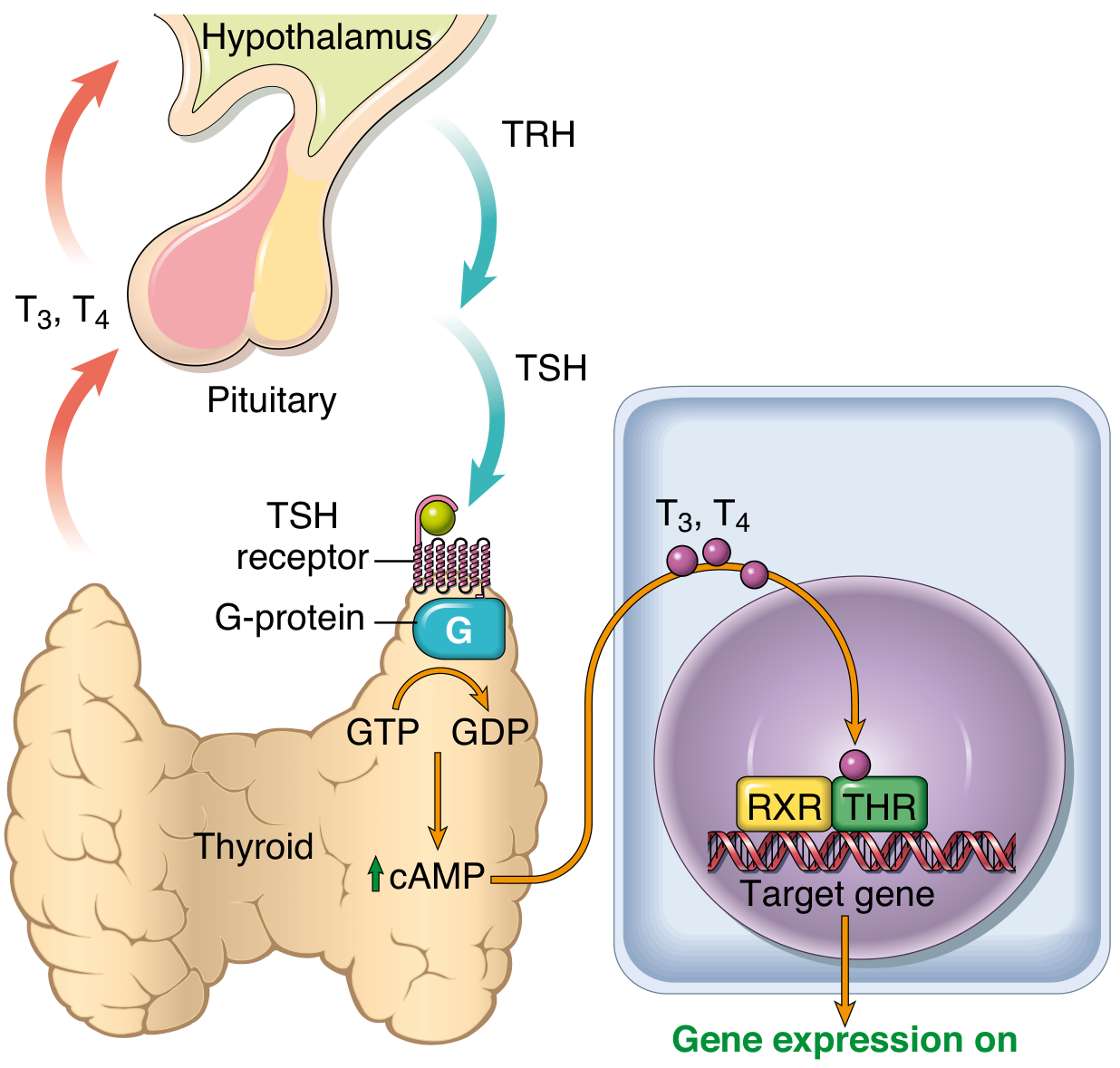
Steps:
- TRH (thyrotropin-releasing hormone) is secreted from the paraventricular nucleus of the hypothalamus
- TRH stimulates anterior pituitary thyrotrophs to release TSH (thyroid-stimulating hormone)
- TSH binds its receptor on follicular cells → activates Gs protein → ↑ cAMP → stimulates thyroid growth and hormone synthesis and release
- Negative feedback: Rising T3/T4 suppress both TRH (hypothalamus) and TSH (pituitary)
Thyroid Hormone Synthesis Steps (within the follicular cell):
- Iodide trapping - active Na+/I- symporter (NIS) concentrates iodide
- Oxidation - thyroid peroxidase (TPO) oxidizes I- to I2 (reactive iodine)
- Organification - I2 is incorporated onto tyrosine residues of thyroglobulin → monoiodotyrosine (MIT) and diiodotyrosine (DIT)
- Coupling - DIT + DIT → T4; MIT + DIT → T3 (within thyroglobulin stored as colloid)
- Secretion - Follicular cells endocytose colloid; lysosomes cleave T3/T4 from thyroglobulin; free hormones are secreted into capillaries
Circulating Hormones:
-
Most T3 and T4 travel bound to thyroxine-binding globulin (TBG), transthyretin, and albumin
-
Only free (unbound) hormone is biologically active
-
~80% of circulating T3 is produced by peripheral deiodination of T4 (primarily in liver and kidney)
-
T3 has ~10x greater receptor affinity than T4 and is the more potent hormone
-
Robbins, Cotran & Kumar, p. 994-996
6. Actions of Thyroid Hormones (T3/T4)
T3/T4 bind nuclear thyroid hormone receptors (THR-alpha and THR-beta), which heterodimerize with RXR and bind thyroid response elements (TREs) to regulate gene transcription. Major effects:
| System | Effect |
|---|---|
| Metabolism | Increases basal metabolic rate; stimulates carbohydrate and lipid catabolism; promotes protein synthesis |
| Cardiovascular | Increases heart rate and cardiac output; potentiates catecholamine sensitivity |
| Nervous system | Required for normal brain development in fetus and neonate (critical window) |
| Skeletal | Promotes normal bone growth and maturation |
| Thermogenesis | Increases heat production via uncoupling of oxidative phosphorylation |
7. Calcitonin (C cells)
- Secreted by parafollicular (C) cells
- Opposes PTH: promotes calcium deposition into bone; inhibits osteoclast-mediated bone resorption
- Results: lowers serum calcium
- Clinically: C cell hyperplasia and medullary thyroid carcinoma (MTC) arise from these cells; MTC is associated with MEN2A and MEN2B (RET proto-oncogene mutations)
8. Clinical Relevance - Common Disorders
| Category | Examples |
|---|---|
| Hyperthyroidism / Thyrotoxicosis | Graves' disease (TSH-receptor autoantibodies), toxic multinodular goiter, toxic adenoma |
| Hypothyroidism | Hashimoto's thyroiditis (most common in iodine-sufficient regions), iodine deficiency (most common worldwide), iatrogenic (post-thyroidectomy/radioiodine) |
| Goiter | Enlargement from TSH stimulation (iodine deficiency, goitrogens like propylthiouracil and methimazole) |
| Thyroid nodules/neoplasms | Papillary carcinoma (most common), follicular carcinoma, medullary carcinoma, anaplastic carcinoma |
Goitrogens - agents that suppress thyroid hormone synthesis, leading to compensatory TSH elevation and glandular enlargement:
- Propylthiouracil (PTU) - inhibits TPO (oxidation) and peripheral T4→T3 conversion
- Methimazole - inhibits TPO
- Large doses of iodide (Wolff-Chaikoff effect) - blocks hormone release acutely
Sources:
- Gray's Anatomy for Students (9780323934237)
- Junqueira's Basic Histology - Text and Atlas, 17e (9781264930395)
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (9780443264528)
This is a shared conversation. Sign in to Orris to start your own chat.